


¿ Introduction
Achalasia is a primary esophageal motility disorder of unknown etiology, defined manometrically by the absence of esophageal peristalsis and abnormal lower esophageal sphincter (LES) relaxation; symptoms referred more frequently are persistent dysphagia, chest pain and/or regurgitations.1 Achalasia affects both genders equally and has a bimodal age of onset, typically occurring between the third and fifth decades or after 60 years of age.2 Due to the low frequency of this disease, the epidemiologic information is still scarce, and the majority of the series include a limited number of patients.1,3
The effect of aging on esophageal motor function is controversial, and whether the degree of functionality declines with aging or not is not well defined yet.4 In elderly patients with achalasia the residual LES pressure decreases with age;4,5 other studies reported increase on the LES basal pressure but without differences on the residual LES pressure or on the amplitude of the non-peristaltic contractions.6
¿Objective
To describe the clinical presentation and esophageal manometry results in patients with idiopathic achalasia and compared the results between those≤60 years of age and those older.
¿ Methods
We performed a retrospective analysis of all the clinical records from the Gastrointestinal Motility Laboratory at Specialties Hospital, Centro Médico Nacional Siglo XXI, Mexico City, from January 2000 to December 2007. Patients in whom achalasia was initially diagnosed by clinical and manometric criteria were included. Patients with vigorous achalasia (an arbitrarily defined disorder), secondary causes of achalasia (Chagas disease, cancer), or history of previous treatment (surgical myotomy or pneumatic dilation), were excluded. The patients with idiopathic achalasia were divided in two groups: 1) Classic achalasia and 2) achalasia with complete relaxation of EEI. Two groups were established: 1). ≤60 years, and 2). >60 years of age.
Clinical evaluation: At the time of manometric evaluation, all patients were asked to score the severity of dysphagia, regurgitation, heartburn, chest pain, and cough using a 5-point scale ranging from: 0 , no symptom; 1, present ≤1 time/ month; 2, present ≤1 time /week; 3, present ≤3 times a week; 4, present 33 times a week; and 5, with each meal. Time from first symptom or eventual weight loss to diagnosis was also recorded.
Esophageal manometry: Patients were studied after on overnight fasting. The catheter was placed through the nose/mouth. Four-lumen water-perfused (0.5 mL/min) polyvinyl catheters with an outside diameter of 3.5 mm and 50 mm-intervals were used (Zinetics Manometric Catheter, Medtronic A/S, Tonsbakken 16-18, DK-2740 Skovunde, Denmark). The catheters were connected to a low-compliance pneumohydraulic capillary infusion pump system (Microcapillary, Infusion System for esophageal manometry, J.S. Biomedicals, Inc. California). Each lumen was connected to an external transducer (Medexinc Lab Inc., Mx), and the recordings were traced on a PC polygraph HR S/N 712 1616 (Synectics Medical AB, Stockholm, Sweden). Pressures were recorded with a computerized motility system and analyzed by means of specialized software (Polygram Version 5.06C2, Upper GI edition, Gastrosoft Inc). The manometric protocol consisted on the station pull-through technique (SPT).7 Basal LES pressure was calculated as the mean of the differences of the peak LES pressures over the intragastric pressure for each recording port (normal basal LES pressure, 10 mmHg - 25 mmHg). LES relaxation was considered complete when the LES pressure decreased to the gastric baseline pressure, absent when it did not change and incomplete when it decreased but failed to reach the baseline value. Residual LES pressure was considered as the lowest pressure over the gastric baseline occurring within 5 seconds following the onset of a swallow (5 mL water) after measuring three swallows (normal <8 mmHg). Esophageal body function was assessed by giving 10 wet swallows of 5 mL of water at 30s intervals. The velocity and amplitude of the contractions were analyzed with four transducers, 5 cm apart from each other, and located 3 cm, 8 cm, 13 cm and 18 cm above the LES. Manometric parameters were evaluated and classified according to the 2001 Guidelines for the Classification of Esophageal Motility Disorders.8,9 All studies were reviewed by a single experienced gastroenterologist (MG). Achalasia was defined manometrically by: 1). Aperistalsis of the esophageal body, and 2). Abnormal LES relaxation. Aperistalsis was defined as either no motor response in the esophageal body after swallowing or by simultaneous low-amplitude esophageal contractions (10 mmHg - 40 mmHg). Abnormal LES relaxation was defined as an absent or incomplete relaxation with wet swallows (residual pressure >8 mmHg) or complete, but brief relaxation (<6 s) to the gastric baseline. Hypertensive LES (>45 mmHg) was not required for the diagnosis of achalasia.7-11 Classic achalasia is defined by incomplete LES relaxation and aperistalsis of the esophagus.
