
There has been a recent increase in the consumption of cow's milk substitutes, specifically plant-based beverages, which have erroneously been named “plant milks”. Plant-based beverages do not have a standard of identity, and so their nutritional composition can vary from one brand to another, even within the same category. The aim of the present narrative review was to produce a technical opinion to serve as a frame of reference for sustaining the recommendation of soy plant-based beverages. Nutrition and gastroenterology experts that belong to the Asociación Mexicana de Gastroenterología jointly commented on and analyzed themes on plant-based beverages, and on soy drinks in particular, including their nutritional characteristics, consumption in children, and potential growth and development alterations, as well as soy drink consumption in adults and its association with gastrointestinal alterations and other conditions. Plant-based beverages, including those made from soy, are not a replacement for breastmilk or breastmilk substitutes. Soy beverages are considered safe and can enrich the varied diet of its consumers, as long as they are considered an additional liquid portion of the diet. They can be ingested by adults and children above two years of age that present with cow's milk protein allergy or lactose intolerance.
Recientemente ha habido un aumento en el consumo de sustitutos de la leche de vaca, específicamente bebidas de origen vegetal, a las cuales de forma equivocada se les ha dado el nombre de «leches vegetales». Las bebidas vegetales no tienen un estándar de identidad, por lo que su composición nutricional puede variar de marca en marca, inclusive dentro de la misma categoría. El objetivo de esta revisión narrativa fue generar una opinión técnica que sirva como marco de referencia para sustentar la recomendación sobre el consumo de bebida vegetal de soya. Expertos en nutrición y en gastroenterología de la Asociación Mexicana de Gastroenterología comentaron y analizaron de forma conjunta temas acerca de las bebidas vegetales, específicamente de la bebida vegetal de soya, sus características nutrimentales, su consumo en el niño y potenciales alteraciones en el crecimiento y desarrollo, así como del consumo de la bebida de soya en el adulto, y asociaciones con alteraciones del aparato digestivo y otras condiciones. Las bebidas vegetales, incluida la bebida vegetal de soya no son un sustituto de la leche materna ni de los sucedáneos de la leche materna. Las bebidas vegetales de soya son consideradas seguras y pueden enriquecer la dieta variada de los consumidores, siempre y cuando se considere como una más de las porciones líquidas de la dieta. Pueden ser ingeridas por pacientes adultos y niños mayores de dos años con alergia a las proteínas de la leche de vaca o intolerancia a la lactosa.
Plant-based beverages and products have been consumed since the first civilizations all over the world, beginning as small-scale productions for the individual, immediate family, or small local community.1 Over the past 20 years, there has been a global increase in plant-based beverage consumption, with soy drinks being in greatest demand in North America, followed by Latin America, Europe, and Asia.2 Various factors explain the growing popularity of those beverages as alternatives to cow's milk, and they include a greater awareness of the relation of nutrition to the high prevalence of chronic diseases; the presence of entities, such as lactose intolerance or cow's milk protein allergy (CMPA); greater consumer interest in protein and the recognition of soybean foods as good sources of high-quality protein; and the diffusion of research results suggesting that soybean products can be beneficial for health.3 There is a current perception that plant-based beverages, such as those made from soy, are healthy, due to the emphasis placed on their vitamin, fiber, and low-cholesterol content. Consequently, a growing number of consumers have opted for such beverages, adding them to their diet as part of an intended lifestyle improvement.4 Plant-based beverages have been labeled as “milk”, which strictly speaking, is incorrect. According to the Codex General Standard on the Use of Dairy Terms, milk is “the normal mammary secretion of milking animals, obtained from one or more milkings, without either addition to it or extraction from it, intended for consumption as liquid milk or for further processing”, and recommends substituting the term “soy milk” with “soy-based beverage”.5 According to the US Food and Drug Administration (FDA), plant-based beverages as alternatives to milk are defined as those foods that have the physical characteristics of milk or milk-based products, such as taste, flavor, body, texture, and appearance, but do not meet the definition of milk and are nutritionally inferior to the product they wish to imitate.6 However, among its definitions of milk, the Real Academia Española includes “a whitish or milky beverage made of vegetables, plants, or seeds” but there are also a series of alternative terms that can be used, such as “plant-based drink”, or simply “drink”, or even “fortified drink”.7 Those milk substitutes are based on the aqueous extraction from different categories of plants: (a) legumes, such as soybeans, peanuts, peas, or mung bean; (b) nuts, such as almonds and hazel nuts; (c) oilseeds, such as sesame and hemp seeds; (d) oily plants, such as palm trees that bear coconuts; (e) cereals, such as corn, wheat, khorasan wheat, oats, rice, and spelt; (f) pseudo-cereals, such as amaranth, quinoa, and buckwheat; and (g) sedges, such as earth almond. Despite the fact that many plant-based beverages try to resemble milk in color and taste, their nutritional composition is different. The protein content of certain plant-based drinks can be high (legume-based drinks), medium (cereal-based), or low (some rice or nut-based drinks). It should be pointed out that plant-based beverages do not have a standard of identity, and thus their nutritional composition can vary from one brand to another, even within the same category. Therefore, the nutritional composition of the product should always be verified. In addition, it must be clearly understood that the nutritional value of a plant-based drink is not equivalent to that of its corresponding original food.8 Many gastrointestinal disorders are associated with diet and patients often restrict foods from or add them to their diet on their own initiative, following advice based on popular beliefs. Physicians are frequently asked about the possible benefit and safety of the dietary inclusion of plant-based beverages in different clinical contexts, and we often do not have the quality information necessary to give an opinion.
