
A 40-year-old woman, smoker, with no chronic degenerative diseases, underwent laparoscopic fenestration of a simple hepatic cyst in segment V in 2012.
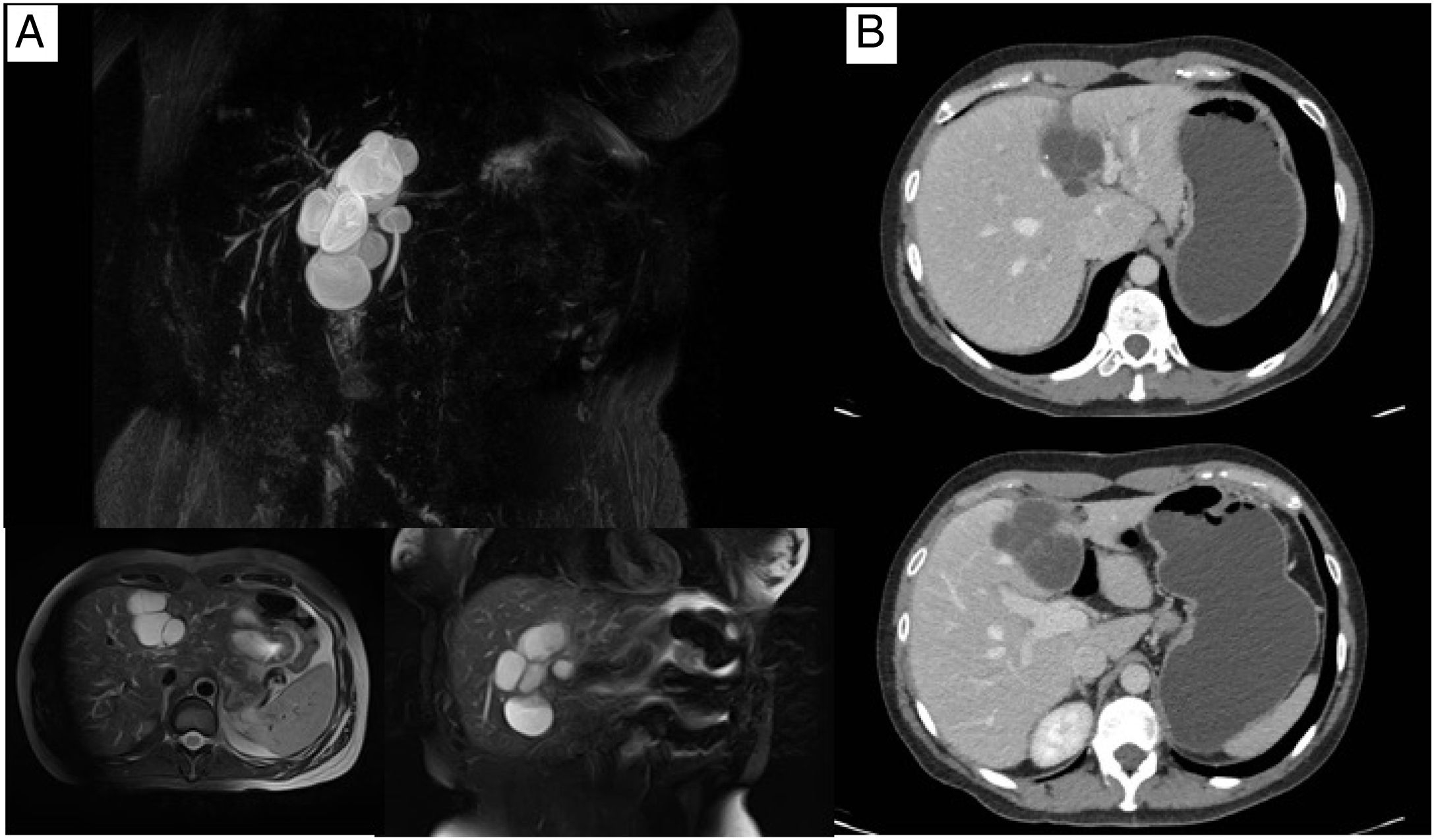
She continued to have follow-up until 2019, when a new abdominal ultrasound showed images suggestive of cystic lesions dependent on the common bile duct. A magnetic cholangioresonance study identified an image consistent with biliary cystadenoma in segment IV (Fig. 1A). The approach was complemented with triphasic abdominal tomography that reported the same findings (Fig. 1B).
 Magnetic resonance imaging and B) axial tomography, both showing the lesion suggestive of biliary cystadenoma in liver segment IV.")
