





The COVID 19 pandemic has forced the establishment of measures to avoid contagion during diagnostic and therapeutic tests in gastroenterology. Gastrointestinal motility studies involve a high and intermediate risk of transmission of infection by this virus. Given its elective or non-urgent indication in most cases, we recommend deferring the performance of these tests until there is a significant control of the infection rate in each country, during the pandemic. When health authorities allow a return to normalcy and in the absence of effective treatment or a preventive vaccine for COVID 19 infection, we recommend a strict protocol to classify patients according to their infectious-contagious status through the appropriate use of tests to detect the virus and its immune response, as well as the use of protective measures to be followed by health personnel to avoid contagion during the performance of a gastrointestinal motility test.
La pandemia por COVID 19 ha obligado a establecer medidas para evitar los contagios durante la realización de pruebas diagnósticas y terapéuticas en gastroenterología. Los estudios motores del tubo digestivo implican un riesgo elevado e intermedio de trasmisión de la infección por este virus. Dada su indicación electiva o no urgente en la mayoría de los casos, recomendamos diferir la realización de estas pruebas hasta que haya un control significativo de la tasa de infección en cada país, durante la pandemia. Cuando las autoridades sanitarias permitan el regreso a la normalidad y en ausencia de un tratamiento efectivo o una vacuna preventiva de la infección por COVID 19, recomendamos un protocolo estricto para clasificar a los pacientes de acuerdo a su estatus infecto-contagioso mediante el uso apropiado de pruebas para la detección del virus y su respuesta inmune, así como el uso de medidas de protección que deberá seguir el personal de la salud para evitar el contagio durante la realización de una prueba de motilidad gastrointestinal.
From the very start of the outbreak, SARS-CoV-2, or COVID-19 infection, has been highly contagious. The virus spread rapidly across the globe, and by May 2020, infected more than 5 million persons in 188 countries.1 Due to its high infection and fatality rates, along with the lack of prior immunity, this new infection has been perceived as a great threat to the life and health of the worldwide human population.
The first case of COVID-19 in Latin America was reported in Brazil on February 26, 2020, and the first death on March 7 in Argentina.2 In Mexico, the first case was reported on February 25 and the first death on March 18, and in Colombia, the first case was reported on March 6 and the first death of a physician on April 11.3 Thus, at the time of this writing (May 2020), Latin America is considered to be the epicenter of the pandemic. Confronted with that situation, and following the recommendations of the World Health Organization (WHO), the governments of the Latin American countries have declared health emergencies and implemented actions (on different dates and in accordance with the epidemiologic trend of each country), such as restrictions in the public, private, and social sectors that include voluntary quarantining, shutting down schools, closing borders, suspending international air travel, carrying out physical distancing, and limiting nonessential activities.
As in other parts of the world, medical care has changed dramatically in relation to non-urgent diseases that involve the performance of diagnostic and therapeutic procedures, such as those carried out at neurophysiology and/or digestive motility units. Positions have already been established on how to work and/or resume activities at those units (e.g., those issued by the American Neurogastroenterology and Motility Society [ANMS]4 and the Grupo Español de Motilidad Digestiva [GEMD])5 but due to the fact that the epidemiologic behavior, protective equipment availability, serologic diagnostic test performance capacity for corroborating immunity, and socioeconomic context are different throughout Latin America, a group of experts that are members of the Sociedad Latinoamericana de Neurogastroenterología (SLNG) had a virtual meeting to formulate a consensus document with recommendations for the performance of gastrointestinal motility tests.
The present document establishes a series of guidelines for prioritizing, selecting, and performing the most frequently indicated neurogastroenterology procedures at digestive units in the face of COVID-19, such as manometry and esophageal reflux measurement, anorectal manometry and biofeedback, and breath tests.
