
The predictive scale for mortality risk in patients with nonvariceal upper gastrointestinal bleeding (NVUGIB) proposed by Italy's PNED (Progetto Nazionale Emorragia Digestiva) group has not been validated in Latin America since its original publication.
AimTo compare the PNED system and the Rockall score as mortality predictors in patients hospitalized for NVUGIB.
Material and methodsA multicenter, prospective, cross-sectional, analytic study was conducted that recruited patients diagnosed with nonvariceal upper gastrointestinal bleeding within the time frame of 2011 to 2015. Six Mexican hospital centers participated in the study. The Rockall and PNED system scores were calculated, classifying the patients as having mild, moderate, or severe disease. The association between mortality and risk was determined through the chi-square test and relative risk (RR) calculation. Statistical significance was set at a P<.05.
ResultsInformation on 198 patients was collected. Only 8 patients (4%) died from causes directly associated with bleeding. According to the Rockall score, 46 patients had severe disease (23.2%), 5 of whom died, with a RR of 5.5 (CI 1.35-22.02, P=.006). In relation to the PNED, only 8 patients had severe disease (4%), 5 of whom died, with a RR of 38.7 (CI 11.4-137.3, P=.001).
ConclusionsThe PNED system was more selective for classifying a case as severe, but it had a greater predictive capacity for mortality, compared with the Rockall score.
El grupo Progetto Nazionale Emorragia Digestiva (PNED) de Italia publicó su propuesta de escala predictora de riesgo de mortalidad en pacientes con hemorragia digestiva alta no variceal (HTDANV), que desde su publicación no ha sido validada en Latinoamérica.
ObjetivoComparar el sistema PNED contra la escala de Rockall en la predicción de mortalidad de pacientes hospitalizados por HTDANV.
Material y métodosEstudio multicéntrico prospectivo, transversal, analítico, en el cual se reclutó a pacientes con diagnóstico de hemorragia de tubo digestivo alto no variceal del 2011 al 2015. Se contó con la colaboración de 6 centros hospitalarios mexicanos. Se calculó la puntuación por escala Rockall y por sistema PNED, clasificando a los pacientes en enfermedad leve, moderada o severa. Finalmente, se determinó la asociación entre mortalidad y riesgo mediante aplicación de la χ2 y con cálculo de riesgo relativo (RR), con una p significativa al presentar valor menor de 0.05;
ResultadosSe recolectó información de 198 pacientes. Solo 8 pacientes (4%) fallecieron por causas directamente asociadas con la hemorragia. Al aplicar escala Rockall, 46 pacientes alcanzaron puntuación de enfermedad severa (23.2%), de los cuales 5 fallecieron, con un RR de 5.5 (IC 1.35-22.02, p=0.006). En cuanto a PNED, solo 8 pacientes alcanzaron puntuación de enfermedad severa (4%), de los cuales 5 fallecieron, con un RR de 38.7 (IC 11.4-137.3, p=0.001).
ConclusionesEl sistema PNED fue más selectivo para calificar un caso grave, pero tuvo mayor capacidad de predicción de mortalidad comparado con la escala Rockall.
Nonvariceal upper gastrointestinal bleeding is a medical emergency managed by gastroenterologists, with an incidence of up to 150 cases per 10,000 inhabitants and presenting as melena or hematochesis.1 The presence of the latter is an indicator for important blood loss,2 and is more commonly found in bleeding of the lower digestive tract.1
Mortality associated with gastrointestinal bleeding appears to be related to advanced age and coexisting diseases, among other things, as opposed to the bleeding per se.3 Chronic diseases, such as high blood pressure, chronic obstructive pulmonary disease, type 2 diabetes mellitus, cirrhosis of the liver, and chronic renal insufficiency, are associated with the development of peptic ulcer and its complications.4
The aim of our study was to compare the PNED system with the Rockall score, as mortality predictors in patients hospitalized for nonvariceal upper gastrointestinal bleeding.
Materials and methodsType of studyMulticenter, prospective, cross-sectional, analytic.
