
Enteric perforations and fistulas are difficult to manage due to comorbidities, poor nutritional status, and anatomic challenges related to multiple interventions in those patients. The use of endoscopic methods as a nonsurgical approach is increasing. The aim of the present study was to describe the clinical experience with the use of the Ovesco Over-The-Scope Clip system in the closure of perforations, fistulas, and other indications in the digestive tract at a tertiary care hospital center.
Materials and methodsA case series was carried out on patients that underwent lesion closure with the Ovesco clip, within the time frame of January 2015 to December 2017.
ResultsThe Ovesco clip was used for closure in 14 patients ranging in age from 21-90 years, with different indications: iatrogenic perforations; anastomotic leaks and fistulas; tracheoesophageal fistulas; and esophagogastric perforation. Technical success was achieved in 100% of the patients and clinical success in 78.57%. No complications were reported.
ConclusionsThe Ovesco Over-The-Scope Clip system is a safe and effective method for managing gastrointestinal acute perforations and fistulas.
Las perforaciones y fistulas enterales son de difícil manejo debido a las comorbilidades, mal estado nutricional y dificultades anatómicas relacionadas con múltiples intervenciones en estos pacientes. La utilización de métodos endoscópicos como abordaje no quirúrgico está incrementado. El objetivo del trabajo es describir la experiencia clínica con el uso del clip Ovesco en el cierre de perforaciones, fistulas y otras indicaciones en el tracto digestivo en un centro terciario.
Material y métodosSerie de casos en pacientes realizados entre enero de 2015 a diciembre de 2017.
ResultadosSe realizaron 14 casos con diferentes indicaciones: perforaciones iatrógenas; fugas y fistulas anastomóticas; fistulas traqueoesofágicas; cierres de perforaciones esofagogástricas, con rangos de edad (21-90 años). El éxito técnico se logró en el 100%, el éxito clínico fue en el 78.57% de casos. No se reportó ninguna complicación.
ConclusionesEs un método efectivo y seguro para el manejo de perforaciones agudas y fistulas enterales.
The Ovesco Over-The-Scope Clip (OTSC®) system is mounted on an application cap at the distal end of the endoscope in a manner similar to that of a variceal band-ligation cap. The system has been approved for use in humans in Europe since 2009 and in the United States since 2010.1,2 Its closure strength is equal to that of manual suture in ex vivo porcine models3 and it can grasp all the visceral wall layers, conditioning full-thickness cicatrization without causing adhesions.4,5
The most recognized indications for its use are in iatrogenic acute perforation closure, severe gastrointestinal bleeding, gastrointestinal fistulas, anastomotic defects, fistula correction in bariatric surgery, and closure of natural orifice transluminal endoscopic surgery (NOTES).
The aim of our study was to describe the clinical experience and outcomes using the Ovesco Over-The-Scope Clip system in the closure of gastrointestinal perforations and fistulas at a tertiary care hospital center.
Materials and methodsA case series was carried out on patients above 20 years of age that had Ovesco clip placement within the time frame of January 2015 to December 2017.
Technical success was considered when there was adequate clip placement and release, and clinical success was regarded as the resolution of the gastrointestinal problem and/or endoscopic or radiologic data that demonstrated complete closure of the defect. Case failure was defined as the poor positioning of the Ovesco clip and/or lack of resolution of the gastrointestinal problem.
Complications were considered those related to the endoscopic procedure or damage to the equipment.
Descriptive statistics were used to analyze the results and they were described through range and mean.
The study protocol was approved by the research and ethics committee of the Hospital Pablo Tobón Uribe in Medellín, Colombia. All patients signed statements of informed consent prior to the procedure.
Description of the procedureThe types of Ovesco clips and graspers employed, depending on the anatomic site affected, were those for: esophageal closure 11/3a (165cm), gastric closure 12/6gc (165cm), and colonic closure 12/6a (220cm). Endoscopic evaluation of the targeted site was performed, it was then aspirated, the tissue was suctioned and trapped with a Twin Grasper®, and the clip was deployed.
ResultsSixteen Ovesco clips were used in 14 patients with a mean age of 48.3 years (range: 21-90 years). The cases corresponded to 8 women (57.14%) and 6 men.
The Twin Grasper® was used in half of the patients, according to the criterion of the endoscopist, based on the anatomic characteristics and location of the lesion. Clip release was carried out utilizing the suction and trap technique in the rest of the cases. Technical success was achieved in 100% of the cases and clinical success in 78.57%. Case follow-up time was a mean 5 months (range: 1-12 months).
Lesion diameters varied from 5 to 30mm, with a mean of 17.1mm.