In December 2018, the Asociación Mexicana de Gastroenterología summoned a multidisciplinary group of 14 specialists to review and discuss the scientific evidence on plant-based beverage consumption, in relation to both general and gastrointestinal health, in children and adults, and formulate a technical opinion.
MethodsThree coordinators of the group were named (RV, MI, and MR) and they carried out a review of the bibliography, utilizing the search words of “soy”, “plant drinks”, “soy drinks”, “soy intake”, “soy consumption”, “soy drink consumption”, “lactose intolerance”, “soy allergy”, “digestive system”, “digestive diseases”, “diet”, “nutrition”, “treatment”, “therapy”, “prevention”, “management”, “review”, “guidelines”, “consensus”, and “meta-analysis” and their Spanish equivalents. The search was conducted in PubMed, encompassing articles written from January 1990 to November 2018. All publications in English and Spanish were included. Preference was given to consensuses, guidelines, systematic reviews, and meta-analyses, but was not limited to them. Complementary electronic and manual searches were also conducted on all publications up to December 2018 that the coordinators deemed relevant. The complete bibliography was at the disposal of the working group, to be consulted at any time throughout the entire process. Given the nature of the document, there are no ethical implications. The result of the finished review is presented below.
Soy plant-based beverageAccording to the Regional Standard for Non-Fermented Soybean Products of the CODEX ALIMENTARIUS (CXS 322R-2015), the classification of soy drinks and related products is the following: (a) plain soybean beverage: a milky liquid, prepared from soybeans, removing the protein and other components in hot/cold water or through other physical means, without adding optional ingredients; (b) composite or flavored soybean beverages: a milky liquid prepared by adding optional ingredients to plain soybean beverages, which include products such as sweetened, salted, or spiced soybean beverages; (c) soybean-based beverages: a milky liquid prepared by adding optional ingredients with a lower protein content than composite or flavored soybean beverages.9
It is important to differentiate between soy-based drinks and infant formulas based on soybeans. The European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) suggests that soy protein infant formula can be used in cases of severe or persistent lactose intolerance, galactosemia, or religious and other considerations that stipulate the prohibition of cow's milk.10 The present document does not offer detailed information on soy protein-based infant formulas, but it does mention them when describing the effects of soybeans on children. It specifically encompasses the evidence on soy plant-based beverages, emphasizing eliminating the use of the term “soymilk”.