MethodologySummoned by the presidency and scientific committee of the SLNG, a group of experts in the area of neurogastroenterology from several Latin American countries had a virtual meeting on April 15, 2020, to formalize the creation of a document that would serve as a guide on how to resume and perform gastrointestinal motility procedures in the scenario of the COVID-19 pandemic. At that first reunion, three working groups were organized to revise and establish the recommendations for the areas of: 1) esophageal function tests, 2) anorectal function tests, and 3) breath tests. The recommendations established were based on currently available recommendations, consensuses, and evidence, making the necessary adjustments according to the settings of each Latin American country during the different phases of the pandemic. Two other virtual meetings were carried out to analyze, revise, and modify the recommendations of each working group. The final virtual meeting took place on May 27, 2020, at which the seven members of the expert group unanimously approved the recommendations that follow below.
Motility procedures and the risk for SARS-CoV-2 infectionHigh risk: Due to the nature of the virus and its transmission route, it is clear that all aerosol-generating procedures involve a very high risk of infection for the personnel exposed to them. Therefore, esophageal manometry, impedance pH monitoring, wireless capsule pH monitoring, antroduodenal manometry, and breath tests are the gastrointestinal motility tests that should be considered high risk.
Intermediate risk: The fact that the nucleocapsid protein of the virus has been detected in gastrointestinal epithelial cells and RNA of the virus has been found in stool points to the possibility of fecal transmission of SARS-CoV-2.6,7 In a meta-analysis on the subject, Tian et al.6 showed that fecal PCR became positive two to five days later than positive sputum PCR in 36-53% of the infected patients, and the fecal excretion of viral particles persisted up to 11 days after sputum excretion in 23-82% of the patients. In another meta-analysis, Cheung et al.7 estimated that the prevalence of viral RNA in stool in patients with COVID-19 was 48.1% (95% CI 38.3–57.9), reporting the case of a 78-year-old patient in whom viral RNA persisted up to 33 days. Importantly, the fact that viral particles are detected in stool does not necessarily mean there is transmission by that route, but in the face of uncertainty and following the colonoscopy guidelines, anorectal manometry (ARM), biofeedback, balloon expulsion test, electromyography, colonic manometry, and barostat study should be considered procedures of intermediate risk.8
Colonic transit measurements utilizing radiopaque markers, or a wireless motility capsule, are considered noninvasive procedures but involve exposure to subjects that could be asymptomatic virus carriers. Thus, we suggest that those tests also be considered intermediate risk.
When can we return to normality?Strictly speaking, it must be understood that NONE of the abovementioned procedures can be considered urgent to the extent that their performance would be required during the epidemic phase of the COVID-19 pandemic. According to numerous guidelines and recommendations, postponing all “elective” motility procedures should be managed in the context of the clinical indication and should be adapted to the reality of each Latin American country. The dialogue between physicians and patients is encouraged for explaining and understanding the situation.
The reopening of the motility laboratories in each Latin American country will depend on several factors, including:
- a)
The epidemiologic situation of the region. That situation is established according to the health authority of each country, considering the phases (Table 1) determined by the WHO9 for the COVID-19 pandemic:
- •
Phase 1 (case importation): in this first setting, the disease arrives at a country through one person or a small number of people that acquire the virus abroad, thus the number of cases is limited to a few dozen.
- •
Phase 2 (community contagion): for this stage of the pandemic, outbreaks of the disease begin to occur in persons that have not been traveling. The first persons with COVID-19 that arrived at the country infected others they came in contact with, and in turn, those persons continue to propagate the disease. Confirmed cases begin to surpass the hundreds and containment becomes more complicated.
- •
Phase 3 (epidemic contagion): This is the most critical stage in the advancing of an epidemic because it means the disease is now present in the entire country and there is an elevated number of community outbreaks (thousands of persons). The main risk is that the number of patients increases exponentially, overloading the healthcare facilities and medical services.
Table 1.Activity resumption according to the different phases of the pandemic.
