






¿ Introduction
Heartburn is one of the main symptoms of gastroesophageal reflux disease. This disease is considered to be a public health problem throughout the Western world.1 Around 10% of the adult population of the United States reports suffering from heartburn on a daily basis2 and in Brazil heartburn presents weekly prevalence in 11.9% of the population.3
Within this high general prevalence certain factors present a close relationship with greater severity of gastroesophageal reflux. Among these are age,4 obesity,4,5 increased intra-abdominal pressure6 and cigarette smoking.1,5 However the mechanism that triggers heartburn, regardless of whether gastroesophageal reflux is present or not, is so far only partially understood.7
With regard to epidemiological studies one of the factors that should always be brought in mind is the subjects' socioeconomic condition. This has importance as a risk factor8 in relation to the diagnosis,9,10 treatment,11 prevention and even morbidity-mortality of the disease.12
Low socioeconomic level is associated with a large range of diseases.13 However, although the correlation between individuals socioeconomic condition and their overall health is well established in Western countries,13-15 few studies have evaluated socioeconomic factors in relation to gastroesophageal reflux disease10,16 and even fewer in relation to heartburn. Furthermore there is a lack of epidemiological studies focusing on private gastroenterological clinics. Socioeconomic condition is not routinely evaluated in private gastroenterological clinics. This is perhaps because of short time to carry out complete evaluations or because the patients maybe don't understand or accept the importance of such data. Patients often report imprecise data simply because they do not wish to feel diminished or depreciated in front of the physician, or because they cannot see the importance that this information might have for achieving correct diagnosis and treatment for the disease.
Because of the high prevalence of heartburn, its direct correlation with gastroesophageal reflux disease and the poor understanding of this symptom, we decided to conduct this study in order to correlate heartburn occurrences among patients with different socioeconomic conditions.
¿ Methods
We conducted a prospective study over a consecutive 18-month period among 1184 patients living in three cities on the coast of the State of São Paulo, Brazil (Santos, São Vicente and Guarujá) who sought assistance at a private gastroenterological clinic. These subjects answered a previously established questionnaire.
Patients living in one of these three cities who were aged 18 years or over were eligible for inclusion in the study. Pregnant or breastfeeding women, individuals who had undergone surgery on the esophagus and/or gastrointestinal tract (except appendectomy) and individuals who refused to participate in the study were excluded.
The questionnaire was applied by a single examiner and was made simple and with objective questions to avoid confounding issues.
Heartburn was defined as a sensation of retrosternal burning that radiates from the manubrium of the sternum to the base of the neck and into the throat.17
With the aim of standardizing the procedure for the questionnaire and to avoid biased responses, we chose to apply the questionnaire to the third patient and the last patient on each consultation day. If the third patient did not fulfill the inclusion or exclusion criteria, the next patient was evaluated. If the last patient of the day could not be evaluated, we chose the first patient of the subsequent day.
The clinical questionnaire was divided in four parts. In the first part, personal identification data were sought (name, present address, number of children, marital status and date of birth). In the second, the subjects were asked how often they had felt heartburn or pyrosis over the preceding month and whether such symptoms had interfered with their daily activities and to what extent. In the third, the characteristics of the food consumed in the household were evaluated, along with the educational level of the family member who cooked and the family income. In the fourth and last part, the sanitation conditions of the patient's home were evaluated.
During the medical consultation, we measured the body mass index (BMI), defined as the weight in kilograms divided by the square of the height in meters (weight/height2). We used the World Health Organization classification, such that individuals with BMI of up to 18.5 kg/m2 were considered underweight; 18.6 kg/m2 to 25.0 kg/m2, normal weight; 25.1 kg/m2 to 30.0 kg/m2, overweight; 30.1 kg/m2 to 40.0 kg/m2, obesity; and greater than 40.0 kg/m2, morbid obesity.
Qualitative variables were represented by absolute frequencies (n) and relative frequencies (%), and quantitative variables by means, standard deviations (SD), medians, minimum and maximum values. The presence of associations between the variable "city" and the other variables was evaluated using the chi-square test. The same test was used to investigate the presence of any association between the most disturbing symptom and patients personal data. Comparisons between the cities were made using the analysis of variance (ANOVA) technique for quantitative variables with normal distribution. Differences were investigated by means of multiple comparison tests. The distinct quantitative variables (number of television, number of radios, etc.) were analyzed using the nonparametric Kruskal-Wallis test for independent samples. Differences were again investigated by means of multiple comparison tests.
Scores were attributed to frequency variables, as follows: never = 0, up to once a month = 1; between two and four times a month = 2; between five and twelve times a month = 3; and between 13 and 30 times a month = 4. The cities were also compared in relation to the frequency scores, using the nonparametric Kruskal-Wallis test.
The significance level was taken to be 0.05 (α = 5%) and descriptive levels (p) lower than this value, were considered significant.
The study was performed in accordance with the declaration of Helsinki, the protocol was thoughtfully explained and informed consent was obtained from all patients.