Nutritional aspects of soybeansSoybeans (Glycine max L.) are one of the main crops for human consumption. In the Western world, the two principal sub-products of soybeans are oil and protein paste. Soy protein is used as a concentrate, an isolate, or is textured, for human consumption. It is a complete protein that contains all the essential amino acids, is low in fat, and free of saturated fat and cholesterol, and is widely used to increase the nutrient density of all types of foods. Furthermore, soybean grains are rich in folate, zinc, iron, and calcium. However, the bioavailability of iron is very low and the value of soy as a source of iron is limited. In contrast, the bioavailability of zinc is around 25%, and that of calcium 20%, which is a lower percentage of calcium than in milk, but relatively good for a plant-based food.11
The quality of soybean protein is greater than that of other grains, almost reaching the level of animal protein, in accordance with the content of essential amino acids.8 The quality of soybean protein is evaluated by taking its biologic value and content, as well as the proportion of essential amino acids, into account. The digestible indispensable amino acid score is calculated by dividing the milligrams of amino acids in a protein by the milligrams of the amino acids in the reference protein. In a study conducted on 70 common foods, soybean grains had a score of 100% and a digestibility-corrected amino acid score of 78% and soy-based drinks had a score of 100% and a digestibility-corrected amino acid score of 86%.12,13 In contrast to milk, soybeans do not contain vitamins A, D, C, or B12 and have a small amount of calcium, iodine, and vitamin B2. As a result, those elements and vitamins are added to many soy-based drinks.8
Non-nutritive componentsSoybeans contain components that have traditionally been considered antinutrients, such as trypsin inhibitors, phytates, and oligosaccharides. Those compounds have recently been thought to be beneficial to health in small quantities and thus are called non-nutritive compounds, given that they are not always harmful.14,15 Trypsin inhibitors interfere with protein digestibility, but boiling soybeans reduces those antinutrients by 80–90%.16 Trypsin inhibitors are being studied for their anti-carcinogenic properties17 and phytates, which contribute to the low bioavailability of minerals in soy, are also being analyzed for their antioxidant effects.15,18 Oligosaccharides, mainly raffinose and stachyose, are responsible for the production of gases due to the fact that the intestinal mucosa does not have the enzyme necessary for hydrolyzing those oligosaccharides. Therefore, they pass into the large intestine without being hydrolyzed, where the bacteria metabolize them and form large quantities of carbon dioxide, hydrogen, and in some cases, methane. In addition, they provide a prebiotic benefit because they promote bifidobacteria growth.13,18
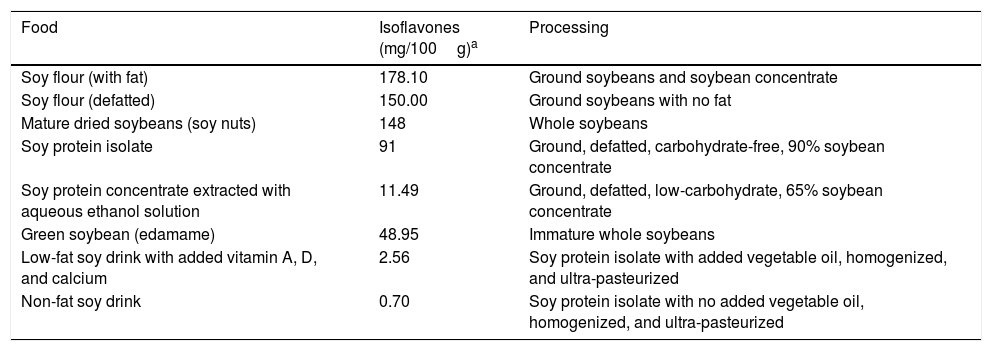
IsoflavonesLegumes are known for their protein and soluble fiber content. Soybeans are special among the legumes due to their high content of phytochemicals, called isoflavones, which are diphenolic molecules that bind to estrogen receptors.13 Isoflavones are natural chemicals that belong to the class of phytoestrogens, or plant-derived estrogens, that act as selective estrogen receptor modulators. They are currently being studied as an alternative therapy to different types of hormonal conditions, as well as for their antioxidant properties and inhibitory actions that intervene in cell replication.13,19 Isoflavones are very similar in chemical structure to mammary estrogens, with binding affinities for estrogen receptors. However, it is complicated to predict the behavior of isoflavones in the body because many factors are involved, such as the mode of administration, the chemical form of the phytoestrogens, their metabolism, bioavailability, half-life, and level of exposure.20,21 Traditional soy products can contain approximately 3.5mg of isoflavones per gram of protein but industrialized soy products can lose up to 80% of their isoflavone content during processing.13 The US Department of Agriculture (USDA) evaluated the isoflavone content of different foods to make recommendations for soybean and soy product consumption, which are described in Table 1.