In relation to the laboratory tests carried out, albumin was documented in half of the cases and their levels were under the reference value (RV: 3.4-5.2mg/dl) (range: 1.8-3.2mg/dl, with a mean of 2.5mg/dl). Hemoglobin was registered in all the cases (range: 8.1-15.9mg/dl, with a mean of 10.5mg/dl). Those findings demonstrated the poor nutritional status in the average patient in our case series.
No complications were registered in relation to Ovesco clip placement.
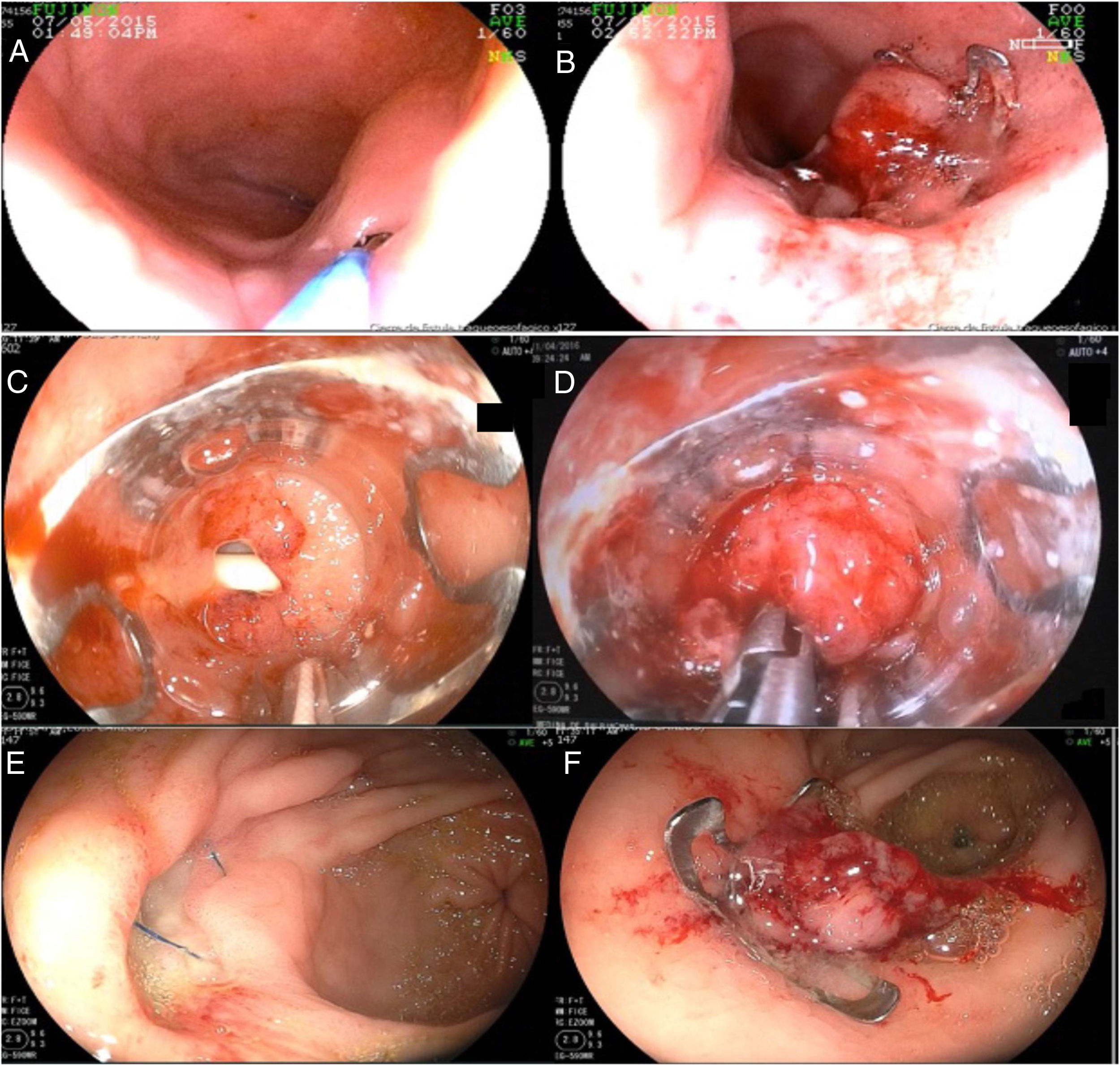
Results by indication groupFistula closureOvesco clips were used for fistula closure in 10 patients: 2 cases of fistula in the gastroenteric anastomosis; 2 cases of gastroperitoneal fistula associated with bariatric surgery (gastric sunset, gastric sleeve) of 7mm and 14mm, respectively; and 2 cases of tracheoesophageal fistula, the first in a patient with HIV/AIDS with a chronic 20mm fistula due to tuberculosis, and the second due to a 5mm fistula associated with tracheal polyp resection (figs. 1A and 1B), achieving complete closure in both cases.