Phase of the pandemic* PPE availability and supply When to resume motility studies Esophageal manometry/ pH impedance Anorectal manometry/ Biofeedback Breath tests Phase 3 (exponential increase of new cases) Limited(no reserve or less than a one-week supply) Postpone all procedures Postpone all procedures Postpone all procedures Phase 2 with a rapid increase of new cases Very low(less than a 4-week supply) Urgent procedures (waiting period < 2 weeks):- EM in cases of suspected achalasia whose diagnosis imminently influences treatment- EM in cases of severe dysphagia that prevents oral nutrition and hydration There are no urgent proceduresPostpone all procedures There are no urgent proceduresPostpone all procedures Phase 2 but with a trend toward a decrease of new cases (deacceleration, end of lockdown) or with no epidemiologic evidence of exponential increase Sub-optimum (a 4 to 8-week supply) Resume or maintain at 50% capacityPrioritize the following semi-urgent procedures (waiting period of 2−4 weeks):- EM to evaluate dysphagia (no achalasia)- Preoperative EM evaluation of cases of large hiatal hernia - pH-impedance if the diagnosis would radically change treatment, for example, pulmonary manifestations Resume or maintain at 50% capacityPrioritize the following semi-urgent procedures (waiting period of 2−4 weeks):- Patients that had begun biofeedback therapy and did not finish it during the pandemic- Severe fecal incontinence, considering that ARM could influence medical/surgical treatment - Patients with proctalgia- Patients with severe constipation in whom dyssynergy needs to be corroborated or ruled out Resume or maintain at 50% capacityThere are no semi-urgent procedures Phase 1 or 5 Decrease or absence of cases for at least two weeks Normal (12-week availability and supply) Return to total capacity (100%) and resume activities based on the pre-pandemic indications for each study Return to total capacity (100%) and resume activities based on the pre-pandemic indications for each study Return to total capacity (100%) and resume activities based on the pre-pandemic indications for each study ARM: anorectal manometry; EM: esophageal manometry; PPE: personal protective equipment.
- •
The WHO also recognizes other possible settings, once the situation begins to stabilize and the contagion curve begins to flatten.
- •
Phase 4 (second wave): Once local contagion is reduced, imported cases are likely to present again, producing a second wave of infected patients. That can occur three to nine months after phase 3 has ended.
- •
Phase 5 (end of the epidemic): The WHO is in charge of declaring the end of the pandemic once the majority of countries are safe, with contagion under control.
In countries with adequate epidemiologic surveillance systems, the declaration of phases is established, based on the number of new infections expected to occur as a result of infection by a single individual (R0), which expresses the speed at which the disease can propagate in a given population.10 If the R0 is close to a value of 2, the country is experiencing exponential growth. An R0 of 1 indicates that the infection rate is remaining constant, and when it is below 1 (e.g., two infected persons would infect fewer than two individuals), the number of infected persons is decreasing.
- b)
Availability of personal protective equipment. Obviously, the risk of infection in healthcare professionals is higher if they do not have the adequate personal protective equipment (PPE) (see further ahead). However, it is important to recognize that there is a worldwide shortage of material, resulting in possibly limited availability in some of the Latin American countries. In fact, the Inter-American Society of Digestive Endoscopy11 and the Asian-Pacific Society for Digestive Endoscopy (APSDE-COVID declarations)12 issued their recommendations based on PPE availability. We believe that could play a key role in the reopening of gastrointestinal physiologic procedures in our region (Table 1).
- c)
Type of institution at which motility studies will be performed: Outpatient centers that specialize in those techniques have a lower risk than hospitals or clinics because they have a lower circulation of patients. Such centers also aid in decongesting the demand at hospitals.
Table 1 summarizes activity resumption in relation to the phases of the pandemic, PPE availability, and the urgency of the primary digestive motility test procedures.
