
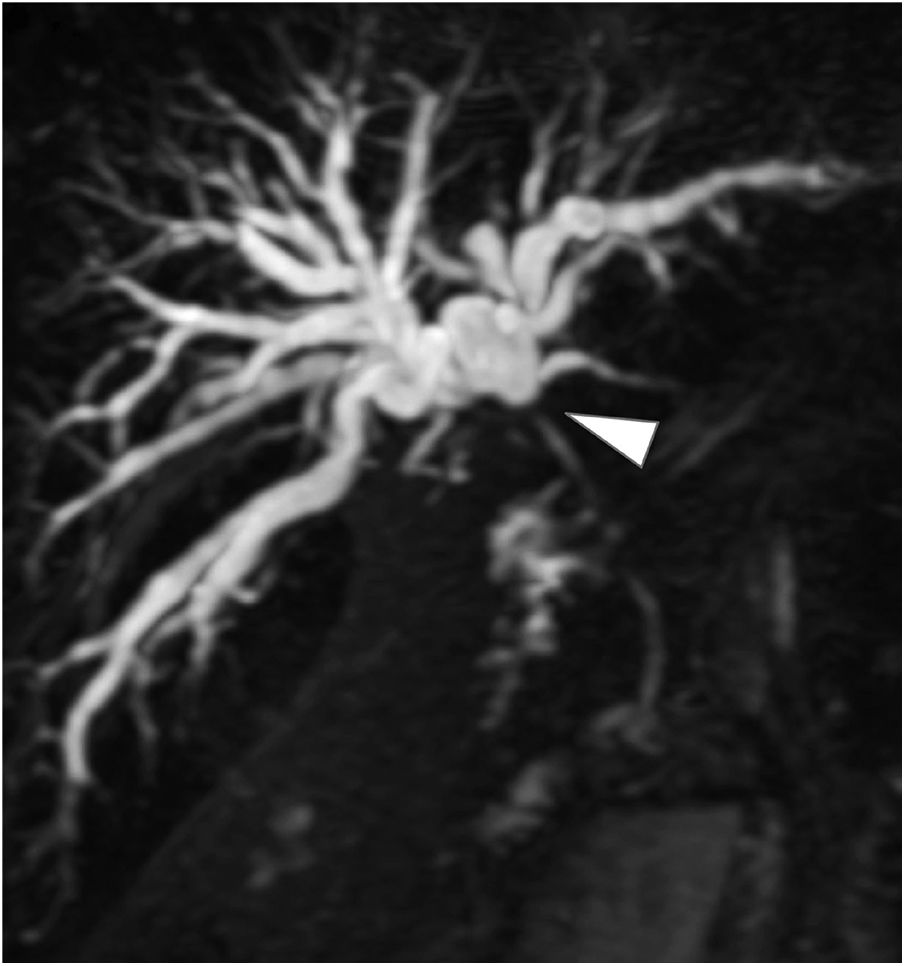
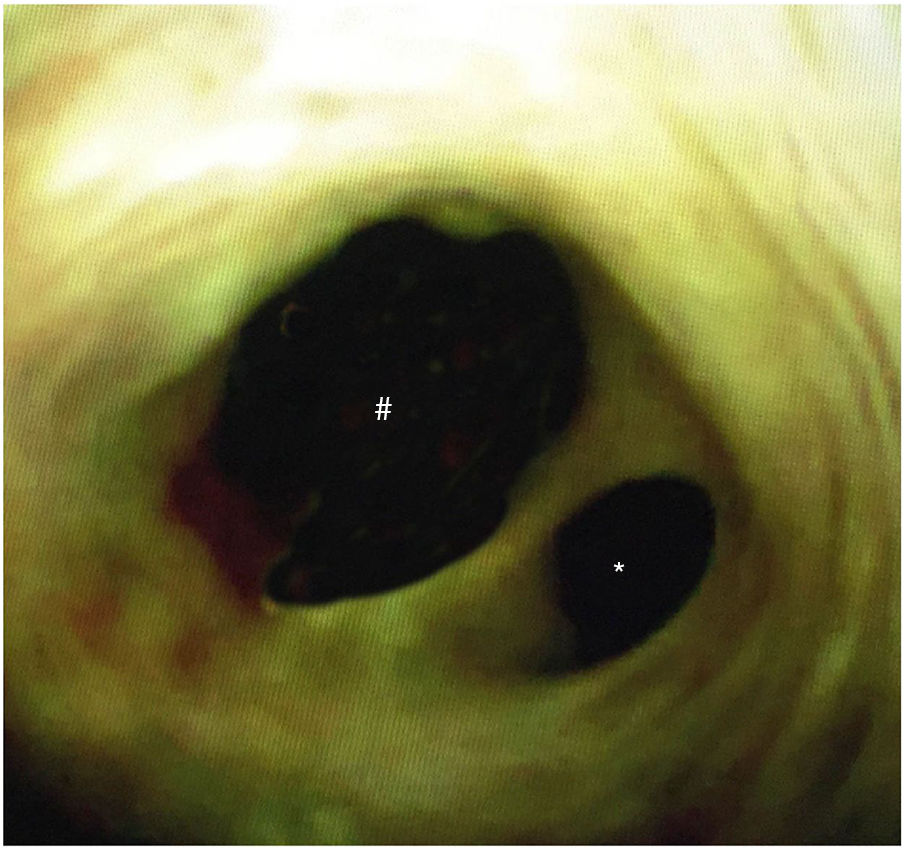
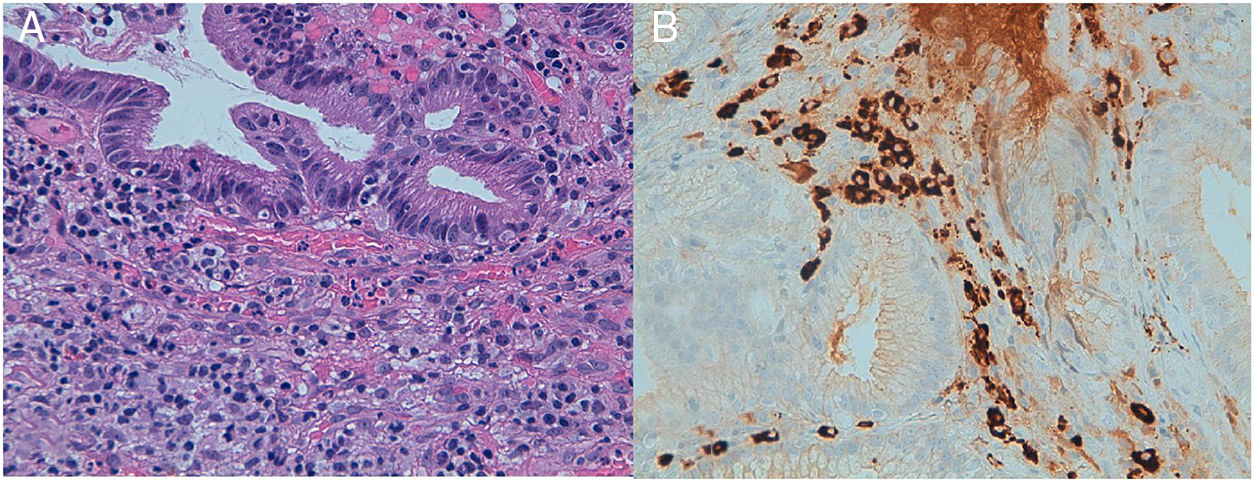
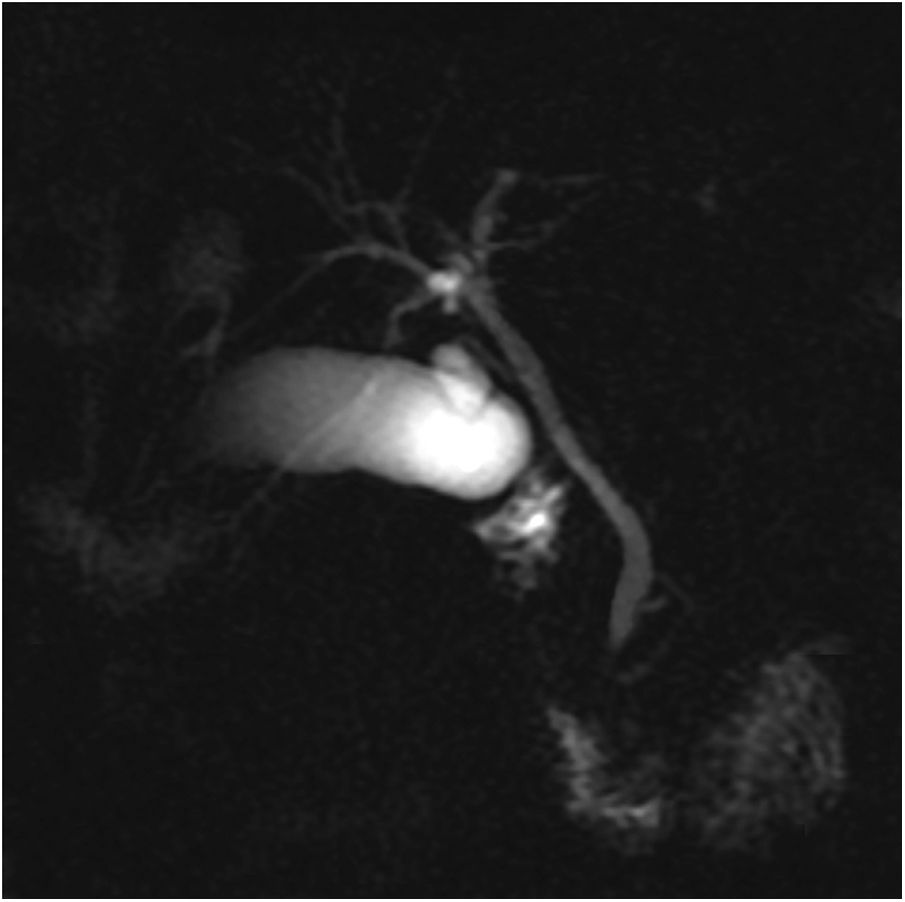
A 51-year-old man was evaluated for obstructive jaundice associated with mild dyspepsia. He had an unremarkable past medical history and physical examination revealed no significant findings except for jaundice. Laboratory test results showed altered liver enzymes (total bilirubin 20.1mg/dl, direct bilirubin 18.8mg/dl, AST 53U/l, ALT 144 U/l, GGT 386 U/l, ALP 203 U/l). A computed tomography (CT) scan and subsequent magnetic resonance cholangiopancreatography (MRCP) demonstrated a 1.2cm hilar mass, which constituted hilar stricture and occlusion