Sample sizeThe study sample was a convenience sample that included all the patients diagnosed with nonvariceal upper gastrointestinal bleeding hospitalized at the participating centers within the time frame of the analysis.
MethodologyPatients diagnosed with nonvariceal upper gastrointestinal bleeding within the time frame of May 2011 and May 2015 were recruited. The following Mexican hospital centers participated in the study: Antiguo Hospital Civil de Guadalajara Fray Antonio Alcalde, Hospital Regional “Lic. Adolfo López Mateos” ISSSTE in Mexico City, Hospital Regional 220 IMSS of Toluca, Unidad Médica de Alta Especialidad IMSS in Yucatán, Hospital General de Zona y Medicina Familiar No.1 IMSS Hidalgo, and Hospital General de Pachuca SSA. The clinical and demographic data of all the patients were obtained using a specifically designed collection sheet with a special focus on mortality cases.
The other baseline characteristics obtained in accordance with the Non-variceal Upper Gastrointestinal Haemorrhage clinical guidelines were: physical examinations and laboratory data (hemodynamic data, rectal examination, nasogastric probe, complete blood count, and coagulation times), age, state of shock, comorbidities (diabetes, high blood pressure, neoplasias),5 as well as endoscopic findings (Forrest stage Ia, Ib, IIa, and IIb gastric and duodenal ulcers,6–8 erosive gastropathy, esophagitis according to the Los Angeles classification, among others), progression time, the time lapse until endoscopy, endoscopic treatment, intrahospital complications and mortality, and hospital stay. All the elements necessary for calculating the Rockall and PNED scores were documented.9
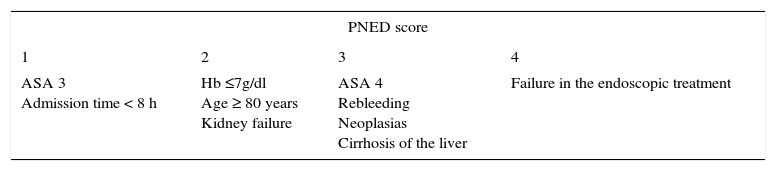
The PNED risk scores for patients were calculated by adding together the points of all the variables present. The result was 0 (zero) when the patients had none of the identified risk factors. The patients were divided into high-risk, intermediate-risk, and low-risk groups, based on their scores. The patient mortality risk profile was divided into low (score of 0-4), intermediate (score of 5-8), and high (score>8) (Table 1).10
PNED score.
| PNED score | |||
|---|---|---|---|
| 1 | 2 | 3 | 4 |
| ASA 3 Admission time < 8 h | Hb ≤7g/dl Age ≥ 80 years Kidney failure | ASA 4 Rebleeding Neoplasias Cirrhosis of the liver | Failure in the endoscopic treatment |
ASA: American Society of Anesthesiology; Hb: Hemoglobin; PNED: National Project of Digestive Bleeding (Italian acronym)
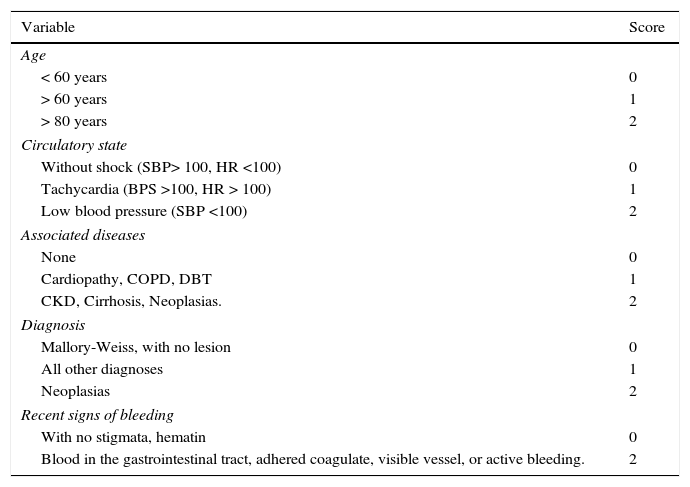
The Rockall risk scores were calculated by adding together the points of the variables present. The result was 0 (zero) when patients had none of the identified risk factors. The patients were divided into high-risk, intermediate-risk, and low-risk groups, based on their scores. The patient mortality risk profile was divided into low (score of 0-2), intermediate (score of 3-4), and high (score>5) (Table 2).11
Rockall score.