With which patients and tests can we return?Once the return to activities or the reopening of activities is being contemplated, it is important to consider each of the following aspects:
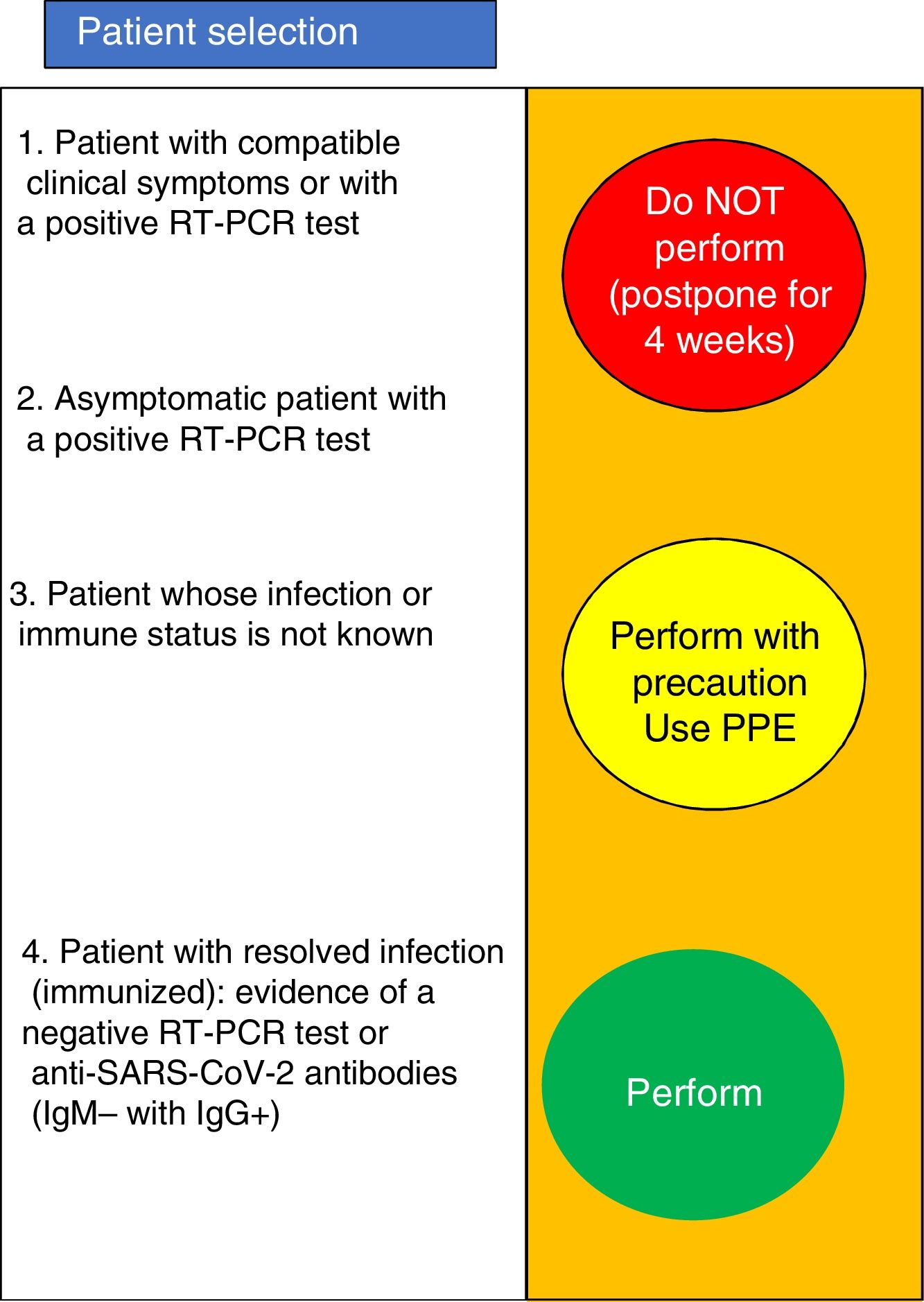
Patient selectionAccording to the GEMD,5 at present there is NO conclusive scientific evidence that supports performing microbiologic tests before a motility procedure to diagnose SARS-CoV-2 for the purpose of modifying the protective measures related to the infection. However, it is important to recognize that increasingly more subjects infected with SARS-CoV-2 are recovering, but there is also a high number of subjects that can be asymptomatic carriers. RT-PCR testing determines if the patient is infected, whereas serologic testing (IgM and IgG against SARS-CoV-2) determines the immune status. Depending on the availability of those tests in each country, their performance before the patient undergoes neurophysiologic studies is recommended. In line with that, patients indicated for a digestive motility study should be classified as follows:
- 1
Patient with clinical symptoms consistent with COVID-19 or a positive RT-PCR test.
- 2
Asymptomatic patients with a positive RT-PCR test.
- 3
Patient that had COVID-19 infection and developed an immune response: a negative RT-PCR test and negative IgM with positive IgG.
- 4
Patient whose infection status or immune status is not known.
