

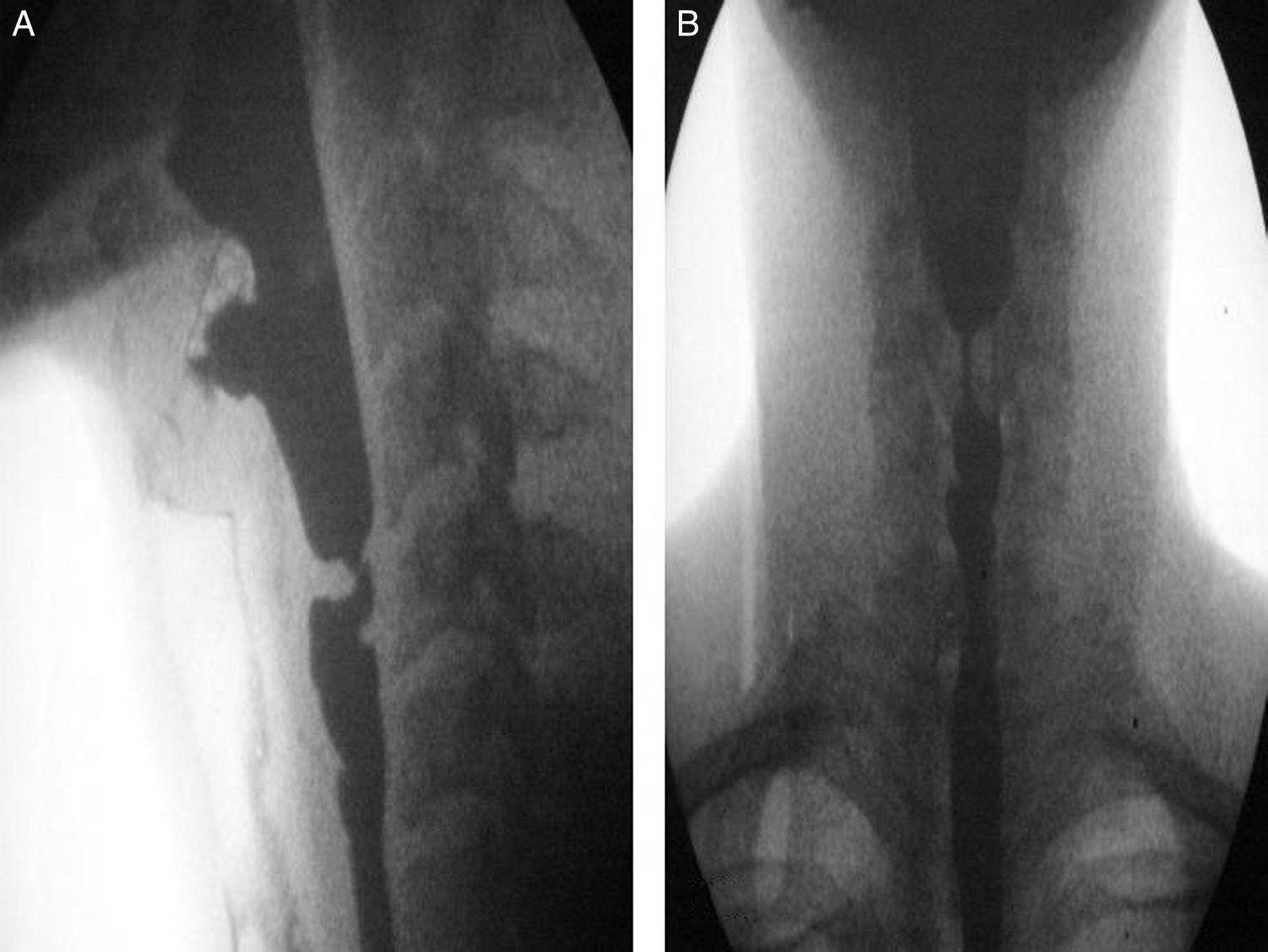
A 30-year-old man with a past history of epidermolysis bullosa since childhood, with several affected first-grade relatives, presented with generalized dermatologic involvement (figs. 1A and B) that intensified over the last 5 years. He was referred to the gastroenterology service with oropharyngeal dysphagia of 2-year progression and a 10-kg weight loss related to reduced food intake due to the swallowing alteration. He had dysphagia with solid food intake from the onset of the condition. As part of the clinical evaluation, the Volume-Viscosity Swallow Test (V-VST) was carried out: he tolerated liquids in small amounts at the time of the assessment. The evaluation protocol included endoscopy, which identified a stricture 13cm from the upper dental arcade that did not allow the passage of the endoscope. A barium swallow revealed a proximal stricture of the upper esophageal sphincter (figs. 2A and B). The treatment proposal was a modification in relation to food texture and caloric intake and non-endoscopic percutaneous gastrostomy for later dilation.
 Loss of fingernails, bleeding scabs and erosions on the back of the hands. B) Bleeding ulcers, erosions, and scabs on the wrists and forearms.")
 Lateral projection of the barium swallow: stricture in the proximal region of the upper esophageal sphincter. B) AP projection of the barium swallow: medial stricture in the proximal region of the upper esophageal sphincter. The proximal part of the stricture is dilated and the inferior part of the stricture has irregular walls.")
A) Lateral projection of the barium swallow: stricture in the proximal region of the upper esophageal sphincter. B) AP projection of the barium swallow: medial stricture in the proximal region of the upper esophageal sphincter. The proximal part of the stricture is dilated and the inferior part of the stricture has irregular walls.
Epidermolysis bullosa is a group of genetic alterations that belongs to the genodermatoses. Its pattern of inheritance is autosomal dominant or autosomal recessive. It is characterized by the formation of ampules on the skin and can sometimes affect the mucosa.1–3 The most important gastrointestinal involvement is esophageal stricture, presenting as a result of ampule formation and their later cicatrization, as well as from trauma caused by the passage of food, and its most frequent location is the upper third of the esophagus.4,5 The V-VST is utilized to evaluate patients with oropharyngeal dysphagia through different food textures and amounts. It evaluates the risks related to nutritional complications, along with the patients that require modifications in food consistency.6 Treatment of esophageal stricture consists of modifying a diet of solid foods to one of purees and liquids. Severe strictures require serial dilation that used to be carried out with Maloney or Tucker dilators through the gastrostomy tube.7,8 Today fluoroscope-guided dilation is preferred and has the advantage of specific anatomic identification, as well as evaluating stricture length and severity.9 Another option is gastrostomy, whether as laparoscopic-assisted gastrostomy, percutaneous endoscopic gastrostomy, or non-endoscopic percutaneous gastrostomy.10 Oral viscous budesonide has shown good results in children with non-severe esophageal stricture.11
Ethical responsibilitiesProtection of persons and animalsThe authors declare that no experiments were performed on humans or animals for this study.
Data confidentialityThe authors declare that they have followed the protocols of their work center in relation to the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Sarabia Aldana C, Zavala-Solares MR. Disfagia orofaríngea en paciente con epidermólisis bullosa. Revista de Gastroenterología de México. 2016;81:227–229.