Statistical analysis: Results are expressed as proportions, medians (intervals) and means (± standard deviation). Results from patients older than 60 years were compared to those of patients being 60 years old or younger. Manometric parameters were compared between the two groups using non-paired t-test and duration of symptoms using median test. In addition gender and symptoms were compared between the two groups using the Z-test. Spearman's correlation coefficients were obtained to detect possible relationships among discrete variables; a p value <0.05 was considered as significant. Statistical analysis was performed by means of the SPSS statistical software for Windows (SPSS 12.0, Chicago, IL, USA).
¿ Results
One hundred and ninety patients with achalasia were assessed: 106 (55.8%) were female and 84 (44.2%) male. Thirty-one patients were excluded: 23 because of having been submitted to Heller's myotomy, two because of previous pneumatic dilation, five because of vigorous achalasia and one because of Chagas disease.
A total of 159 patients were therefore enrolled, including 112 patients who suffered from classic achalasia and 47 patients who suffered from achalasia with complete LES relaxation, but brief (<6 s). The overall mean age was 46.43 ± 16.51 years. Clinical variables: The clinical characteristics are described and compared by age groups on Table 1. Chest pain was more frequent in patients≤60 years than in those >60 years (51.2 vs. 22.2%, p <0.003). This difference was maintained when comparing only the group of men ≤60 years vs. men >60 years (51.9 vs. 9.52%, p <0.002).
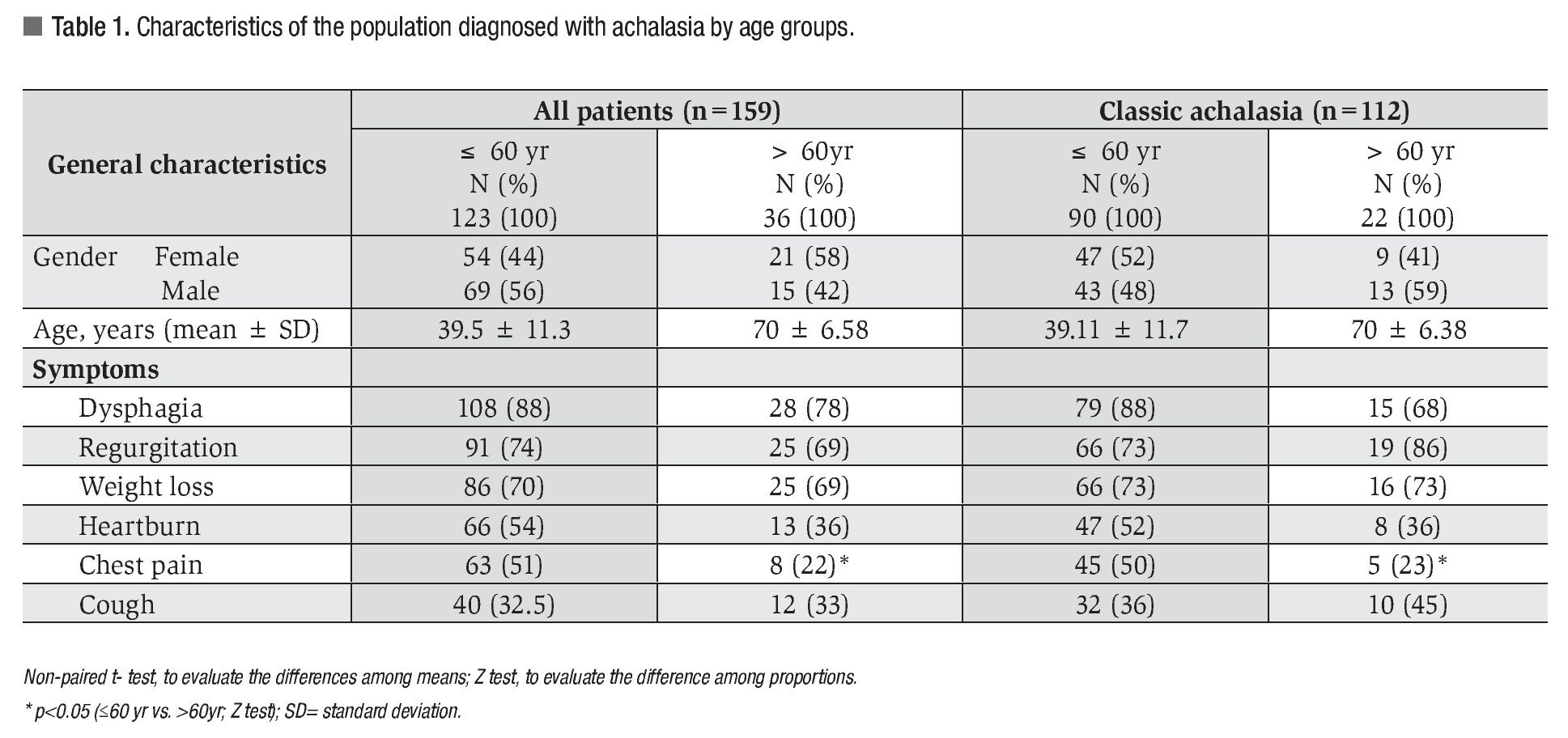
The clinical characteristics of the patients with classic achalasia (Table 1) were similar to the ones observed in the overall group; chest pain was more frequent (50 vs. 23%, p <0.03), and the duration of symptoms in months was greater in patients ≤60 years than in those >60 years, 24 months (range 1 - 228) vs. 12 months (range 3 - 480) (p <0.05, respectively).