In cases 1 and 2, the motility test will not be programmed and should be re-scheduled for at least four weeks later (Fig. 1). Corroboration of active infection resolution (a negative RT-PCR 24−48 h before the motility study) is recommended. In case 3, the motility test can be performed with no problem. Importantly, availability of and access to those serologic and molecular biologic tests can vary between the Latin American countries. Therefore, in treating case 4 patients, a potential risk of infection must be assumed, and the motility test must be performed utilizing all the PPE (that scenario is probably the most common in our countries).
It is very important to take into account that even though the RT-PCR test is the “gold standard”, there is variability in its diagnostic accuracy. For example, false negatives have been reported at 30%, if the test is performed during the first days of infection or the pre-symptomatic phase.13 Therefore, the recommendations must be adjusted to the sensitivity and specificity of each test and the laboratories that perform those assays must be encouraged to use the commercial tests that have shown the best diagnostic accuracy.
A) emergency-based test selectionEsophageal function testsThe esophageal physiologic studies, including esophageal manometry (conventional or high resolution), 24-hpHstudy, or pH-impedance study are diagnostic tests usually performed on ambulatory patients in the context of gastroesophageal reflux symptoms or nonobstructive dysphagia. They have a broad spectrum of clinical indications that includes the evaluation of antisecretory treatment-refractory esophageal symptoms (dysphagia, regurgitation, or chest pain) not explained by upper gastrointestinal endoscopy assessment, the evaluation of esophageal motor function prior to antireflux surgery, the evaluation of persistent reflux symptoms despite medical therapy, or the development of postoperative dysphagia.14,15
In general, they are elective tests that in exceptional cases can have an urgent indication (Table 1). Certain medical indications can have a degree of urgency, as recently described by the ANMS.4 The presence of probable achalasia with severe symptoms (significant dysphagia making oral food intake and hydration impossible), the presence of large hiatal hernias (with risk of aspiration or volvulus), or the impossibility of maintaining oral hydration and nutrition are relatively urgent, or semi-urgent, indications. In the case of giant hiatal hernias, if manometry cannot be carried out due to the COVID-19-related limitations, surgery should be performed without previous manometry.
All other indications, such as dysphagia with no weight loss, reflux studies prior to antireflux surgery, studies due to refractory reflux symptoms, and suspicion of supragastric belching or rumination syndrome, can be postponed.16
For as long as there is no return to performing functional tests, the recommendation is to support achalasia diagnosis or dysphagia evaluation through barium swallow tests, which can be useful. Regarding patients with reflux symptoms, continuing, changing, or adjusting the medication dose is recommended during the time in which it is not possible to complete their diagnostic evaluation.
Anorectal function studies and biofeedback therapyAccording to the International Anorectal Physiology Working Group (IAPWG) and the London classification, the conventional indications for performing anorectal function tests (primarily anorectal manometry [ARM])17 are: 1) constipation and/or defecation disorder symptom evaluation, 2) fecal incontinence (FI) evaluation, 3) painful anorectal disorder evaluation, 4) preoperative and postoperative evaluation of ileorectal anastomoses, rectopexy, fistulotomies, etc., and 5) evaluation of obstetric trauma. It should also be pointed out that ARM, in addition to having a diagnostic purpose, is utilized in many centers for biofeedback therapy in patients with constipation and/or fecal incontinence.
In that respect, and reviewing the indications, we emphasize the fact that anorectal function tests are not urgent procedures, and thus should be postponed during the exponential phase of the pandemic.