| Variable | Score |
|---|---|
| Age | |
| < 60 years | 0 |
| > 60 years | 1 |
| > 80 years | 2 |
| Circulatory state | |
| Without shock (SBP> 100, HR <100) | 0 |
| Tachycardia (BPS >100, HR > 100) | 1 |
| Low blood pressure (SBP <100) | 2 |
| Associated diseases | |
| None | 0 |
| Cardiopathy, COPD, DBT | 1 |
| CKD, Cirrhosis, Neoplasias. | 2 |
| Diagnosis | |
| Mallory-Weiss, with no lesion | 0 |
| All other diagnoses | 1 |
| Neoplasias | 2 |
| Recent signs of bleeding | |
| With no stigmata, hematin | 0 |
| Blood in the gastrointestinal tract, adhered coagulate, visible vessel, or active bleeding. | 2 |
CKD: Chronic kidney disease; COPD: Chronic obstructive pulmonary disease; DBT: Diabetes; HR: Heart rate; SBP: Systolic blood pressure
The demographic data were described through measures of central tendency and dispersion. The association between mortality and the instrument scores were obtained through the chi-square test and the relative risk (RR) calculation. Statistical significance was set at a p value under 0.05.
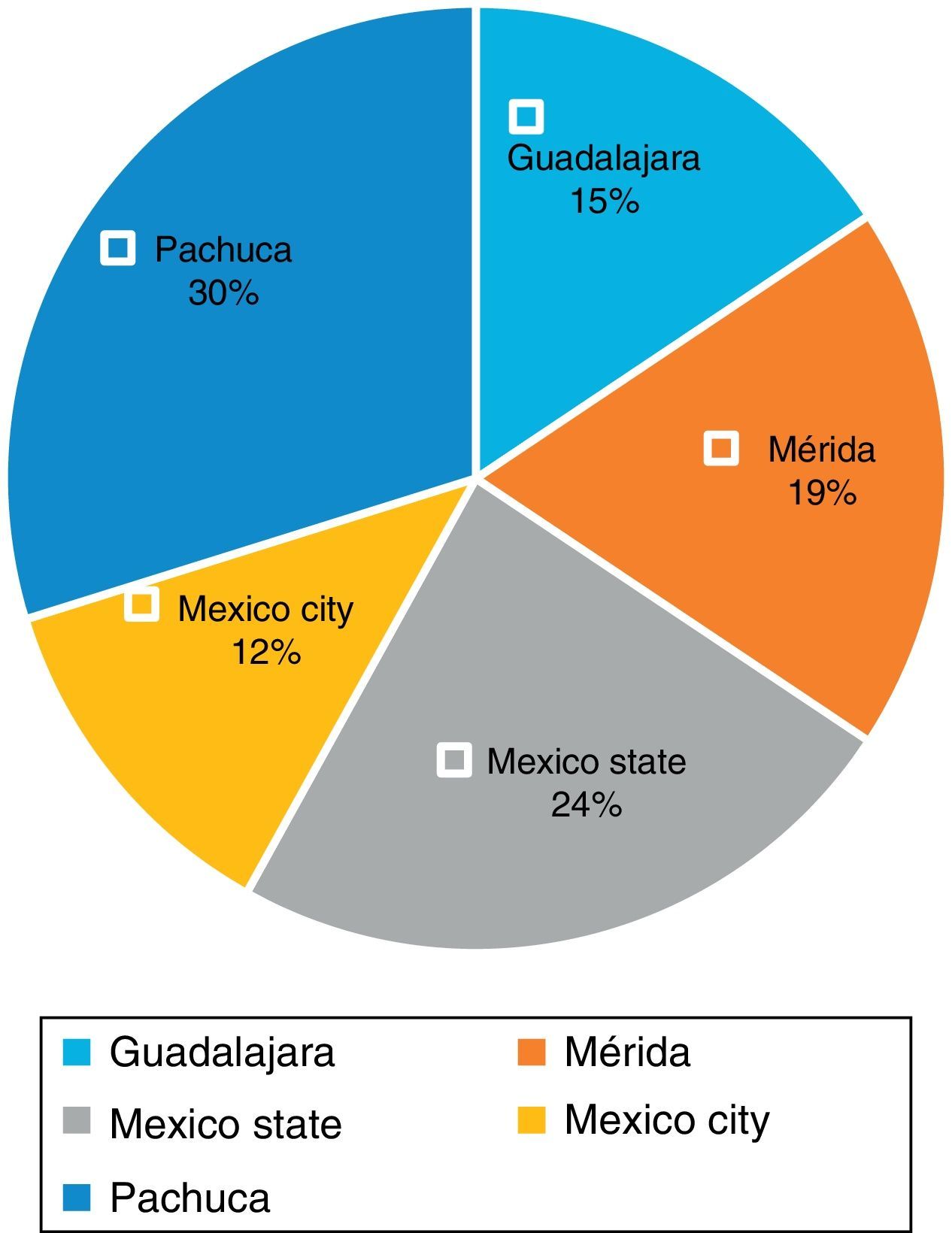
ResultsInformation was obtained from a total of 198 patients seen at different Mexican hospitals. The 36% majority of the study patient total was from the State of Mexico and Mexico City (CEMCAM and Hospital Regional Lic. Adolfo López Mateos of the ISSSTE), followed by 30% seen at the Hospital General SSA and the HGZMF1 IMSS Pachuca, 19% at the