Manometric variables: The manometric parameters are shown on Table 2. The mean basal LES pressure was similar in both groups. The LES was hypertensive (>45 mmHg) in 21 subjects: 17 patients ≤60 years and 4 patients >60 years (13.8 vs. 11%, p >0.8). The LES relaxation was incomplete (residual pressure >8 mmHg) in 70.4% of the cases; however, its frequency was similar in both groups (73.1% for ≤60 years and 61.1% for >60 years, p = 0.23). The amplitude of the simultaneous esophageal contractions on the esophagus body was also similar in both groups. An inverse correlation between age and residual LES pressure was found (r = -0.164, p <0.05).
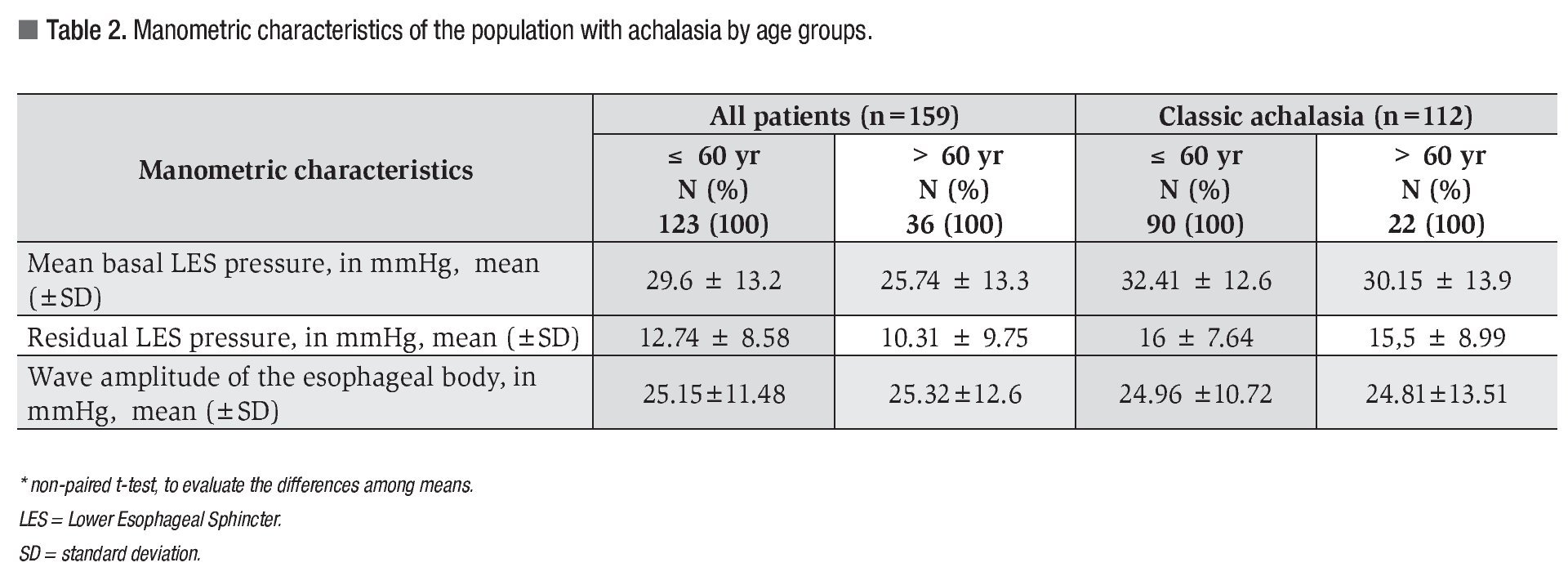
The manometric characteristics of patients with classic achalasia were similar for both groups (Table 2); however, when comparing classic achalasia vs. achalasia with complete relaxation, the mean basal LES pressure was greater in the group of classic achalasia (31.9 ± 12.8 vs. 20.9 ± 11.1, p <0.001) (Figure 1).