When laboratories are reopened, certain semi-urgent situations should be prioritized (Table 1). Returning first to the performance of ARM in patients that had already received biofeedback therapy or had been programmed for it before the pandemic, is sustained by IA and IIB grades of evidence in the management of constipation and FI, respectively, according to the ANMS.18 In addition, its resumption in patients with FI is supported by the fact that ARM provides a pathophysiologic approach in more than 90% of cases. For example, sphincter hypertonia (low resting baseline pressure) is associated with passive FI,19,20 whereas hypocontractility (the inability to reach an increase in pressure during voluntary contraction) suggests that FI, specifically urge FI, can be secondary to external anal sphincter (EAS) lesions. In a prospective study conducted by Rao et al., ARM not only confirmed the clinical impression but also contributed new clinically undetected information on patients with FI and influenced the treatment decision in the majority of cases.21
Until the return to normality, recommendations for patients that have not completed their biofeedback sessions include: continue, at home, carrying out the pelvic floor exercises learned during training or use the electronic devices.22 If patients had learned how to perform those types of exercises before the pandemic, they should continue doing them on a regular basis. With respect to constipation and chronic proctalgia, we recognize that they considerably compromise patient quality of life, but given their chronic nature, we feel that the performance of ARM can wait, as long as patients are offered symptomatic medical treatment (laxatives, antispasmodics, etc.) to mitigate symptom intensity. If defecatory dyssynergy is suspected in relation to inappropriate straining, abdominal breathing exercises can be useful.23 If defecation alterations related to posture are suspected, its correction, including the use of a device that favors the opening of the anal right angle (a 6-inch-high footstool to favor knee flexion) can also be helpful.24
The performance of other anorectal tests involving the placement or manipulation of probes or devices in the anorectum, e.g., surface electromyography, barostat, or pudendal nerve latency, should follow the same recommendations for ARM. None of those tests are considered urgent and they should be programmed once neurogastroenterology units have returned to normality. Regarding colonic transit with radiopaque markers or with a wireless capsule, even though they do not involve an aerosol-generating process, they should be postponed, given that patients and physicians are frequently going to the health units for study follow-up and surveillance. Finally, colonic manometry, which requires colonoscopy-assisted probe placement, is considered a procedure with intermediate risk that should be postponed until the final stage of the pandemic.
Breath testsBreath tests are studies that are widely used to evaluate different function alterations, such as bacterial overgrowth and intolerance to different carbohydrates (mainly lactose), and are the standard for corroborating eradication of Helicobacter pylori infection.25,26 They are programmed studies and are not to be considered a medical emergency under any circumstance during the COVID-19 pandemic.
Even though the filter mouthpieces of some systems incorporate a unidirectional valve and an infection control filter that have been shown to eliminate 99% and 96.5% of the bacteria and viruses in the air, respectively, specific tests have not been carried out to demonstrate whether they are capable of preventing SARS-CoV-2 infection.
How do we return?The general steps to follow are detailed below, taking into account that there can be certain variations according to the test that is performed.4,5
Patient preparation- a)
A telephone interview with the patient should be carried out 24 h before a motility test to identify symptoms consistent with COVID-19 (cough, fever, myalgia, anosmia, ageusia, diarrhea). If any of those symptoms are identified, the recommendation is to cancel the appointment and postpone it until the case is re-evaluated. The patient should be sent to a service (clinic, emergency room, infectious diseases unit, etc.) that can perform a RT-PCR test and provide appropriate management. That recommendation will depend on the protocol for COVID-19 care established in each country.
- b)
Patients should preferably go to their appointment alone, but if not possible, be accompanied by only one person, ideally under 65 years of age. The patient and companion should each be given a facemask if they entered the unit without one. The patient and companion should then apply hand sanitizer or wash their hands.
- c)
The companion should not enter the unit, unless the patient requires specific assistance, and should stay in the waiting room.
- d)
Before entering the room in which the procedure will be performed, all patients must be asked again about the presence of respiratory symptoms or fever, to stratify their transmission risk, and their body temperature should be measured. If there is any suspicion, the procedure should be canceled and rescheduled.
- a)
- a)
Personnel care
- •
Promote the application of basic hygiene measures, among the entire personnel, for the prevention of infection.