Unidad Médica de Alta Especialidad IMSS in Mérida, Yucatán, and 15% at the Hospital Civil Fray Antonio Alcalde in Guadalajara (fig. 1).

Of the 198 patients, 54% were men and 46% were women.
Patient age ranged from 40 to 79 years, and the 70-79 year age group predominated. The mode was 71 years, the median was 62 years, and the mean was 56 years.
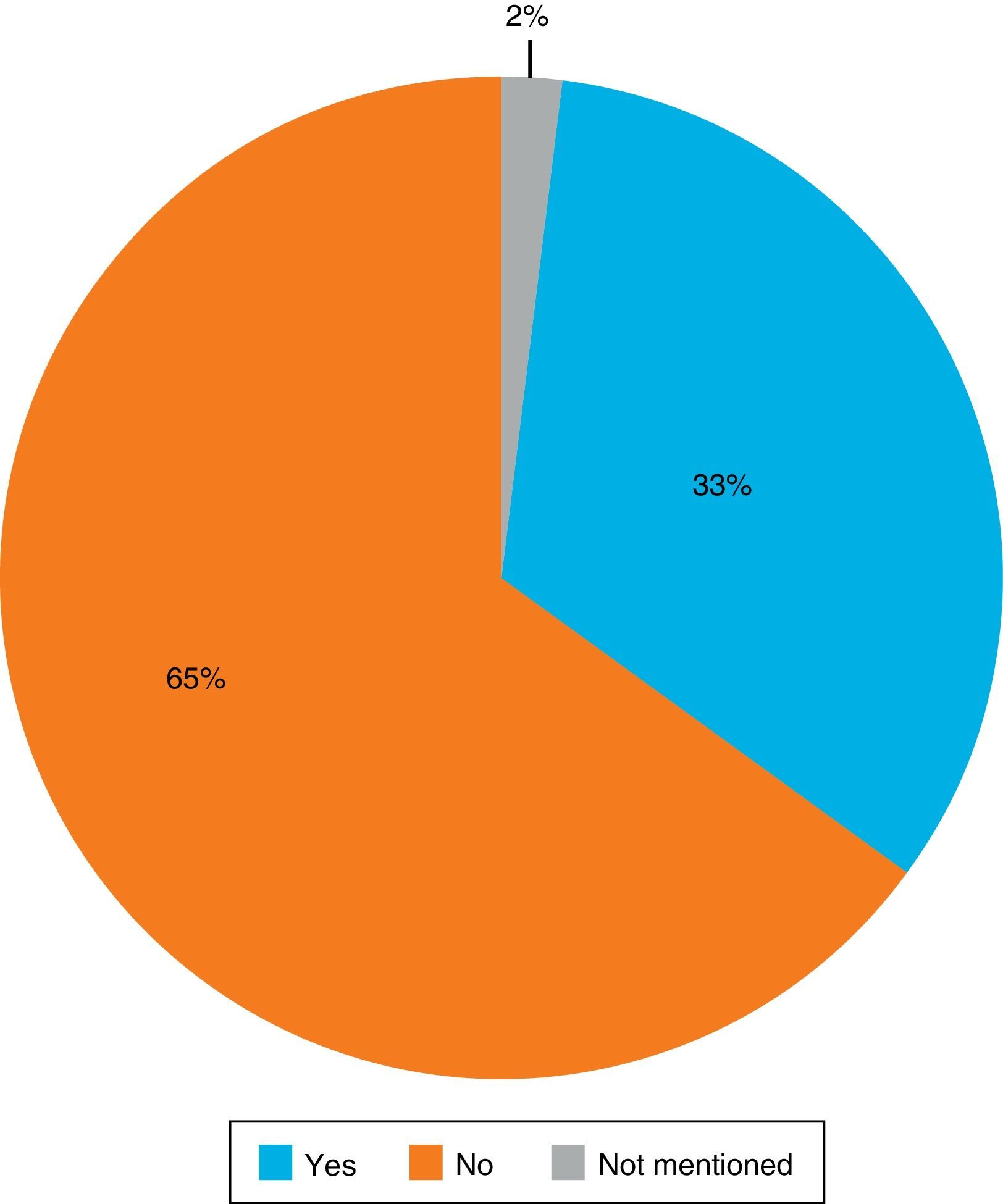
Of the patient total, 33% took NSAIDs for a prolonged period of time. Among the most widely used medications were aspirin, ketorolac, diclofenac, and ibuprofen. Twelve percent of the patients stated that they took anticoagulants or antiaggregants, such as aspirin, clopidogrel, and acenocoumarol (fig. 2).