Isoflavone content in different soy-based products and its relation to the type of processing.
| Food | Isoflavones (mg/100g)a | Processing |
|---|---|---|
| Soy flour (with fat) | 178.10 | Ground soybeans and soybean concentrate |
| Soy flour (defatted) | 150.00 | Ground soybeans with no fat |
| Mature dried soybeans (soy nuts) | 148 | Whole soybeans |
| Soy protein isolate | 91 | Ground, defatted, carbohydrate-free, 90% soybean concentrate |
| Soy protein concentrate extracted with aqueous ethanol solution | 11.49 | Ground, defatted, low-carbohydrate, 65% soybean concentrate |
| Green soybean (edamame) | 48.95 | Immature whole soybeans |
| Low-fat soy drink with added vitamin A, D, and calcium | 2.56 | Soy protein isolate with added vegetable oil, homogenized, and ultra-pasteurized |
| Non-fat soy drink | 0.70 | Soy protein isolate with no added vegetable oil, homogenized, and ultra-pasteurized |
The isoflavone content in foods was obtained from the US Department of Agriculture's Database for the Isoflavone Content of Selected Foods.22
Legumes, including soybeans, are normally processed before being ready for consumption. Processing facilitates their digestibility and attempts to improve their organoleptic properties and reduce or inactivate their undesirable components, as well. Non-thermal processing, such as germination, husking, or fermentation, and thermal processing, such as simple boiling, pressure cooking, and toasting, are commonly utilized for legumes, including soybeans. At the end of the process, to prevent microbial growth, soy-based beverages are thermally treated through pasteurization at 85–90°C for 15s or ultra-pasteurization at 129–143°C for 3–5s. Products that are totally stable at room temperature are treated at 137–142°C for 4–17s.15 All those thermal treatments have an effect on the nutritional quality of the product. Loss of the isoflavone-related cholesterol-reducing effect has been reported for ultra-pasteurized soy drinks.15,23
Homemade beveragesTraditional homemade soy-based beverages have been produced in Asia for hundreds of years. The process is relatively simple and involves minimal processing of soybean grains, thus the nutritional quality of the end product is very similar to that of the unprocessed grains. Nevertheless, by being minimally processed, traditional beverages have less protein digestibility and contain greater quantities of intestinal gas-producing oligosaccharides, as well as a higher content of lectins and trypsin inhibitors, because the proteins are not denaturalized. Isoflavone content, which can be reduced by up to 80% through processing, is also unaffected.13,14,18
Industrialized beveragesCurrently, there are many soy-drink production methods, but in general, they all include the following steps: the soybean grains are soaked and ground, either wet or dried, to extract soy flour. The flour is then filtered or decanted to remove the insoluble lipid components. Soy concentrates and isolates are obtained from that non-fat flour and are the main ingredients in the beverages. They can be mixed with sugar, artificial flavors, and stabilizers.24 Finally, the beverages are homogenized (to have a standardized particle size) and pasteurized or ultra-pasteurized to prevent microbial growth. The final product is a white liquid that resembles cow's milk25 and is packaged in aseptic, non-aseptic, or sterilized containers, giving it a shelf life of up to 6 months.15
The soy concentrate and isolate production process naturally reduces the quantity of available oligosaccharides, because both are derived from non-fat soy flour, to which an alcohol solution responsible for eliminating the oligosaccharides was added, greatly reducing the production of gas in the intestine.24 In addition, the soy concentrate and isolate production process denaturalizes the proteins, increasing their digestibility and reducing the content of lectins and trypsin inhibitors.15,16
Soy concentrates and isolates are being used in the formulations of many beverages for human consumption, targeting different population sectors. The difference between soy concentrates and isolates is in the percentage of proteins. Soy concentrates should contain at least 65% soy protein, and soy isolates should have a final minimum content of 90%.16,24 Soy protein isolate is the purest form of the different commercially available ingredients derived from soybeans. In general, soy protein isolates have an almost neutral flavor and are very easy to digest. Soy drinks stand out among their many uses in foods.15