of the biliary tract and its dilation in the intrahepatic area (fig. 1), suggesting hilar cholangiocarcinoma (Bismuth-Corlette II). Percutaneous cholangiography for internal-external biliary drainage confirmed the hilar stricture (fig. 2A); cholangiography performed 10 days later showed its normalization (fig. 2B). The patient underwent cholangioscopy that confirmed a normal biliary duct at the hilum (fig. 3) and endobiliary forceps biopsies were taken in the same session. The histopathologic evaluation revealed transmural chronic inflammatory cell infiltrates, with no signs of malignancy. Immunohistochemical staining showed IgG4-positive plasma cells (figs. 4 A and B). MRCP at 6 months confirmed a normal biliary tree (fig. 5).
 reconstruction showing biliary tract occlusion due to a hilar stricture (arrowhead) and dilation of the intrahepatic biliary tree.")
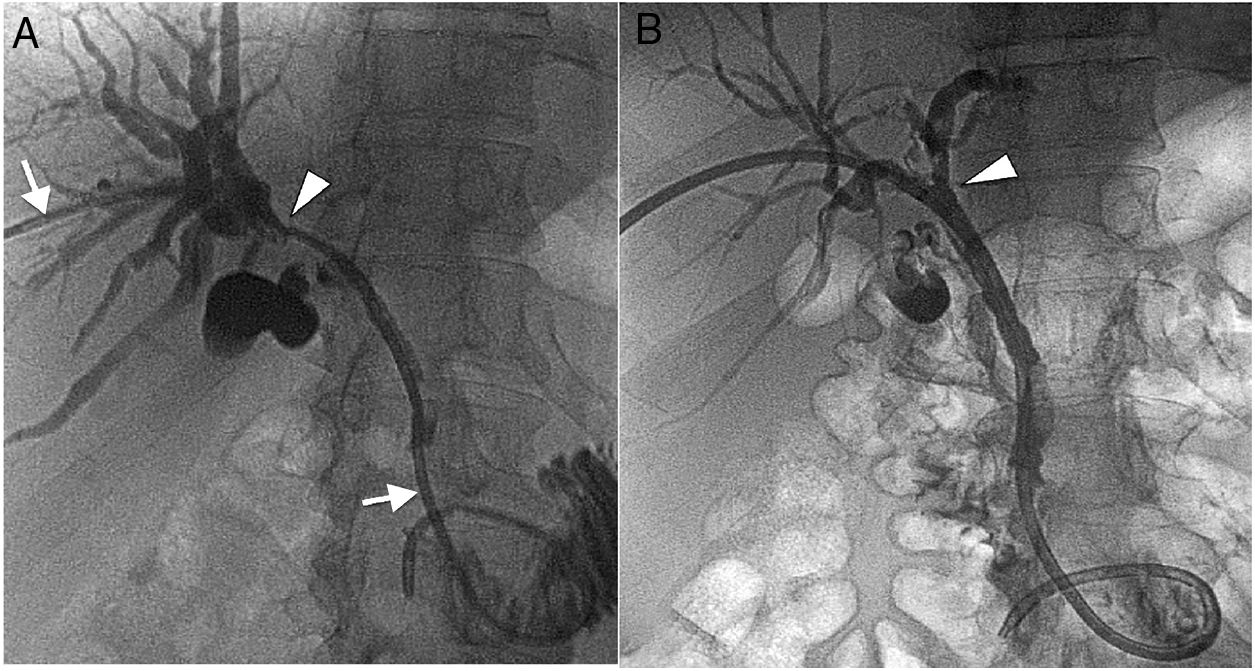
 Cholangiography for percutaneous internal-external biliary drainage (arrows) confirming a hilar stricture (arrowhead). B) Cholangiography at 10 days shows a normalized situation, with no more hilar stricture (arrowhead).")
 and left (*) hepatic biliary duct.")

 reconstruction showing a normal biliary tree.")
No financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Barberis A, Rossi UG, Filauro M. Colangitis imitando al colangiocarcinoma hiliar. Revista de Gastroenterología de México. 2019;84:245–247.

