

Obscure gastrointestinal bleeding (OGIB) is defined as occult bleeding or it manifests as bleeding of unknown origin after negative endoscopy and colonoscopy. OGIB can present as occult bleeding characterized by anemia, iron deficiency and/or fecal occult blood, or it can manifest as hematochezia or melena, with no evidence of the bleeding site through conventional studies. Approximately 5% of gastrointestinal bleeding occurs between the Treitz ligament and the ileocecal valve.1 Diagnosis and treatment of patients with OGIB are often long and difficult processes.2 Capsule endoscopy (CE) has been shown to be a cornerstone in evaluating the patient with OGIB. The benefits of CE include the fact that it is a painless, invasive method that is widely accepted by the patient for studying the small bowel (SB).1 All the patient has to do is swallow the capsule endoscope. Despite its being a minimally invasive method, several complications must be taken into account, such as retention of the capsule endoscope (0.7%), impaction in the cricopharyngeus or diverticula, and aspiration into the respiratory tract.3–8 Only a few cases of capsule endoscope aspiration have been reported worldwide 6–8 and none in Mexico. Therefore, we believe it is of interest to report the present case, so that the physicians carrying out this type of study are aware of this possible complication.
A 78-year-old man had no past history of chronic degenerative diseases and no complaints of dysphagia or swallowing disorders. He was hospitalized 3 years prior due to upper gastrointestinal bleeding from a gastric ulcer secondary to NSAID ingestion for which he received satisfactory combined endoscopic treatment. He continued with occasional NSAID ingestion. One year ago the patient began to present with postprandial fullness, a weight loss of 14kg during that year, and fecal occult blood on 2 occasions. Panendoscopy revealed a hiatal hernia and chronic gastropathy of the body and antrum. Colonoscopy showed uncomplicated diverticular disease of the descending colon and the sigmoid colon. The patient was referred for CE as part of the approach to OGIB. A bowel transit time test was done on the patient before he was given the capsule endoscope to swallow, and it was normal. There were no complications in relation to the preparation for CE.
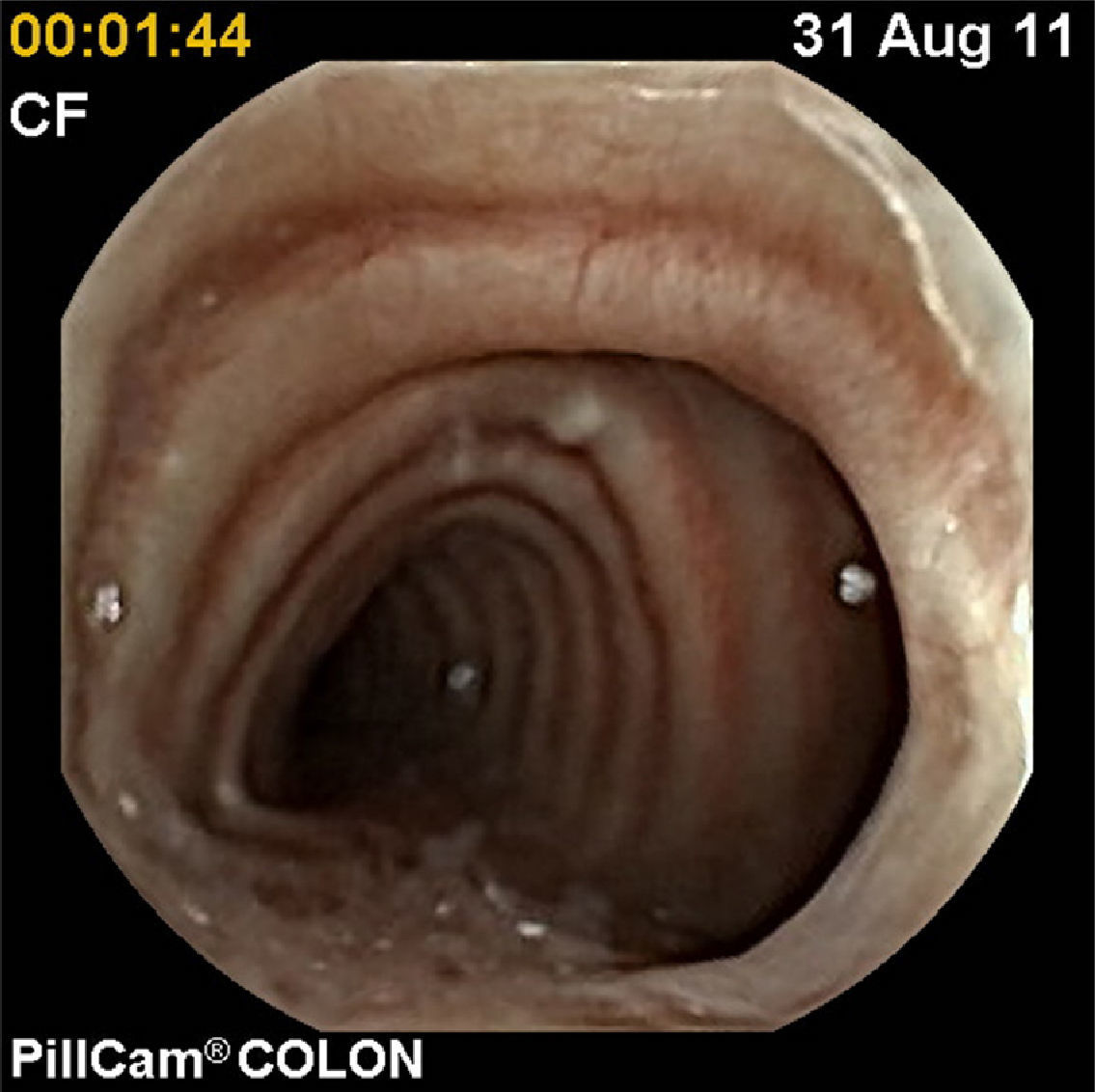