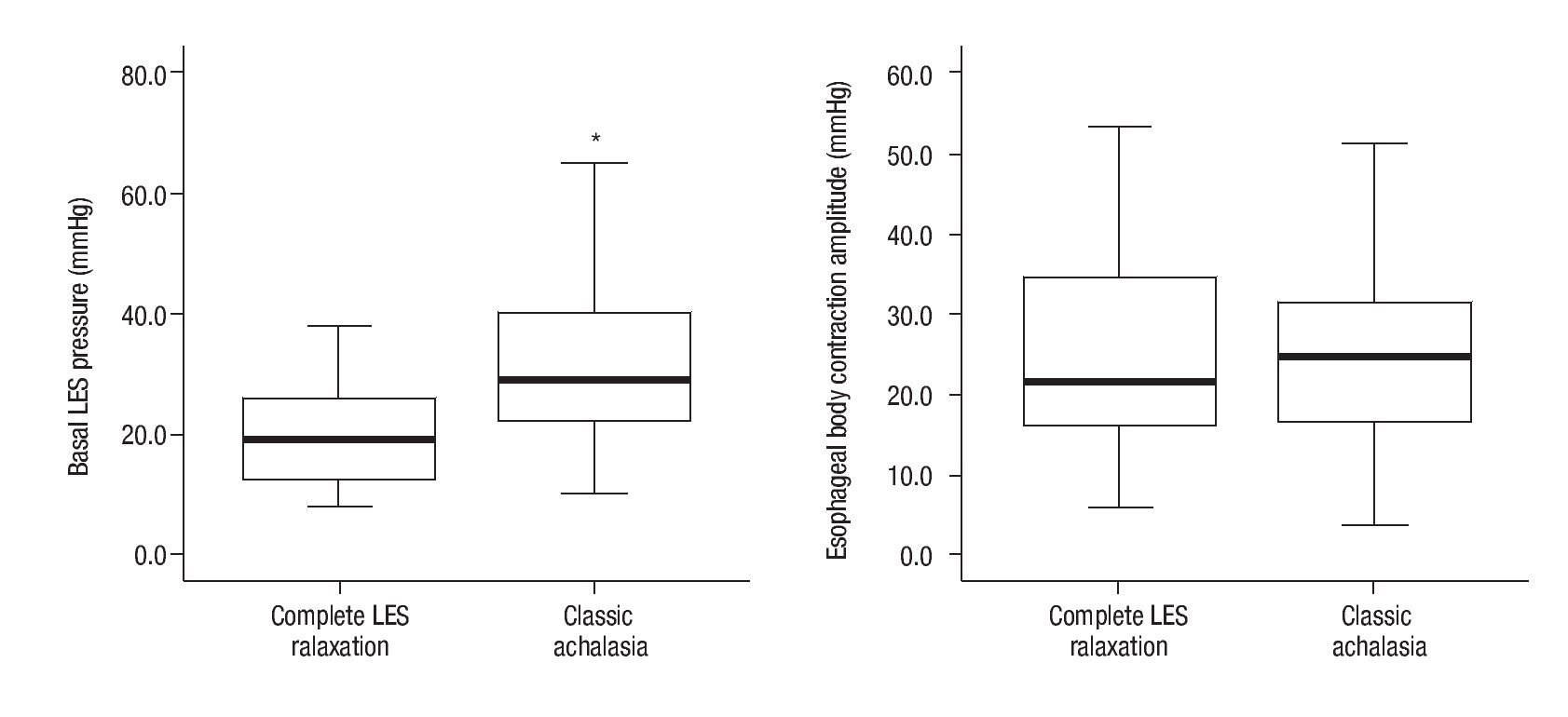
¿ Figure 1. Boxplot depicting the extreme mean basal lower esophageal sphincter (LES) pressure values and the mean wave amplitude of the esophageal body in millimeters of mercury (mmHg) in patients with classic achalasia and achalasia with complete LES relaxation. The horizontal line represents the mean value and the vertical line indicates the distribution tendency. The basal LES pressure in the classic achalasia group was 31.97 mmHg ± 12.85 mmHg, and in the achalasia with complete relaxation group was 20.99 mmHg ± 11.12 mmHg. This difference was statistically significant (p <0.05). The mean wave amplitude of the esophageal body was 24.93 mmHg ± 11.26 mmHg vs. 25.79 mmHg ± 12.85 mmHg, respectively (p = 0.67).