- •
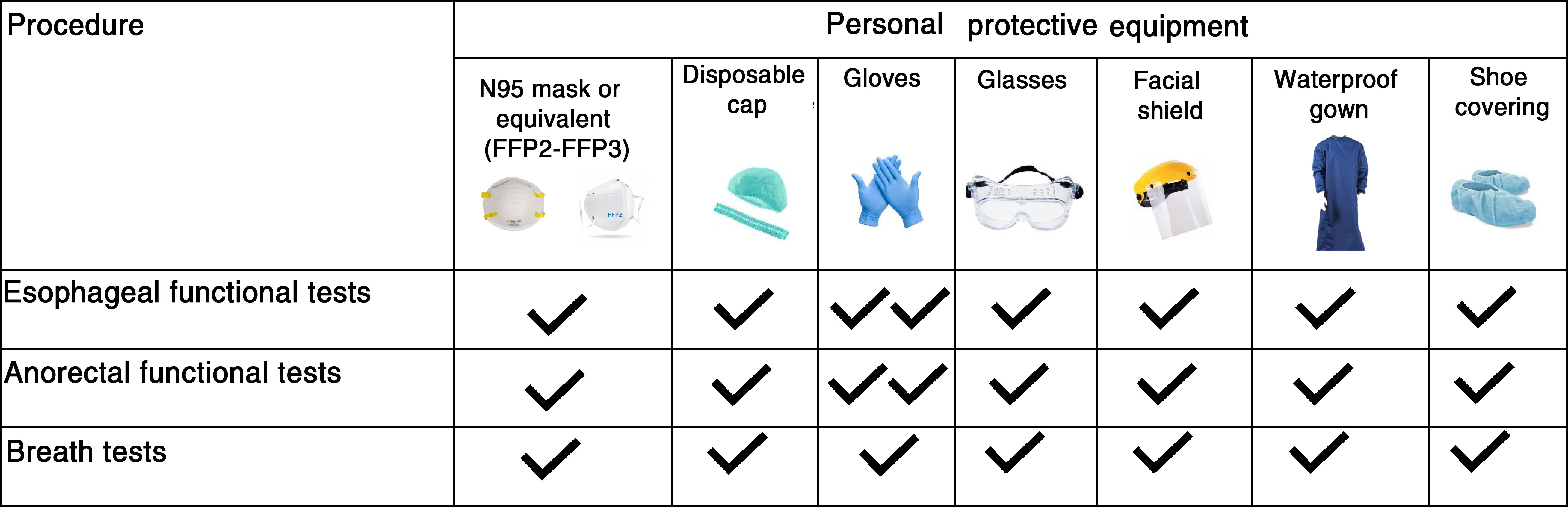
Given that the large majority of Latin American countries are in a community transmission phase, in which spread via asymptomatic individuals is reported, PPE use by all the healthcare personnel involved in the procedures is recommended.
- •
Fig. 2 shows the PPE recommended for each procedure.
- •
The procedure should not be performed if the PPE necessary for guaranteeing the performance safety of the manometric studies is not available.
- •
Learn how to adequately put on and take off all PPE.
- •
- b)
Equipment care and use recommendations
- •
Equipment preparation and probe calibration should be performed before the patient is admitted to the procedure room, to decrease the amount of exposure time.
- •
If informed consent is utilized, promote the use of “verbal or recorded” consent, when permitted by local committees. Otherwise, consider disinfecting the material involved (ballpoint pens or pencils) and insist on handwashing after contact with said material.
- •
The patient will be asked to enter the procedure room with no personal belongings (cellphone, glasses, keys, etc.).
- •
Regarding ARM, the patient will change clothes in a specific bathroom (whose cleaning should follow the specific protocol for COVID-19).
- •
All the material utilized (syringes, trays in case of vomiting) should be disposable.
- •
The test should be performed by an expert and not more than 2 persons are recommended to be in the room during the procedure.
- •
The manometric system, as well as the computer keyboard, can be covered in plastic film during each examination.
- •
- •
With respect to pHstudy and pH/impedance, consider whether it is possible to favor the use of disposable or single-use probes.
- •
When using high-resolution solid-state equipment without impedance, consider whether utilizing a disposable case could be useful.
- •
With respect to old modelpHstudy equipment that has a leather carrying case, an alternative could be a plastic bag to cover the case and prevent damage during post-examination disinfection.
- •
Utilizing the Chicago protocol and avoiding unnecessary maneuvers that prolong study duration are recommended.
- •
To the degree possible, if there is more than one procedure room, studies could be carried out in alternating rooms to provide sufficient time for sanitization, if more than 2 studies are to be carried out per day.