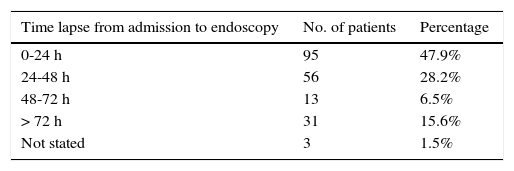
The time lapse from emergency room admission to the performance of endoscopy to determine the cause of bleeding was from 0 to 24h in 48% of the patients. However, it was striking that there was a mean of 2 days before endoscopy, and the time lapse in 22.1% of the patients was 72h or more (Table 3).
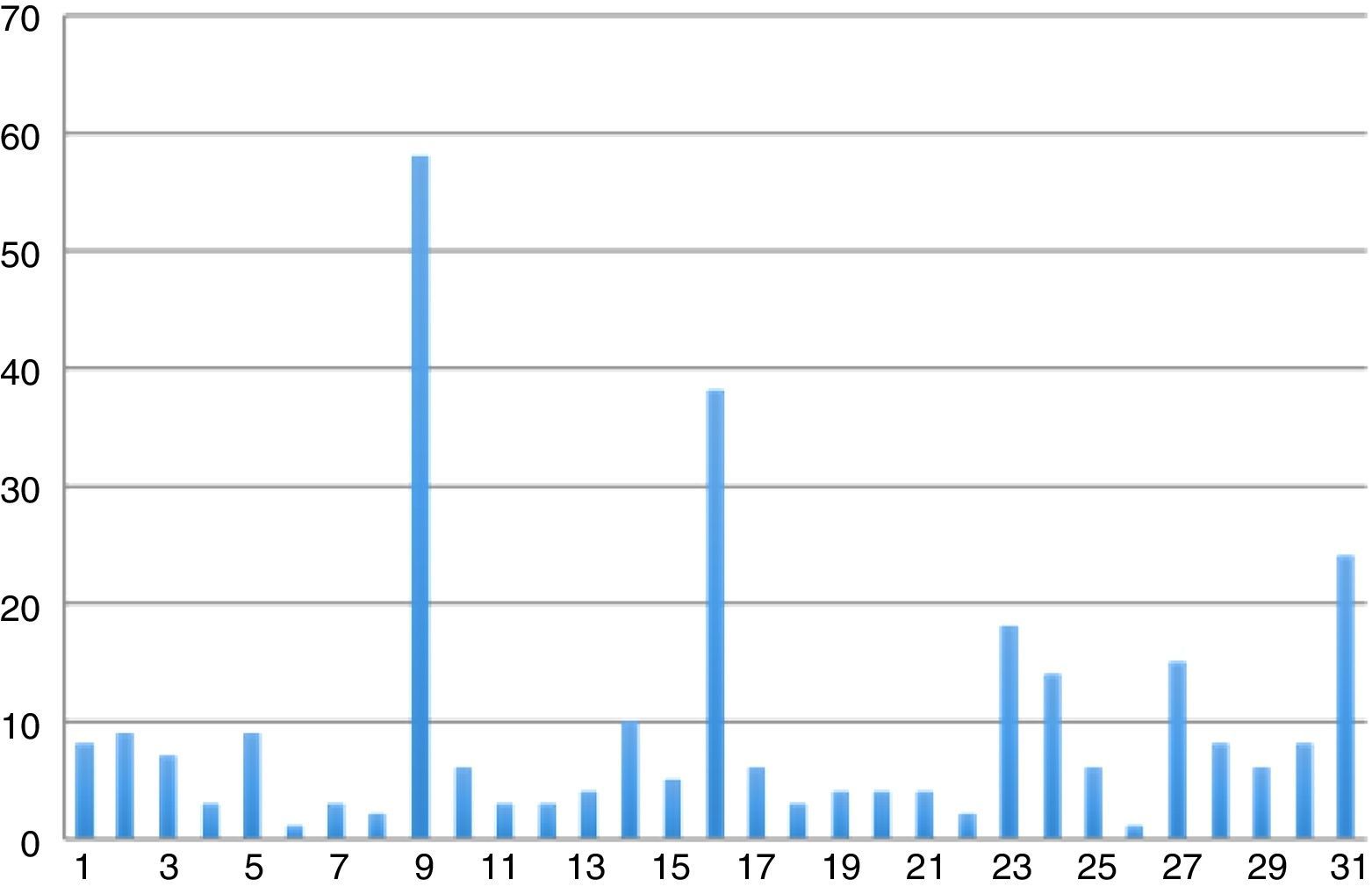
Figure 3 shows the most frequent endoscopic findings. There was a high incidence of erosive gastropathy (58 patients, 29.2%), followed by Forrest III gastric ulcer (38 patients, 19.1%), and Forrest III duodenal ulcer (18 patients, 9%) (fig. 3).

Twenty-five percent of the patients were admitted to the emergency room with hemodynamic instability.