Evidence on soy plant-based beverages in childrenEffect of soy on heightSome parents decide to give their children plant-based beverages due to the perception that they are healthier options. Nevertheless, the majority of plant-based drinks contain less protein, or protein with a lower biologic value and less fat. Some studies have associated cow's milk consumption during infancy and childhood with an increase in height, an important child growth and development parameter, compared with other beverages. In a study that included 5034 healthy children, the height of the children that drank 3 glasses of non-cow's milk daily was approximately 1.5cm lower than the height of the children that drank 3 glasses of cow's milk per day.26 The limitations of that study were its cross-sectional design, determining associations but not causality, and the fact that the comparison was made with children that consumed 3 glasses of different types of non-cow's milk (goat's milk, soy or rice drinks, etc.). Another meta-analysis and systematic review of 12 studies demonstrated that children that drank cow's milk were taller.27 In a study on 8950 children, DeBoer et al.28 found that taller height was associated with higher cow's milk consumption but no comparison was made with plant-based beverages.28 There is considerable evidence, mainly from developing countries, but also from studies conducted in industrialized countries, that cow's milk stimulates linear growth and that cow's milk consumption plausibly stimulates circulating insulin-like growth factor, thus impacting height.29 There is also evidence that excessive cow's milk protein consumption, especially during a child's first 1000 days, could be associated with a later risk for overweight/obesity.30 Evidence suggests that cow's milk consumption conditions better growth in children, most likely related to the caloric intake that 2 glasses of milk provides per day, which accounts for approximately 30% of the total requirement of a child between 1 and 5 years of age. We must keep in mind that no single food is indispensable from the nutritional perspective, thus it is feasible to have adequate nutrition without milk consumption. Nevertheless, milk is a very complete food from a nutritional and culinary perspective.31 A soy-based drink is the plant-based beverage that provides a protein supply similar to that of cow's milk, but because it has fewer calories and its protein has a lower biologic value, it could condition nutritional risk and lower growth in children that do not meet their daily energy and protein intake requirements. Therefore, each case in which the use of plant-based beverages is being considered must be individualized. Canada's Food Guide states that plant-based drinks should not be recommended for children under 2 years of age because they are low in important nutrients (fat, protein, calories). If utilized after that age, the plant drink that contains at least 6g of protein per glass, is adequately fortified (with at least 30% of the daily recommended value of calcium and vitamin D), and contains less than 10g of sugar per 250mL glass should be chosen and adequate and sufficient diet verified.32 New studies utilizing soy-based drinks are needed to really understand and define whether plant-based beverage consumption could be a cause of lower height, given that the existing studies and case reports compare cow's milk with several plant-based beverages whose nutritional content varies greatly.
Endocrinologic situations: precocious puberty and thyroid alterations?The use of soybean products, in both infant formulas and soy-based drinks, has increased in recent years, with data showing that a good number of infants are fed with soy protein-based formula in the United States.33 As stated above, soy products may contain isoflavones, which can act as weak hormone disrupters because they are functionally similar to mammalian estrogens and their active metabolites.34 In the last few decades, an earlier onset of puberty has been described and the consumption of soybean protein-based products beginning at a young age has been suggested as a possible contributing factor. However, the related data have not been conclusive. Adults that during infancy received either soy formula or cow's milk formula were analyzed retrospectively, and the conclusion reached was that exposure to soy formula did not appear to present general health results different from the exposure to cow's milk protein.35 The study conducted by Sinai et al.36 is the first to prospectively evaluate the association between the consumption of soybean protein-based infant formula and the time of onset of puberty. A total of 89 infants were randomized to receive a soy formula or other formula. The infants were evaluated from birth to three years of age and then re-evaluated at 7.8 years of age and 10.5 years of age. The study showed no association between the consumption of soybean-based infant formula and early puberty.36 A narrative review by Testa et al. showed there was no current, sufficiently solid evidence that soy infant formulas significantly affected human development, reproduction, or endocrine function. Special attention should be given to monitoring thyroid function in children diagnosed with congenital hypothyroidism.37 The authors of a review study concluded that the presently available evidence indicates that soybean foods can be incorporated into the diet of children and adolescents, except for those allergic to soy, which is relatively uncommon. They also found that there was little evidence that soybeans conditioned adverse hormonal effects in children, but the data were limited.13
There is still no overwhelming evidence on the general health effects of long-term consumption of soybean protein-based formulas because not all safety-related problems regarding soy formulas in infants have been conclusively resolved. Further investigation is needed to arrive at definitive conclusions.
