
Gallstone ileus is a rare complication of cholelithiasis. It is characterized by bowel obstruction secondary to gallstone impaction at some point of the gastrointestinal tract due to the existence of a bilioenteric fistula. The aim of this analysis was to evaluate our experience through a retrospective study, covering a 12-year period. It included 14 cases (10 women and 4 men) with a median age of 81 years; 11 of the patients had comorbidities. The main analytic alteration was an increase in urea (median 79mg/dl). Diagnosis was confirmed through abdominal computed tomography in 10 cases and plain abdominal x-ray in 4. The stone was located in the jejunum in 6 cases, the ileum in 6, and the sigmoid colon in one; the mean stone size was 3cm. There were 11 cases of cholecystoduodenal fistula, one case of cholecystocolonic fistula, and one idiopathic fistula. Two patients died, including the patient that did not undergo surgery.
El íleo biliar, rara complicación de la colelitiasis, se caracteriza por la oclusión intestinal secundaria a la impactación de un lito biliar en algún punto del tracto digestivo debido a la existencia de una fístula bilioentérica. El objetivo del trabajo es analizar nuestra experiencia mediante un estudio retrospectivo durante un período de 12 años. Se incluyeron 14 casos (10 mujeres y 4 varones) con una mediana de edad de 81 años y comorbilidades en 11. La principal alteración analítica fue elevación de urea (mediana 79mg/dl). El diagnóstico se confirmó mediante tomografía en 10 casos y radiografía simple de abdomen en 4. El cálculo se localizó en yeyuno en 6 casos, íleon en 6 y sigmoides en uno con un tamaño medio de 3cm. La fístula fue colecistoduodenal en 11 casos, colecistocólica en uno e idiopática en uno. Fallecieron 2 pacientes, incluido el caso no operado.
Gallstone ileus, a rare complication of cholelithiasis, is an infrequent cause of bowel obstruction (1-3%, although it can represent up to 25% of the small bowel obstructions in patients above the age of 65 years) caused by the impaction of a gallstone at some point of the gastrointestinal tract due to the existence of a bilioenteric fistula produced by multiple inflammatory processes. Its diagnosis is based on the Rigler triad (bowel obstruction, ectopic gallstone, and pneumobilia). Its treatment can be either enterotomy with or without differed cholecystectomy, or enterotomy, cholecystectomy, and fistula closure.1,2
The aim of this study was to analyze the clinical and demographic characteristics, treatment, and morbidity and mortality associated with gallstones due to a rare pathology.
MethodsA retrospective study of the case series of patients diagnosed with gallstone ileus at the Hospital Universitario San Juan de Alicante over a 12-year period (2001-2012) was conducted. The quantitative variables were defined through medians and percentiles (25; 75) and the qualitative variables by frequency and percentage.
ResultsDuring this time period, 1,165 cases of bowel obstruction were registered; 14 (1.2%) were due to gallstone ileus, of which 10 (71.4%) presented in women and 4 (28.6%) in men, with a median age of 81 years (77; 88). Eleven patients (78.5%) presented with some type of comorbidity; the most frequent were high blood pressure (8 cases; 57.1%), diabetes mellitus (5 cases; 35.7%), and heart disease (5; 35.7%), with a Charlson comorbidity index of 1 (0; 1) and an age-adjusted index of 5 (3; 6). Its incidence was 0.45 cases/100,000 inhabitants/year, distributed in the following 3-year periods: 2001-2004 (4 cases), 2005-2008 (4 cases), and 2009-2012 (6 cases).
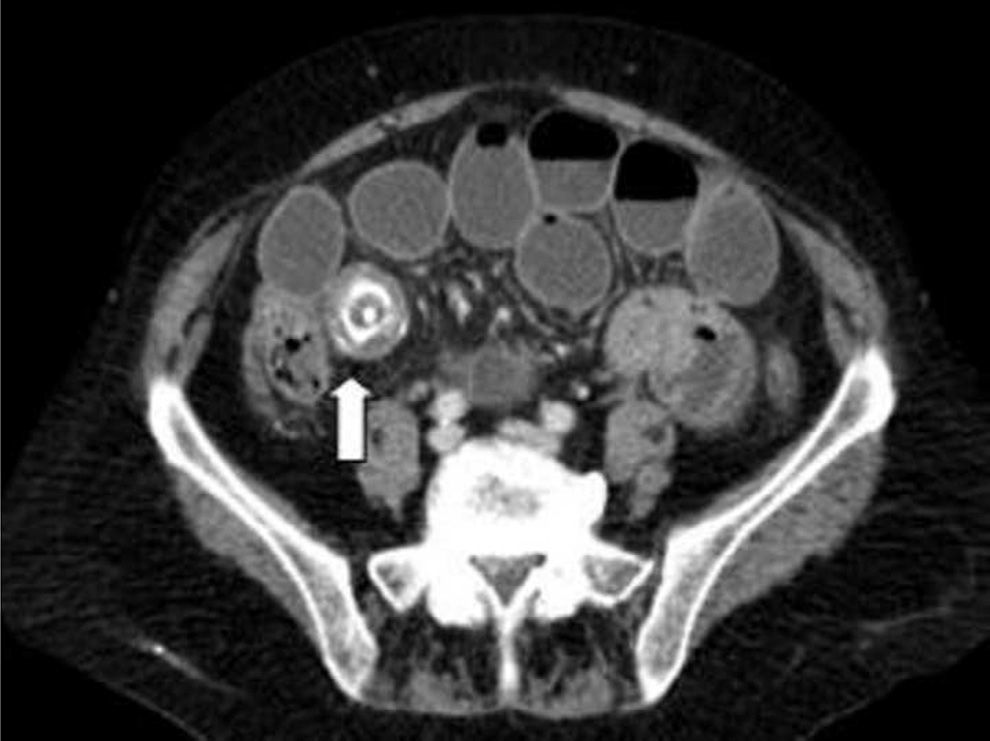
Upon admission to the Emergency Department, the symptoms the patients complained of were vomiting (14; 100%), colicky abdominal pain (12; 85.7%), and absence of bowel transit (5; 35.7%) of 2-day progression (1; 4). After the initial evaluation, blood tests were ordered and their results were: hemoglobin 14.8g/dl (13.2; 16.1), hematocrit 44% (38.7; 48.1), leukocytes 12100/mm3 (8,800; 18,600), neutrophils 86.5% (80; 89), urea 79mg/dl (58; 96), and creatinine 1.3mg/dl (1; 2). Diagnosis was confirmed by abdominal x-ray alone in 4 cases (28.6%) and abdominopelvic computed tomography scan was required in 10 cases (71.4%). Figure 1 shows the example of a case in which diagnosis was established through computed abdominopelvic tomography.