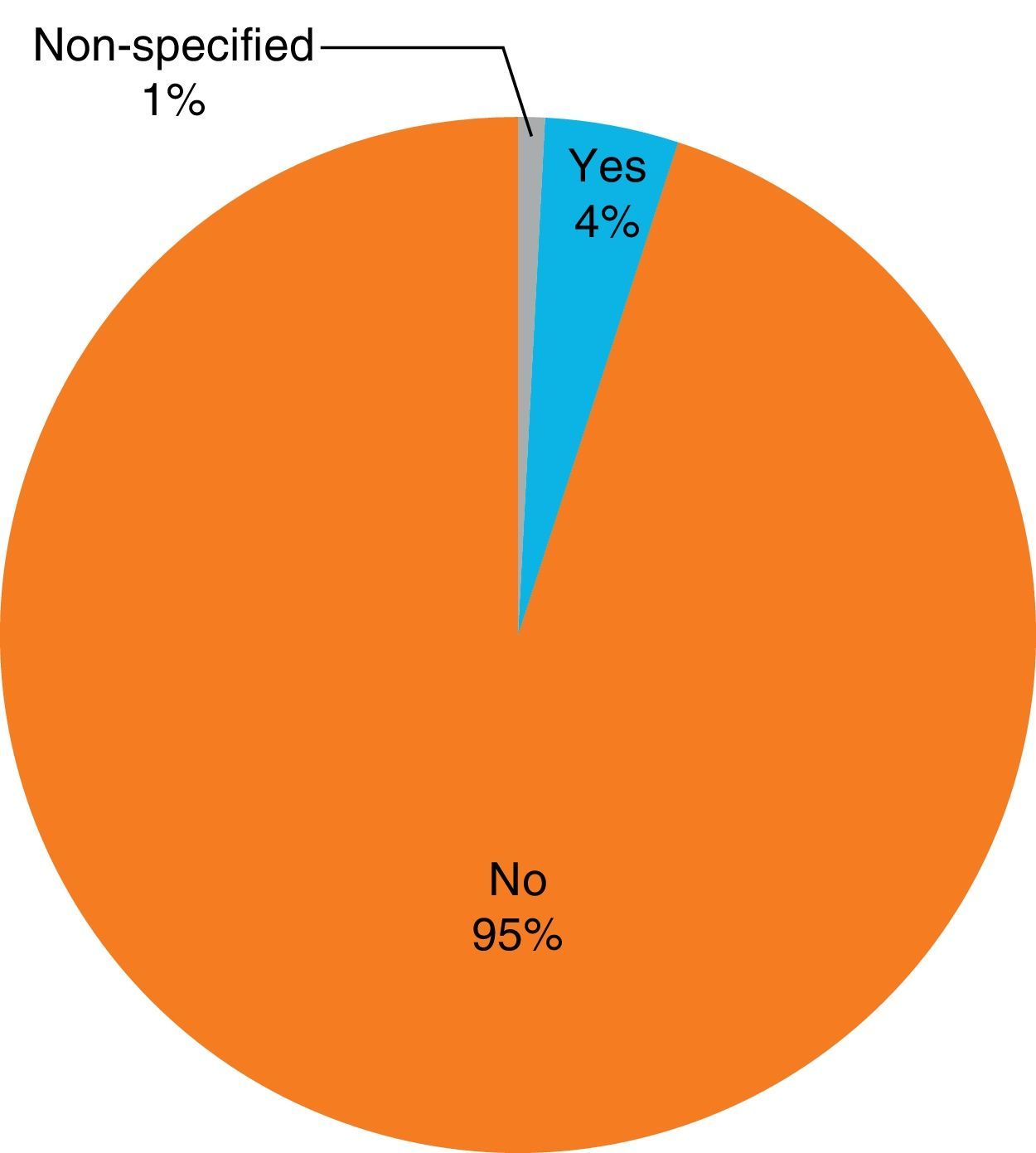
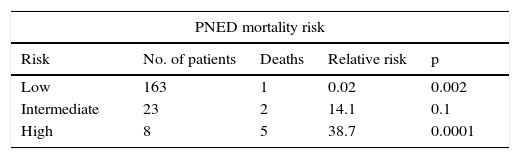
In relation to mortality, 8 (4%) of the 198 recruited patients died. The most frequent cause of death was refractory hypovolemic shock. Other causes were multiple organ failure and uncontrolled arrhythmias (fig. 4).

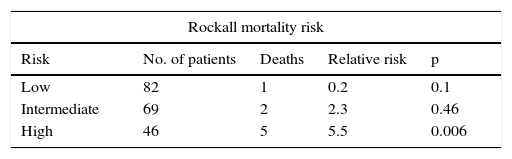
In patients with a low or intermediate-risk Rockall score, the RR mortality prediction was not significant. Nevertheless, the RR for mortality in the high-risk scores was 5.5 (p=0.006, CI: 1.3-22) (Table 4).
In comparison, the PNED score results showed that the RR in patients with low and intermediate-risk scores had little predictive value. However, the RR in the patients with a high-risk score was 38.7 for intrahospital mortality (p=0.0001, CI: 11-134) (Table 5).