Allergy and soyFood allergy arises from a specific immune response induced by the exposure to the proteins of a given food. Food intolerance refers to non-immune reactions caused by unique physiologic characteristics of the individual that include metabolic, toxic, pharmacologic, and undefined mechanisms.38,39 Eight foods are responsible for 90% of food allergies: milk, eggs, soybeans, wheat, peanuts, nuts, fish, and shellfish.40,41 Food allergies to the proteins of cow's milk, eggs, soybeans, and wheat, tend to be transitory, whereas the allergies to peanuts, nuts, fish, and shellfish are usually more persistent.42–44 The first allergic reactions to soybeans were reported in 1934, and incidence is around 0.3%.45 Allergy to soybean protein often begins during the first years of life, with a reaction to soy infant formula. Even though the majority of children overcome soy allergy, it can continue into adulthood. Around 28 soybean proteins are recognized by IgE in patients with soy allergy,46,47 but only some of those proteins have been recognized as allergens. The major soy allergen is a subject of debate, given that different studies identify different proteins (a major allergen is that which is recognized by more than 50% of the population studied).48 According to the International Union of Immunological Societies, the following proteins are officially accepted as soy allergens: Gly m Bd 30K (cysteine protease), Gly m 3 (a profilin), and Gly m 4 (a PR-10 protein), which are associated with oral allergy syndrome; and the hydrophobic hull proteins, Gly m 1 and Gly m 2.49–52 Other soybean proteins also characterized as allergens include the Gly m 5 (β-conglycinin) and Gly m 6 (glycinin) reserve proteins, the trypsin inhibitor (Gly m TI), and the 2S soy albumin (Gly m 2S). The two main soy storage proteins, β-conglycinin and glycinin, are the 7S and 11S globulins, and they account for around 30% and 40% of the total protein of the seed, respectively. Sensitization to both allergens is a potential indicator of severe soy allergic reaction. The aeroallergens identified in soybeans are hydrophobic proteins found in the hull, the most important of which are Gly m 1 and Gly m 2.53,54 Soy allergy can also develop secondary to the initial sensitization to another allergen, as a result of cross-reactivity. A retrospective analysis of the levels of IgE specific for aeroallergens and food allergens in 273 children revealed that sensitization with IgE to soy in early infancy (caused by food ingestion) is not very common. Sensitization with IgE is more frequent in school-age children and is caused by the primary sensitization through pollen inhalation.55 Children with soy allergy have been reported to develop tolerance as follows: 50% at one year of age and 67% at 2 years of age. However, more recent studies state that said tolerance can be reached at later ages.38,39 Soy drinks can be tolerated by children with cow's milk protein allergy (CMPA) that do not have a concomitant soybean protein allergy. It is important to remember that soy drinks are not a treatment for CMPA and should not be considered a milk substitute in children with CMPA during the first two years of life.
In summary, there is no evidence on the health benefit of plant-based beverages in childhood nutrition. Given the above information, and in an effort to prevent nutritional problems, the technical opinion group of the AMG emphatically states that plant-based beverages should not be utilized as a replacement for breastmilk or as a replacement for breastmilk substitutes in the feeding of children during the first two years of life. Their later use as part of the liquid portion of diet must be individualized, but in no way can plant-based beverages be the main source of nutrition in the pediatric stage.
Soy beverages and the microbiotaThe gut microbiota plays an important role in general health, and diet is one of the main determining factors of its composition.56 There is some evidence on the consumption of soy drinks and its effect on the composition of the gut microbiota.
In a murine model, Lee et al.57 studied whether a mixture of soy drink and fiber could attenuate changes in the gut microbiota and in inflammation induced by a high cholesterol diet. Soy drink administration was associated with improvement in serum HDL cholesterol levels and of the colonic expression levels of genes in tight junction proteins (ZO-1 and occludin) and inflammation-related proteins (IL-1β, IL-10, and Foxp3). They also reported that the Firmicutes to Bacteroidetes ratio increased due to a greater proportion of Lactobacillus spp.
Fernández-Raudales et al.58 evaluated the consumption of 250mL of a conventional soy drink, a low glycinin soy drink, and bovine milk for 3 months in men with overweight and obesity (BMI 25–40kg/m2) and found that the total bacteria increased in the three groups over time. However, the composition of the microbiota was modified in a potentially beneficial manner in the soy drink consumers due to the decrease in the relative abundance of Firmicutes and the increase in Bacteroidetes, resulting in a final decrease in the Firmicutes to Bacteroidetes ratio. The relative abundance of the phylum Proteobacteria increased significantly in the three groups. Inoguchi et al.59 assessed the effect on the microbiota of the consumption of a conventional soy drink and a fermented soy drink (100g/day) for two weeks and found that the number of bifidobacteria y lactobacilli increased, whereas the number of Clostridia decreased significantly, but only with the fermented soy drink intake. Despite those data, there is still not enough evidence on the impact of soy drink consumption on the composition of the gut microbiota. Importantly, in Mexico, soy drinks are not fermented, nor is fiber added to them, making it impossible to issue a general recommendation.