¿ Discussion
We found a significantly higher frequency of chest pain in patients younger than 60 years and also an inverse correlation between age and residual LES pressure.
Because aging and achalasia are both associated with degenerative changes in the myenteric plexus,3,12 it is reasonable to expect that aging may modify the manometric presentation and, possibly, the disease clinical presentation. Esophageal motility disorders are considered a dynamic and progressive disease spectrum. It has been suggested that the esophageal body aperistalsis with complete LES relaxation represents an early stage of the disease, eventually progressing to classic achalasia (esophageal body aperistalsis and incomplete LES relaxation).8,10,13 In contrast, Mearin and Malagelada14 consider that complete LES relaxation is not necessarily an early manifestation of classic achalasia. Others might argue that the method of detecting LES relaxation was suboptimal. Richter described that 70% - 80% of patients have incomplete or null relaxation, and that the other 20% - 30% have complete relaxation (residual pressure <8 mmHg), although of short duration and functionally inadequate.9 In this series, we included 159 patients with both clinical and manometry findings of achalasia, and found that 71% of the patients fulfilled the diagnostic criteria for classic achalasia, in agreement with what it has been reported in other series elsewhere.3,8,9
The initial presentation of the disease has been described to typically occur in people between the third and fifth decades of life, and that one third of cases present after 60 years of age;15 however, authors as Ribeiro and Clouse have described a lower frequency in the elderly population (14% and 8%, respectively).4,5 In contrast, Hashem and collaborators found that, in a series of 117 patients with achalasia, 42% of the subjects were older than 65 years.6 Recently, Birgisson and Richter reported an epidemiological study performed in Iceland where demographic and clinical features in 62 patients with classic achalasia were assessed; 38.7% of the cases were adults older than 60 years.16 In this series, 22.6% of the cases were adults above 60 years of age.
Clouse et al. reported that the clinical presentation of achalasia is affected by age, with chest pain being less severe and less common in older adults. In this series we found that chest pain is more frequent in ≤60 year and that men are less affected than women in older that 60 years, a finding which was previously described by d´Alteroche et al.17 The mechanism of chest pain is unknown, occurs in some patients, primarily at night, and is especially seen in patients with milder disease when the esophagus is minimally dilated.3 We also observed that the duration of symptoms in older than 60 years was shorter compared to that of the adults younger than 60 years; this difference is also seen in the group of patients with classic achalasia suggesting that age may affect the early diagnosis.
Upon evaluation of the manometric characteristics of patients with achalasia, we found an inverse correlation between age and LES residual pressure, a finding which has also been described in healthy subjects, besides the correlation between age, the residual LES pressure and the amplitude of the esophageal contractions.18 Nevertheless, upon comparing the means of the residual pressures we found no significant differences such as those reported by Clouse et al, and Ribeiro et al.4,5
In this group of classic achalasia, the only manometric difference with respect to patients with complete LES relaxation was a greater basal LES pressure (31.97 vs. 20.99 mmHg, p <0.001), a finding which was previously described by Hashemi et al, who, in turn, suggested that the increase in the basal LES pressure in elderly patients may represent the chronicity of the disease.6
Esophageal manometry is considered the gold standard diagnostic test for achalasia. The recent introduction of high resolution manometry has greatly helped in making the diagnosis of achalasia. It allows a more careful evaluation of LES and esophagogastric junction relaxation using the integrated relaxation pressure, and is divided into 3 subtypes based on the function of the esophageal body with the idea that different subtypes may respond to treatment in a variable fashion.19
We believe this retrospective study has several limitations: A). the follow-up of the cases, including the evaluation of treatment response, was not possible; B). a possible selection bias: being our institution a referral center, our patients may not be representative of the general population; and C). all achalasia patients were diagnosed with conventional manometry.
¿ Conclusion
Our results indicate that in Mexican patients with achalasia the chest pain is more frequent in men younger than 60 years, and residual LES pressure decreases with age.
Correspondence author: Nayeli Ortiz Olvera, MD,
MSc. Cuauhtémoc 330, México City, México, CP. 06725.
Telephone: (+52) 5556276900, ext: 21566 - 21317 - 21318.
E-mail: nayelixoortiz@yahoo.com.mx
Received March 2th, 2011;
accepted June 30th, 2011.