 A guidewire is passed through a small tracheoesophageal fistula for its adequate identification. B) Ovesco clip released at the fistula site, with complete closure. C) Hiatal hernia perforation during the passage of the nasogastric tube. D) Use of the Twin Grasper®: moment of grasping the tissue to then release the clip. E) Suture dehiscence of the Graham patch in the stomach (anterior wall of the proximal antrum). F) Closure of the fistulous orifice with the Ovesco clip.")
A) A guidewire is passed through a small tracheoesophageal fistula for its adequate identification. B) Ovesco clip released at the fistula site, with complete closure. C) Hiatal hernia perforation during the passage of the nasogastric tube. D) Use of the Twin Grasper®: moment of grasping the tissue to then release the clip. E) Suture dehiscence of the Graham patch in the stomach (anterior wall of the proximal antrum). F) Closure of the fistulous orifice with the Ovesco clip.
The remaining 4 cases were colonic fistulas: the first was a 30mm colonic perforation due to cosmetic surgery (liposuction); the second was an 8mm fistula associated with abdominal blunt trauma; the third was a case of multiple colocutaneous fistulas, 18mm and 20mm, due to a gunshot wound (thoracoabdominal trauma), requiring 2 Ovesco clips; and the fourth was a case of diverticular perforation that fistulized (measuring 12mm). Closure was achieved in 75% of the cases.
Acute perforationOvesco clips were used in 2 cases of acute perforation: the first was an iatrogenic perforation of a nasogastric tube through a hiatal hernia (5mm) (figs. 1C and D) and the second was a perforated gastric ulcer, initially managed with a Graham patch that presented with dehiscence one week later (15mm). Clinical success in that indication was 100% (figs. 1E and F).
Miscellaneous indications: esophageal stent fixationOne case of acute traumatic 6cm perforation of the esophagus, in which a 10cm-long covered metallic stent was deployed and successfully fixed with an Ovesco clip to minimize the risk for stent migration.
Upper gastrointestinal bleedingOne case of a patient with gastrostomy that presented with bleeding from an internal granuloma through a fistulous canal. The bleeding episode was severe, with hemodynamic instability. The patient had undergone several endoscopic interventions with adrenaline injection, EndoClip®, and argon plasma that were unsuccessful in controlling the bleeding. An Ovesco clip was placed as a hemostatic and occlusive method.
DiscussionWe achieved 100% clinical success in the cases of acute perforation, results similar to those of Parodi et al., who described high effectiveness (90%) in gastrointestinal perforations smaller than 20mm,6 and to the success rate of a multicenter study7 that included 20 patients with acute iatrogenic perforations.
Our results in the cases of chronic fistula were encouraging, with clinical success in up to 70%. Success was 100% in the 2 cases of tracheoesophageal fistula. One of the chronic tracheoesophageal fistulas treated measured 20mm, which was interesting, given that in the case series of Monkemüller et al.,8 clinical success was achieved in only half of the cases when the indication was for tracheoesophageal fistula closure. Those authors noted that success with the OTSC® system could decrease in cases with openings larger than 10mm and those with fibrotic tissue.
In relation to the OTSC® system as a fixation method, good results in anastomotic leaks were described in a case series.9
The experience with Ovesco clips in cases of gastrointestinal bleeding refractory to other conventional endoscopic measures has been excellent. In a recent prospective study, clinical success was 100%, with no signs of rebleeding, in 6 patients with upper gastrointestinal bleeding that had dual endoscopic therapy failure.10
The Ovesco clip can be released after tissue is trapped and suctioned or with the help of a Twin Grasper®. In our study, the Twin Grasper® was used in half of the cases, especially in fibrotic tissues, or when not enough tissue could be brought together for clip release. We agree that the Twin Grasper® is not always required, as demonstrated in the study by Mönkemüller et al.,8 in which it was used in 25% of the cases. The grasper has an estimated price of almost 700 USD, and therefore increases the cost of the procedure.
The Ovesco OTSC® system is a promising device with which we obtained high rates of technical and clinical success for different indications. The system has been described in other studies as safe and free from complications.6–8 The OTSC® system is now clearly a part of the therapeutic arsenal of the advanced endoscopist but may require broader dissemination and use in clinical practice.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Mosquera-Klinger G, Torres-Rincón R, Jaime-Carvajal J. Cierre endoscópico de perforaciones y fístulas del tracto digestivo mediante el sistema «Over-the scope clip» (Ovesco), en un centro terciario. Revista de Gastroenterología de México. 2019;84:263–266.