DiscussionUpper gastrointestinal bleeding is a potentially critical emergency and continues to be one of the most frequent causes of hospitalization in digestive pathology.
As proposed by Zepeda-Gómez,12 a requisite of our study was registering the patients only if they had undergone gastrointestinal endoscopy.
In relation to this, a second endoscopy was performed solely when the first diagnosis was incorrect or if there was intrahospital rebleeding. Contreras-Omaña et al.1 suggest that bleeding should be confirmed by a second endoscopy.
One of the first important findings of our study indicates that in Mexico, more than 48h go by from the time patients are admitted until the performance of endoscopy in up to one fifth of the cases, at least double the internationally recommended 12 to 24h. Establishing a recommendation to improve access to emergency endoscopy services in referral centers, thus reducing the complications in these cases, is imperative.
In our case series, mortality reached 4% of the case total. This figure is smaller that that reported in the international literature (8 to 10%), which appears to indicate that both the emergency room care and hospital management that these patients receive is generally optimal.13
Since the original publication of the PNED system, it has not been validated in Latin America, making our study the first multicenter, prospective analysis conducted in Mexico on nonvariceal upper gastrointestinal bleeding that compares the prognostic value of the PNED score with another scoring system. The 2010 study by Antonio-Manriquez et al.14 had a larger number of patients, but it compared the Rockall score with the Blatchford score, which depends on clinical factors. Likewise, the focus of the 2010 study by Pavez-Ovalle et al.15 was only on the Rockall score, which, as shown in our study, easily classifies a patient as having “severe” pathology. The PNED system appears to be more selective in determining severity and to have a greater positive predictive value in the Mexican population, making its comparison worthwhile.
In 2008, Marmo et al.10 conducted a study to validate the PNED score in the United States. Even though their study time frame was shorter than ours (16 months), the PNED score was superior for that study's population.
Our study was carried out over a 4-year period for the purpose of obtaining a national sample with greater statistical representation. However, data was obtained from only 198 patients, and so we suggest a follow-up of the present validation with the collaboration of more hospital centers in Mexico.
It is important to emphasize that in our study, despite the fact that there was a wide range between the confidence intervals of the two scoring systems because of the number of patients in our sample, the two RRs for the high-risk scores were highly significant. Nevertheless, the RR of the Rockall score was 5.5, whereas the RR for the PNED score was 38.7, making it a 7.03 times greater mortality predictor than the Rockall score for the population studied at different points in Mexico. This leads us to believe that even if the sample size were larger, the difference between the two prediction values would still be large enough that there would be no important modifications.
Nevertheless, the fact that there is no well-established criterion standard means there is no single reference, making any result incomplete. This is why we strongly insist that further studies be conducted until a general consensus for our environment is reached. Our research center is currently carrying out a new study protocol with this in mind.
ConclusionsIn conclusion, we found that the PNED system appeared to be more selective in considering a case as being severe, and had a greater mortality prediction capacity in high scores, compared with the Rockall score. Measures should be established in referral centers in our country to improve the access to endoscopy services for these patients, given that one fifth of them received that attention as late as 48 to 72h. To the best of our knowledge, ours is the first multicenter, prospective study on nonvariceal upper gastrointestinal bleeding conducted in Mexico and is also the first external validation of the PNED system in Latin America. We suggest that more studies on these scoring systems be carried out in Mexico to compare our results.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.
The authors wish to thank all the specialists in the areas of gastroenterology and endoscopy from the different collaborating hospital centers for their valuable participation so that this study could be carried out.
Please cite this article as: Contreras-Omaña R, Alfaro-Reynoso JA, Cruz-Chávez CE, Velarde-Ruiz Velasco A, Flores-Ramírez DI, Romero-Hernández I, et al. Sistema Progetto Nazionale Emorragia Digestiva (PNED) vs. escala de Rockall como predictores de mortalidad en pacientes con hemorragia de tubo digestivo alto no variceal: un estudio multicéntrico prospectivo. Revista de Gastroenterología de México. 2017;82:123–128.

