
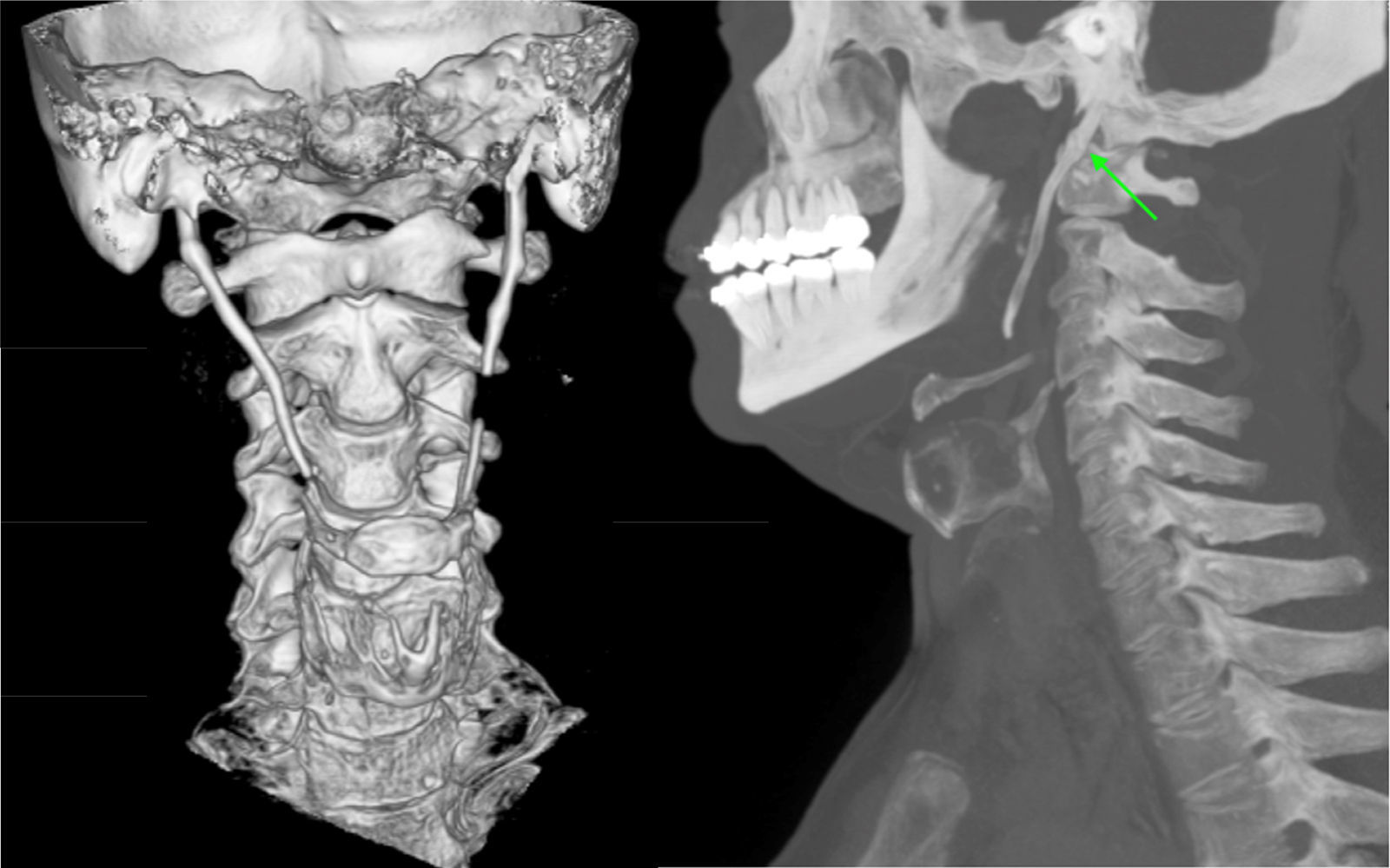
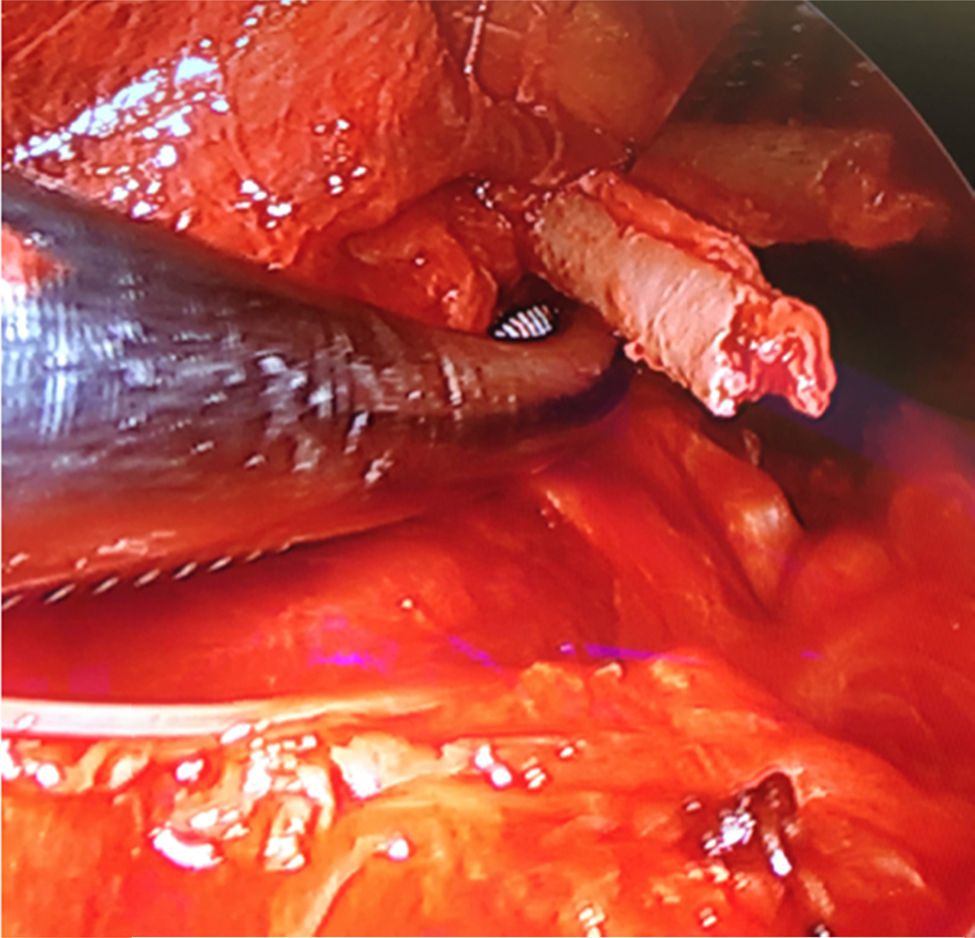

A 57-year-old man with an unremarkable past history sought an otorhinolaryngology consultation for symptoms of oropharyngeal dysphagia and an ever-increasing sensation of a foreign body. Physical examination and fiberoptic nasopharyngoscopy were normal, and so an extension study was carried out. The computerized tomography scan of the neck showed a lengthening of both styloid apophyses, 5cm on the left side and 7cm on the right (Fig. 1). The patient was diagnosed with Eagle syndrome. Given the disease progression and the patient's clinical progression, we decided to resect both styloid apophyses and posterior hyoid horns (Figs. 2 and 3). The patient had satisfactory postoperative progression.


 and both horns of the hyoid bone (lower part of the image).")
Eagle syndrome, first described in 1937, is an entity with characteristic symptomatology caused by the elongation of the styloid apophyses. There is a 3.3% prevalence of elongations of the styloid apophyses, and 4% of those cases may present with symptoms.1,2 In Eagle syndrome, said elongations can be accompanied with pharyngeal pain, oropharyngeal dysphagia, the sensation of a foreign body, orofacial pain, and ATM dysfunction and/or carotidynia.1,2 Conventional radiologic studies can reveal the elongation of the styloid apophyses, but computed tomography provides a better description of the anatomic structures and improved preoperative planning.1,3 Treatment of this entity depends on the patient's symptoms, and the treatment of choice is resection of the styloid apophyses.1
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Benet-Muñoz S, Tacoronte-Pérez L, Fernández-Belda R, Artazkoz-del Toro JJ. Síndrome de Eagle como causa infrecuente de disfagia. Revista de Gastroenterología de México. 2017;82:257–258.

