

An 81-year-old woman had a past history of well-controlled high blood pressure and essential tremor treated with propranolol. She consulted her family physician after noticing the appearance of 8-10 painful lesions on her scalp over the last 3 weeks. The lesions (fig. 1) consisted of firm nodules, adhered to deep layers, between 1 and 2cm in size, and the majority had an ulcerated surface covered with small blood clots. She was referred to the dermatology service for consultation. Two weeks later, before said consultation, she presented with marked mucocutaneous jaundice, choluria, and acholia, for which she came to the emergency department of our center and was admitted to complete her evaluation. A cutaneous biopsy was ordered from the dermatology service. Blood test results were bilirubin 10.2mg/dl, AST 111 IU/ml, ALT 227 IU/ml, GGT 3300 IU/ml, and CA-19-9 436 IU/ml (normal limit < 37 IU/ml). An abdominal CT scan showed a mass located in the uncinate process of the pancreas that conditioned dilation of the common bile duct and duct of Wirsung. Peritoneal, pulmonary, and paravertebral muscle lesions suggestive of metastasis were also observed. Due to these findings, endoscopic ultrasound fine needle aspiration of the pancreatic mass was performed. The scalp biopsy (fig. 2) revealed the presence of cutaneous metastases with morphologic and immunohistochemical characteristics consistent with a pancreatic origin (positive for cytokeratins 7 and 19 and negative for cytokeratin 20). The sample of the pancreatic mass confirmed the presence of an adenocarcinoma at that level. The patient was informed of her diagnosis and prognosis and refused any active treatment for her disease. Thus, the biliary obstruction was treated with the endoscopic placement of a biliary stent and she was released with at-home palliative care.

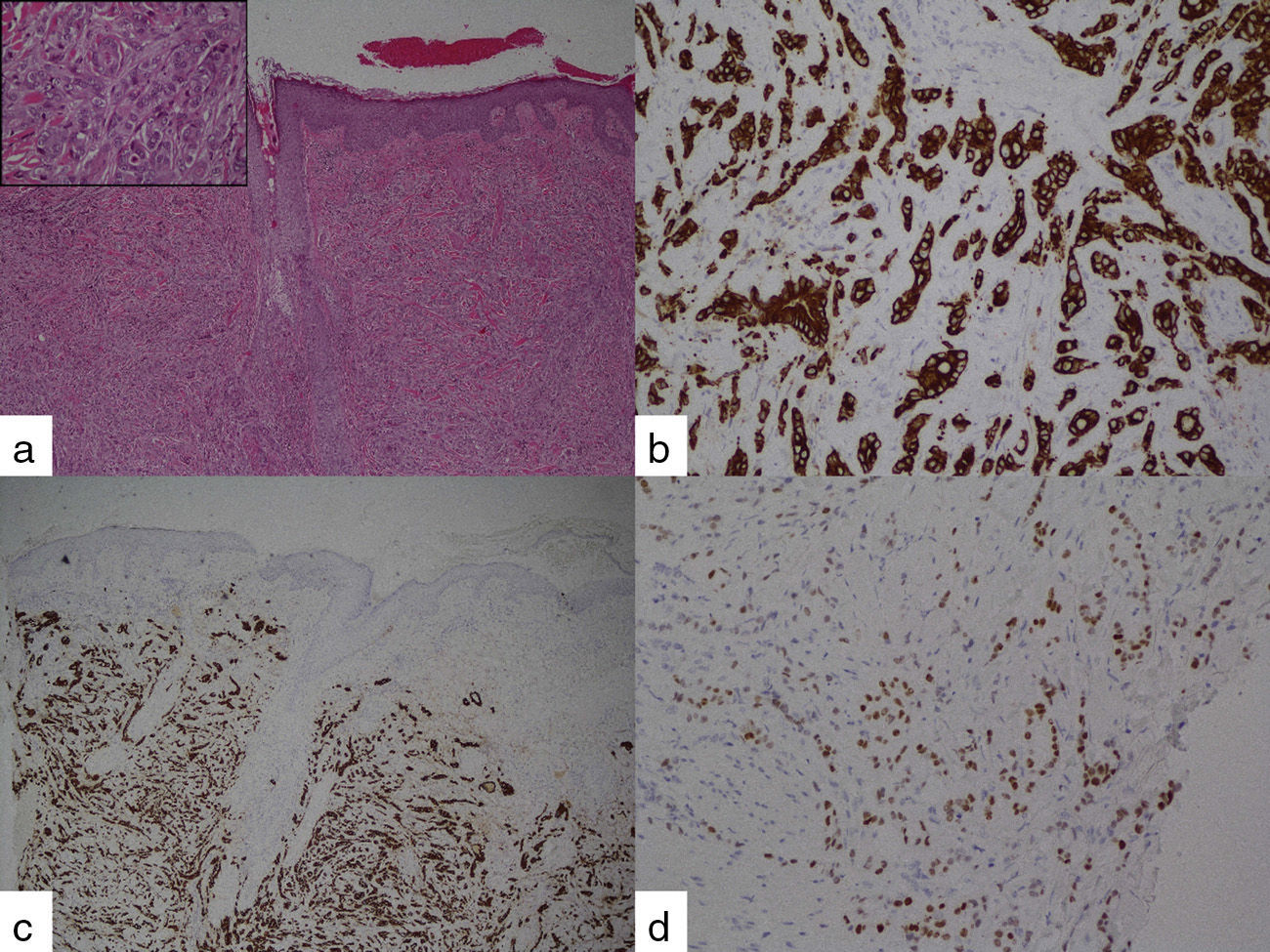
 hematoxylin-eosin stain x4, detail: hematoxylin-eosin, x40; b) immunohistochemical stain for CK7; c) immunohistochemical stain for CK19, and d) immunohistochemical stain for CDX2.")
Cutaneous metastases occur in 0.6%–10.4% of all patients with cancer,1 and is the first disease manifestation in 7.8% of the cases.2 When a lesion suspected of being cutaneous metastasis is found, in addition to the pertinent imaging studies, a biopsy of the lesion with immunohistochemical stain can provide orientation as to primary tumor diagnosis. CK 7 and CK 19 are present in the majority of pancreatic adenocarcinomas and CK 20 is negative in 38-80%. Stains positive for CA-19-9 and CEA are also frequent.3–6 In our case, immunohistochemical stain was suggestive of a pancreatic origin.
Adenocarcinoma of the pancreas is the fourth cause of cancer-related death and prognosis at its first appearance is normally poor, given that many cases are in advanced stages.7 The survival rate of pancreatic adenocarcinoma is especially devastating, with a median survival of approximately 5-6 months. The appearance of cutaneous metastases in this context has a similar impact on survival with respect to other more frequent locations,6,8 and it is customary to find other concurrent secondary implants. Therefore, treatment does not vary with this presentation.
Cutaneous metastases are rare and when they occur, they are usually located in the periumbilical zone, producing the lesion known as the “Sister Mary Joseph Nodule”.9,10 Outside of this location, metastases are uncommon, and are more frequent in men and in advanced-age patients.6
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Tavío-Hernández E, Cañete-Ruiz Á, Moreno C, Urech M, Cano-Ruiz A. Metástasis múltiples en cuero cabelludo como primera manifestación de adenocarcinoma de páncreas. Revista de Gastroenterología de México. 2015;80:287–289.