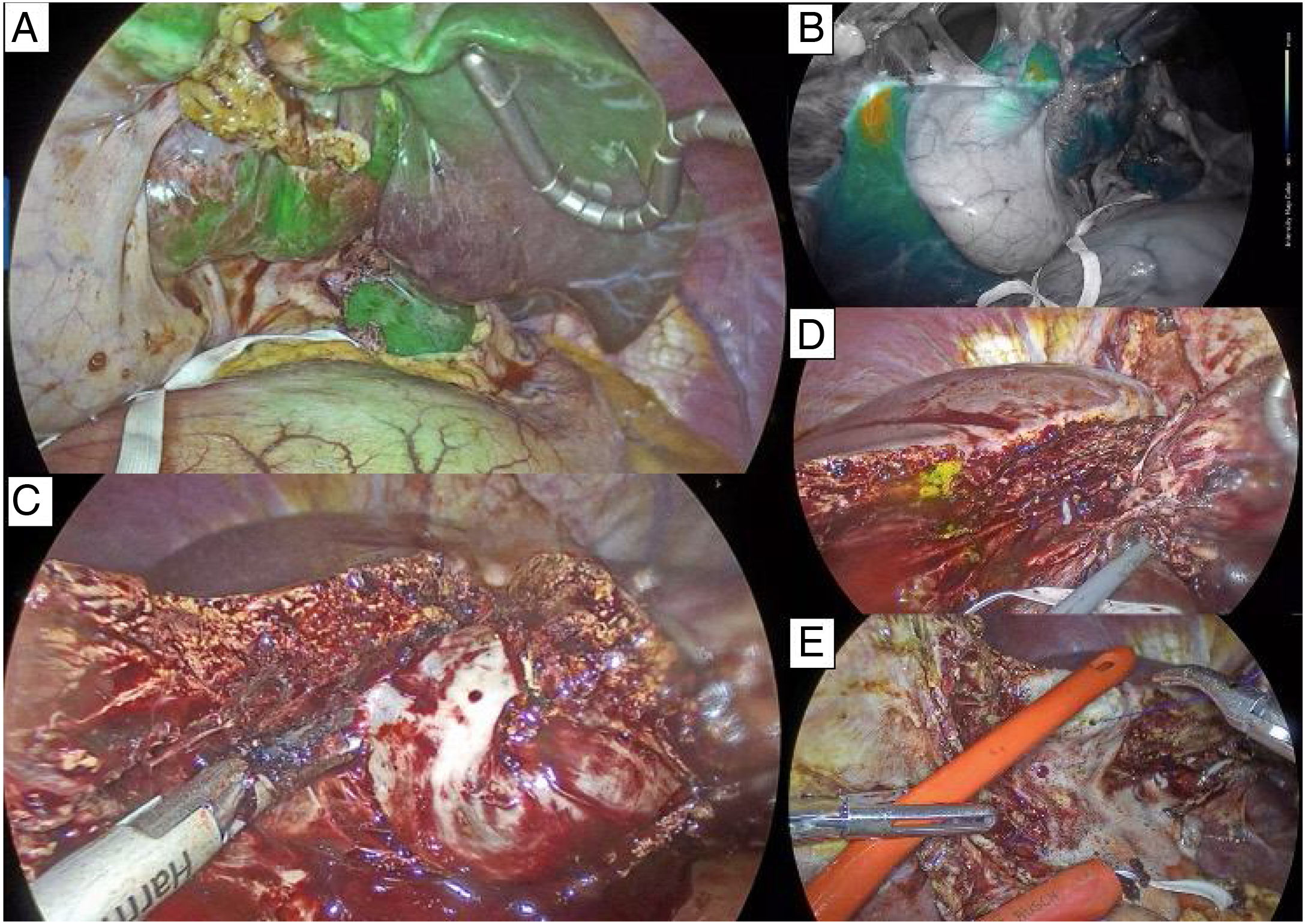
The patient was considered a candidate for laparoscopic indocyanine green (ICG)-assisted left hepatectomy with resection. For the surgical procedure, she was put in the French position and 5 ports were utilized. A band was placed around the hepatic hilum, as preparation for the Pringle maneuver, if required. Dissection began at the hilum to identify the left hepatic artery, which was ligated with a clip and cut. The left branch of the portal vein, which was displaced by the lesion, was then identified and ligated using a vascular stapler. Intravenous ICG (3ml) was injected and the fluorescence imaging filter was activated (Karl Storz Image 1 S NIR/ICG equipment), observing only the absence of drug uptake in segment II (Fig. 2A). The portal vein branch of segment III was identified and ligated again with the stapler. The uptake intensity filter was then activated, and less uptake in the left hepatic lobe was observed (Fig. 2B). Given that the lesion took up all of segment IVb, cholecystectomy was required, so that the transection plane at the level of the middle suprahepatic vein could be detected. After the cholecystectomy, the transection of the liver parenchyma was started to the right of the lesion with ultrasound energy, separating the parenchymal lesion from segment V through blunt dissection. The middle suprahepatic vein was identified and preserved (Figs. 2C and D). The biliary-portal left intrahepatic pedicle was ligated with the vascular stapler, as was the union of the left suprahepatic vein with the vena cava. The specimen was extracted through a 7cm Pfannenstiel incision. The hepatic hilum band was released, with no need to perform the Pringle maneuver during the procedure. Finally, the absence of bile leakage was confirmed using oxygenated water (Fig. 2E).