Soy beverages and lactose intoleranceAn adverse reaction to a food is any abnormal clinical response to its ingestion and can be due to food hypersensitivity or intolerance. Hypersensitivity has a proven immunologic cause and can occur even with the intake of small quantities of the food. Food intolerance, which includes metabolic intolerance, is due to the absence of a digestive enzyme. Such is the case of lactose intolerance, which is characterized by the decrease in or absence of intestinal lactase, and the symptoms are dependent on the dose of lactose.60 CMPA is not frequently diagnosed in adults,61 but lactose intolerance is a genetically programmed entity that affects 70% of the world population.62 Non-hydrolyzed lactose is metabolized by the non-anaerobic microbiota of the colon, causing an increase in the osmotic load. That can be remedied by utilizing products that have been modified to reduce lactose content or products to which the enzyme, lactase, has been added. Lactase tablets can also be simultaneously ingested with the lactose-containing food, or non-dairy beverages that lack said molecule, such as soy drinks, can be consumed. A systematic review of the literature showed that having a primary lactase deficiency was associated with lower bone mineral density in postmenopausal women.63 Postmenopausal women that had a greater risk for fractures were also reported to have low milk intake in childhood,64 indicating the need to include a good calcium supplement in the diet of that specific group. An alternative, apart from lactose-free dairy products, could be the consumption of soy drinks with added calcium because it is the non-dairy drink with the nutritional contribution that is most similar to cow's milk.65 Supplemented soy drinks provide similar quantities of calcium and vitamin D to those of milk8 but there are no reports on the use and effectiveness of soy drinks as milk substitutes in that context. Until there are sufficient studies, soy drinks with added calcium can be used in patients with lactose intolerance, according to patient preferences, as part of an adequate and balanced diet. However, soy drinks cannot be utilized as the only source of calcium and each case must be evaluated individually.
Soy beverages and irritable bowel syndromePatients have long associated irritable bowel syndrome (IBS) symptoms with the ingestion of specific foods or their combinations, and dairy products, fructose, wheat products, and caffeine are among the most common. Twenty to 67% of individuals with IBS complain of subjective intolerance to foods and more than 60% complain of the worsening of symptoms after meals.66 That has led to the implementation of dietary restrictions that are self-imposed or suggested by healthcare personnel.67–69 Milk is one of the foods most frequently eliminated from the diet of patients with IBS, even when there is no objective evidence of lactase deficiency, given that those patients are prone to be more sensitive to the effects of lactose.62 Although efforts have been made to improve tolerance and induce adaptation to dairy products, data are insufficient for supporting the efficacy of milk with reduced lactose content, probiotics, incremental lactose administration, or raw milk, for that purpose.70,71
An alternative for substituting milk consumption in those patients could be the use of soy drinks, taking into account their nutritional characteristics. However, there are no studies describing their tolerance, clinical utility, and possible consumption effects in subjects with IBS. There is evidence suggesting that supplementation with soybean isoflavones could improve the quality of life of patients with IBS, but symptom severity was not significantly suppressed after 6 weeks of consumption.72 Nevertheless, the isoflavone content in the majority of soy drinks is low.
Two important aspects should be considered in relation to soy drink consumption in patients with IBS: the theoretic possibility of triggering food allergies and their high content of the short-chain carbohydrates known as FODMAPs (fermented oligosaccharides, disaccharides, monosaccharides, and polyols) that are not completely absorbed. Even though up to 25% of the general population believes they have a food allergy, it has only been confirmed in 0.3–6% of adults.73 Food allergy is present in 4% of the patients with functional gastrointestinal disorders and the proportion of the total population of patients with IBS with a true food allergy is very low.74–77 Soy does not stand out among the major allergens or triggering factors of food allergies in adults. Added to the fact that there is little evidence that IBS patients with food-related complaints actually present with a true food allergy, the use of soy drinks can be an option in that digestive disorder.
FODMAP fermentation produces gas and a greater liquid load with secondary luminal distension that involves the distal small bowel and the proximal colon. There is evidence that a low FODMAP diet can have a favorable impact on IBS symptoms, especially pain and bloating.78 However, the characteristics of the subjects enabling us to predict who would respond to the diet have not been defined, nor has that diet been shown to be superior to other diets habitually utilized in IBS. Therefore, its implementation is optional, not obligatory.79 Even taking into account their possible beneficial effects, soy drinks cannot be included in that diet due to their high FODMAP content. Consequently, soy drinks can be an acceptable nutritional alternative for those patients with IBS that are lactose intolerant but keeping their high FODMAP content in mind.