The patient was programmed for the CE study with the modified PillCam COLON 1 technique for studying the SB. The patient had some difficulty in swallowing the capsule endoscope, but he was able to do so. Immediately after swallowing it he had the sensation of a foreign body in his throat and a coughing spell of 2min. He did not complain of dyspnea or any other symptom and physical examination showed no cyanosis. He drank water again and had the sensation of having swallowed the capsule. However, one minute later his cough was exacerbated and he expelled the capsule into his mouth. He was given water, he swallowed the capsule with no incident, and the study was completed with no apparent complication. The images were downloaded and when the study was examined, it was seen that the capsule had been aspirated, taking photograms of the respiratory tract (figs. 1 and 2); the capsule was then expelled into the mouth and swallowed again, evaluating the usual trajectory in its entirety. The capsule was passed 8hours later and the cause of the bleeding was identified.


CE has currently become the method of choice for studying the patient with OGIB. It has been approved in the United States by the Food and Drug Administration for the study of these patients, and it is also indicated in the study of Crohn's disease and polyps, among others.9
The present case showed the aspiration of a capsule endoscope and the successful and non-invasive recovery of the patient. The first reported case of aspiration required surgical extraction,8 in another published case extraction was carried out through rigid bronchoscopy, using a foreign body forceps and basket, 7 and in another, the patient did not require any invasive recovery procedure,6 as with our case. Our patient did not present with the classic symptoms of acute aspiration or any symptom of respiratory distress.
Some patients, especially older adults or patients with neurologic diseases, may experience the sensation of a foreign body in the chest after swallowing the capsule, without their actually having aspirated it.7
We should be aware of the complications that may arise and how to manage them. In addition, every study should be done in real time, because it is a useful study tool that evaluates the passage of the capsule endoscope into the digestive tract, aiding us in knowing where it is located. We have performed over 200 studies without having a complication of this type. We should thoroughly question the patient, emphasizing swallowing disorders, and if there are any, carry out complementary imaging studies before the capsule endoscope is swallowed. In the presence of a swallowing disorder, the capsule endoscope should be guided by endoscopy to avoid this complication.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Sánchez-Chávez X, Martínez-García C. Aspiración de cápsula endoscópica: ¿complicación frecuente?. 2013;78:257–258.