- •
- •
If fecal material is encountered during rectal examination, and prior to the introduction of the manometry probe, an enema is customarily given, waiting 30 min to perform the test. In the context of the COVID-19 pandemic, we do NOT recommend that measure because it can increase the risk for exposure. If an enema is to be used, it can be applied at home, before the performance of the motility study.
- •
The London protocol is recommended because the duration of the test, which should be performed by an expert, is 15 min.
- •
The use of high-resolution systems is promoted, given that perfusion systems have the disadvantage of the probes needing constant water perfusion, resulting in the continuous outflow of water into the anal canal, increasing the risk for contact with body fluids.
- •
Systems that have a disposable case for the probe are recommended because they are safer for the patient.
- •
If a balloon expulsion test is to be performed at the end of the study, a disposable probe is recommended.
- •
The post-procedure measures are subject to constant review, depending on the overall situation of each hospital, daily necessities, and material availability, and are adapted to them and to the recommendations of the acting authorities in each country.
- •
Carry out the disinfecting and reprocessing of the probes according to the customary protocol.
- •
Do not reuse single-use devices.
- •
Assign cleaning personnel that exclusively work at the physiology unit.
- •
Apply the protocols for the cleaning and disinfecting of materials that come into contact with patients or their secretions, such as the examining table, keyboard, and screens.
- •
Disinfecting and cleaning are to be performed with a disinfectant included in the institutional cleaning and disinfection policy. The COVID-19 virus is inactivated after five minutes of contact with disinfectants such as bleach, alcohol at 70%, and a sodium hypochlorite solution containing 1000 ppm of active chloride.
- •
Manage residuals following the local protocols of each center for category B (UN3291) high-capacity ineffective material.
- •
Maintain physical distancing of 1–2 meters, basic hygiene measures, and the independent flow of patients in the recovery rooms.
- •
Consider the implementation of patient follow-up programs 7–15 days after the procedure, to evaluate the appearance of symptoms consistent with SARS-CoV-2 infection.
- •
Promote the delivery of unprinted reports and recommendations, i.e., making them online.
The COVID-19 pandemic has forced the establishment of measures to prevent contagion during the performance of therapeutic and diagnostic tests in gastroenterology. Digestive tract motility tests involve intermediate and high risks for transmission of COVID-19 infection. Given their elective and nonurgent indication in the majority of cases, we recommend postponing those tests until there is significant control of the infection rate in each Latin American country during the pandemic. When the health authorities allow the return to normality, and in the absence of an effective treatment for COVID-19 infection, or a preventive vaccine, we recommend a strict protocol for classifying patients according to their infectious-contagious status through the appropriate use of tests for detecting the virus and the immune response to it, as well as the use of protection measures that the healthcare personnel should follow to prevent contagion during the performance of a gastrointestinal motility test. Finally, we recognize that the recommendations contained herein can change in the future, as more evidence with respect to safety measures is being produced.
Financial disclosureNo financial support was received in relation to the present article.
Conflict of interestJose María Remes Troche is a member of the advisory board of Takeda, Asofarma, and Biocodex. He has given talks for Takeda, Asofarma, Medtronic, Carnot, and Alfasigma.
Miguel Ángel Valdovinos Díaz is a member of the advisory board of Takeda. He has given talks for Takeda, Asofarma, Medtronic, Carnot, and Grünenthal.
Laura Sole has given talks for Roemmers, Casasco, Asofarma, Temis Lostaló, and Raffo
Albis Cecilia Hani Amador has given talks for Medtronic, Takeda, Abbott, Biopas, and Astra Zeneca.
Claudia Defilippi has given talks for Pharma Investi, Ferrer, and Axon Pharma.
Luis María Bustos Fernández declares that he has no conflict of interest.
Ricardo Veibig declares that he has no conflict of interest.
Please cite this article as: Remes-Troche JM, Valdovinos-Diaz MA, Viebig R, Defilippi C, Bustos-Fernández LM, Sole L, et al. Recomendaciones para la reapertura y reinicio de actividades de las Unidades de Neurogastroenterología ante la pandemia por COVID-19. Posicionamiento de la Sociedad Latinoamericana de Neurogastroenterología. Revista de Gastroenterología de México. 2020;85:428–436.