 ICG filter, showing drug uptake in segment II. B) Uptake intensity filter with higher drug concentration in the right hepatic lobe. C) Transection of the hepatic parenchyma to the right of the lesion, following the trajectory of the middle suprahepatic vein, distinguishing the resection as a formal (major) left hepatectomy. D) Biliary leakage after the resection. E) Absence of bile leakage confirmed, using oxygenated water after suture placement (cross-stitch) at the leakage site.")
A) ICG filter, showing drug uptake in segment II. B) Uptake intensity filter with higher drug concentration in the right hepatic lobe. C) Transection of the hepatic parenchyma to the right of the lesion, following the trajectory of the middle suprahepatic vein, distinguishing the resection as a formal (major) left hepatectomy. D) Biliary leakage after the resection. E) Absence of bile leakage confirmed, using oxygenated water after suture placement (cross-stitch) at the leakage site.
Surgery duration was 5h, with blood loss of 300ml. No blood transfusions were necessary. The patient had satisfactory progression, with no signs of systemic inflammatory response and with adequate pain control. Oral diet was resumed on postoperative day one and the patient was released on day 3. Histopathologic study confirmed the diagnosis of biliary mucinous cystadenoma.
Biliary cystadenomas are rare cystic tumors (less than 5% of all cystic lesions of the liver). There are two histopathologic types: mucinous and serous. The mucinous type is predominant and presents in women between the fourth and sixth decades of life. Surgical resection is recommended due to their recurrence capacity and potential malignization.1,2
The majority of cases of laparoscopic liver surgery have been limited to the fenestration of cystic lesions, staging of malignant tumors, and diagnosis of trauma lesions. Liver resection has mainly been employed in benign lesions smaller than 5cm and located in the anterior segments of the right liver lobe and in the left liver lobe.3,4
In Mexico, there are only 2 articles on laparoscopic hepatectomy. Both describe cases of left lateral hepatectomy due to focal nodular hyperplasia. The postoperative results were good, and the patients were released before postoperative day 5. Those authors concluded that the surgery is safe in our environment, as long as the infrastructure is appropriate and the surgeons are experienced.5,6 Nevertheless, there are no reports in Mexico on major laparoscopic hepatectomies.
Likewise, ours is the first Mexican report on ICG-assisted liver resection. Multiple ICG applications are possible in liver surgery, as well as the moments at which the dye can be infused. It is a fluorescent, water-soluble coloring substance that is excreted in bile, without being metabolized. It is of special help to surgeons for determining tumor extension and in tumors that cannot be directly palpated in laparoscopic procedures.7–9 In our case, we decided to perform the infusion intraoperatively, with the intention of observing the perfusion in the right liver and the absence of perfusion in the left liver, to facilitate detecting the transection plane. However, given the position of the lesion, it was not possible to ligate the complete left portal pedicle on the first attempt, resulting in the ligation of only the portal branch of segment II, with segmental hypoperfusion. When the branch of segment III was later ligated, the result was a lower concentration of the drug in the left hemi-liver, compared with the right.
Ethical disclosuresThe authors declare that the patient signed a statement of informed consent, conforming with the policies and regulations of our institutional ethics committee. The present article contains no personal information that could identify the patient and no experiments were conducted on humans or animals.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Rueda de León A, González-Espinoza KA, Cisneros-Correa J, del Ángel-Millán G, Domínguez-Rosado I. Hepatectomía izquierda totalmente laparoscópica por cistoadenoma biliar mucinoso. Revista de Gastroenterología de México. 2021;86:208–210.