Soy beverages in dyspepsia and other gut-brain interaction disordersThere are no studies on consumption frequency, tolerance, clinical utility, and possible effects of soy drinks in relation to dyspepsia and other functional gastrointestinal disorders. The implications of their use in those illnesses are similar to those described for IBS.
Soy beverages in liver diseasesTheoretically, soy drinks are an acceptable dietary option in patients with chronic liver failure due to their high content of plant-based protein and low content of methionine. They can be part of a balanced diet in those patients after an individualized nutritional evaluation of each case.
The nutritional profile of soy drinks also makes them a potentially beneficial element, together with a low-calorie diet, for the comprehensive treatment of patients with nonalcoholic fatty liver disease that require such a measure. However, there is little evidence on the topic. Eslami et al.80 conducted a clinical study on 70 patients with nonalcoholic fatty liver disease that were randomized into two different groups to receive an 8-week dietary treatment: the patients in the active group consumed 240mL of a soy drink daily as part of a low-calorie diet, whereas the patients in the control group only followed a low-calorie diet. At the end of the study, the group treated with the soy drink showed a significantly greater reduction of serum alanine aminotransferase and serum high-sensitivity C-reactive protein, compared with the control group. Nevertheless, the changes in other liver enzymes (including aspartate aminotransferase, alkaline phosphatase, and gamma-glutamyl transpeptidase), as well as the lipid profile and anthropometric indexes, were not significantly different between the two groups. Therefore, more evidence needs to be developed in that area before a recommendation can be made.
ConclusionsAt present, the scientific evidence on plant-based beverages is limited. Plant-based beverages, including soy drinks, are not a replacement for breastmilk or breastmilk substitutes. Plant-based beverages are not recommended as the main diet in infants, i.e., during the first two years of life. From a nutritional perspective, plant-based beverages in general, cannot be considered substitutes for cow's milk. The nutritional content of plant-based beverages depends on the type of drink and the brand. Soy drinks are considered safe and can enrich the varied diet of its consumers, as long as they are simply one more liquid portion of the diet, and not the primary source of nutrition. In vulnerable populations, such as preschool and school-age children, adolescents, and older adults, plant-based beverages should be fortified and form part of a correct diet, otherwise there can be nutritional deficiencies. Plant-based beverages can be consumed by pediatric patients above 2 years of age and adult patients that present with CMPA or lactose intolerance, as part of the liquid portion of their diet. More studies on soybean plant-based beverages are needed before recommendations about their beneficial effects on health can be made.
Financial disclosureThe scientific agenda, discussion, and conclusions of the present review were autonomously determined and drafted independently by the members of the group summoned by the Asociación Mexicana de Gastroenterología (AMG).
Strictly for purposes of logistics, the AMG requested and obtained funds from the Instituto de Bebidas de la Industria Mexicana de Coca-Cola.
Conflict of interestRVF: has received financial support to attend congresses and speaking fees from Nestlé®, Sanofi®, Carnot®, BioGaia®, Abbott® Farmacéutica, and Nutricare®.
MEIC: has received financial support to attend congresses and speaking fees from Asofarma® and Takeda®.
MARC: has received financial support to attend congresses from Nestlé®.
MAB: Has been a speaker for Menarini®, Sanfer®, and Taqueda®.
GAAA: has received financial support to attend congresses and speaking fees from Nestlé® and Carnot®.
RICS: is a member of the advisory board of Asofarma®, ponente para Mayoly-Spindler® and a speaker for Asofarma® and Chinoin®.
MVFB, GHV, IMV, EMB, and BAPN: declare there is no conflict of interest.
VHR: has received financial support to attend congresses and speaking fees from Nestlé®.
INB: has received speaking fees from Baxter ® and ASPEN®.
CASR: has received financial support to attend congresses from Nestlé®.
Please cite this article as: Vázquez-Frias R, Icaza-Chávez ME, Ruiz-Castillo MA, Amieva-Balmori M, Argüello-Arévalo GA, Carmona-Sánchez RI, et al. Posición técnica de la Asociación Mexicana de Gastroenterología sobre las bebidas vegetales a base de soya. Revista de Gastroenterología de México. 2020;85:461–471.