.")
The medical treatment that all the patients received consisted of absolute diet, glucosaline solution, and a nasogastric tube. Surgery was indicated in 13 cases, one of which was rejected by the surgical and anesthetic team due to the patient's prior health status (advanced age and dependency in daily life activities) and poor clinical situation at the time of emergency attention. The gallstones were located in the jejunum (6 cases; 46.2%), ileum (6 cases; 46.2%), and sigmoid colon (1 case; 7.7%) with a size of 3cm (3; 4) and enterotomy/colotomy was performed for their extraction, together with primary suture. The fistula was cholecystoduodenal in 11 cases (84.6%), cholecystocolonic to the hepatic angle in one case, and unknown in one case. There were postoperative complications in 9 cases (69.2%); 6 of them were medical (46.2%), primarily 4 cases of cardiac insufficiency and 2 of acute pulmonary edema; 6 were surgical (46.2%), 5 surgical wound infections and one evisceration that did not require re-intervention. Three patients presented with both types of complications. Twelve patients survived and 2 patients, including the one that was not operated on, died (14.3%). The mean hospital stay was 11 days (8; 15) and the mean outpatient follow-up period was 6 months (3; 8), during which time no gallstone ileus recurrence or re-admittance for cholangitis was observed.
DiscussionGallstone ileus is a pathology with a low incidence rate, but many authors suggest a greater importance due to the progressive increase in the age of the population; in the last four years, we have observed a discrete increase in this tendency, albeit in very small figures.2 This entity appears more frequently in advanced-age women with associated comorbidity, as occurred in our case series.1–4
The criterion standard for its diagnosis is abdominal x-ray in which the Rigler triad is observed; this occurs in less than 50% of the cases (in our series it was observed in 28.6%), making it necessary to carry out other radiographic studies such as ultrasound and computed abdominal tomography.2–6 Correct preoperative diagnosis is usually under 75%; in our case series, all the patients were preoperatively diagnosed due to the systematic use of computed abdominal tomography in cases of obstruction with no apparent cause, or of poor progression with conservative management that included a nasogastric tube.
Bilioenteric fistula can occur at any point, but the most frequent is the cholecystoduodenal location, as in our case series. The impaction site of the gallstone depends on its size and the diameter of the digestive tract lumen. The most frequent sites are the terminal ileum and the ileocecal valve; less common places are the jejunum, duodenum (Bouveret's syndrome), stomach, or colon. In our case series, the sites were the terminal ileum, jejunum, and colon; there were no cases in the duodenum or stomach.1–3
Treatment is surgical, through enterotomy either alone with or without differed cholecystectomy (2-stage surgery), or associated with cholecystectomy and fistula closure (1-stage surgery). Because the majority of patients are high-risk, most authors recommend the first option for resolving bowel obstruction symptoms, due to its lower morbidity and mortality (12 as opposed to 17% in 1-stage surgery), despite the theoretical risk for symptom recurrence (5%) or ascending cholangitis caused by bilioenteric fistula (10%) 2,7–9 In our case series, all the patients (except one in whom intervention was rejected) underwent enterotomy alone without fistula closure or differed cholecystectomy; mortality was similar to the published data and morbidity was high. Some authors have reported spontaneous evacuation of stones in 5-7% of the patients; we had no experience in that because all our study patients were operated on except one, who died a few hours after being admitted to the hospital.9,10
The main limitation of our study was its retrospective design, together with its small sample size, common in the majority of studies on gallstone ileus due to its low incidence.
In conclusion, gallstone ileus primarily affected advanced-age women that had associated comorbidity; its main cause was cholecystoduodenal fistula and the obstruction site was the terminal ileum and the jejunum. Treatment was surgical (enterotomy with stone extraction) and there was a high morbidity rate, most likely due to the type of population affected. We suggest the systematic performance of a computed abdominal tomography scan in the cases of bowel obstruction with no apparent cause or in those whose progression with conservative treatment with nasogastric tube is poor, so that the correct preoperative diagnosis of this pathology can be made.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: García-Marín A, Pérez-López M, Pérez-Bru S, Compañ-Rosique A. Gallstone ileus, an uncommon cause of bowel obstruction. Revista de Gastroenterología de México. 2014;79:211–213.