¿ Results
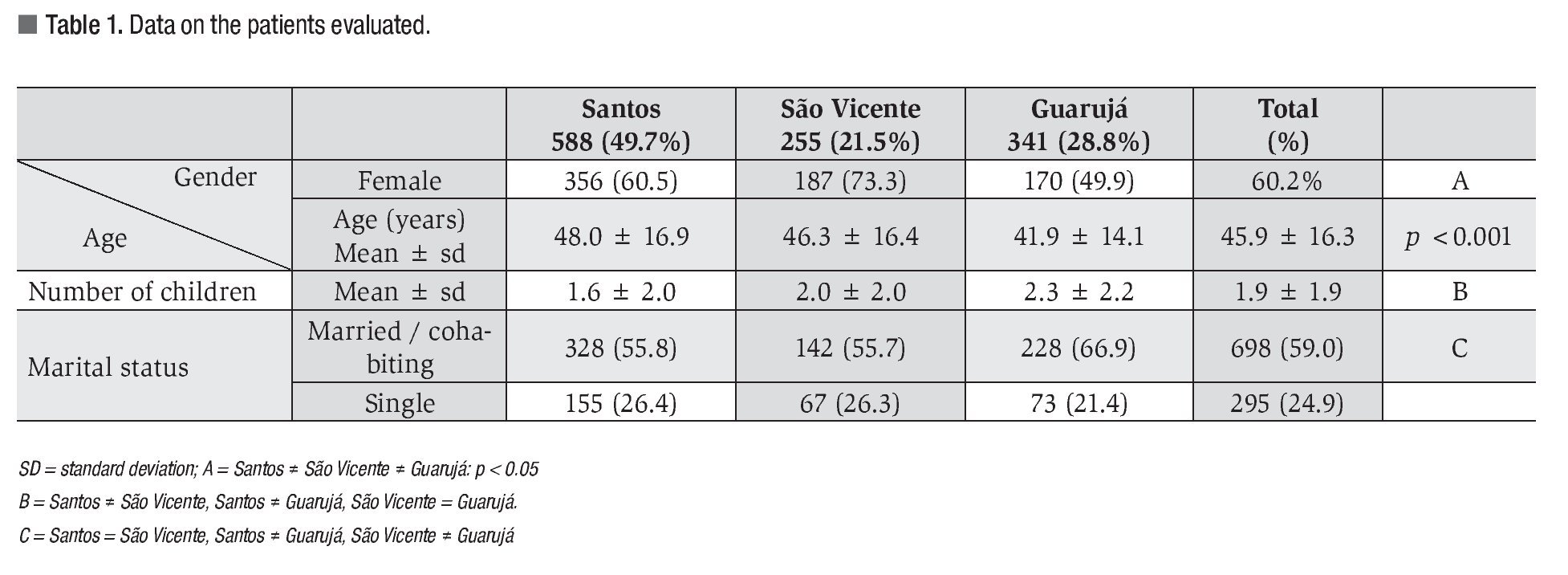
A total of 1184 patients living in the three cities who sought consultations with a gastroenterologist were evaluated. Out of this sample, 588 (49.7%) lived in Santos, 255 (21.5%) in São Vicente and 341 (28.8%) in Guarujá. The majority of patients were women (713; 60.2%). The patients' mean age was 45.9 ± 16.3 years, with an age range from 18 to 96 years. Most of the patients were married or cohabiting (698 individuals; 59.0%), while 295 (24.9%) were single, 115 (9.7%) were widowed and 76 (6.4%) were divorced. The mean number of children that the patients had was 1.9 (SD = 1.9). Data on the patients evaluated are showed in Table 1.
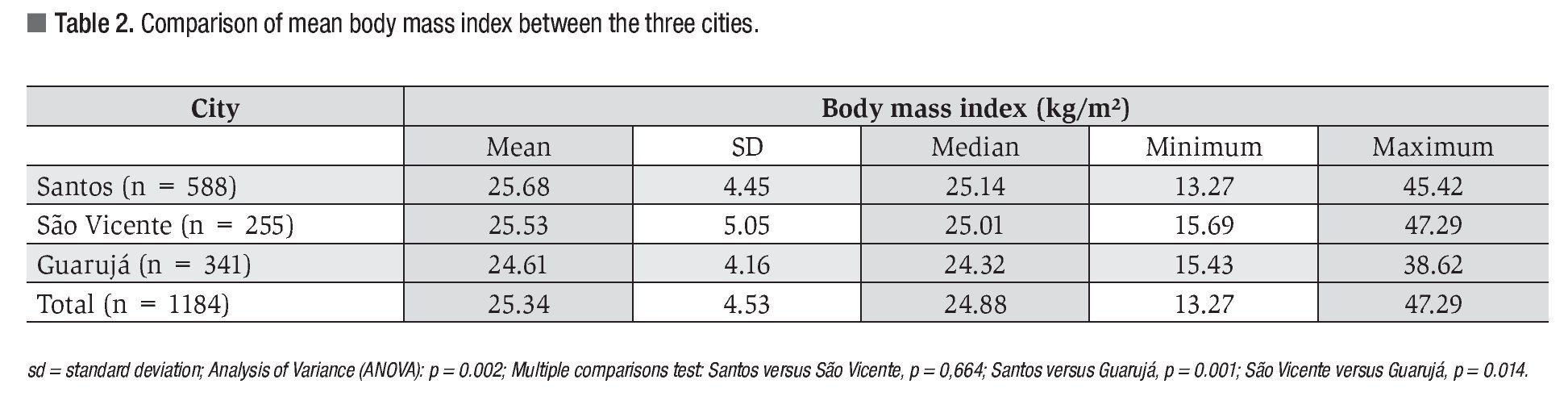
There were statistically significant differences between the cities regarding the mean BMI among the individuals attended (p = 0.002) (Table 2).
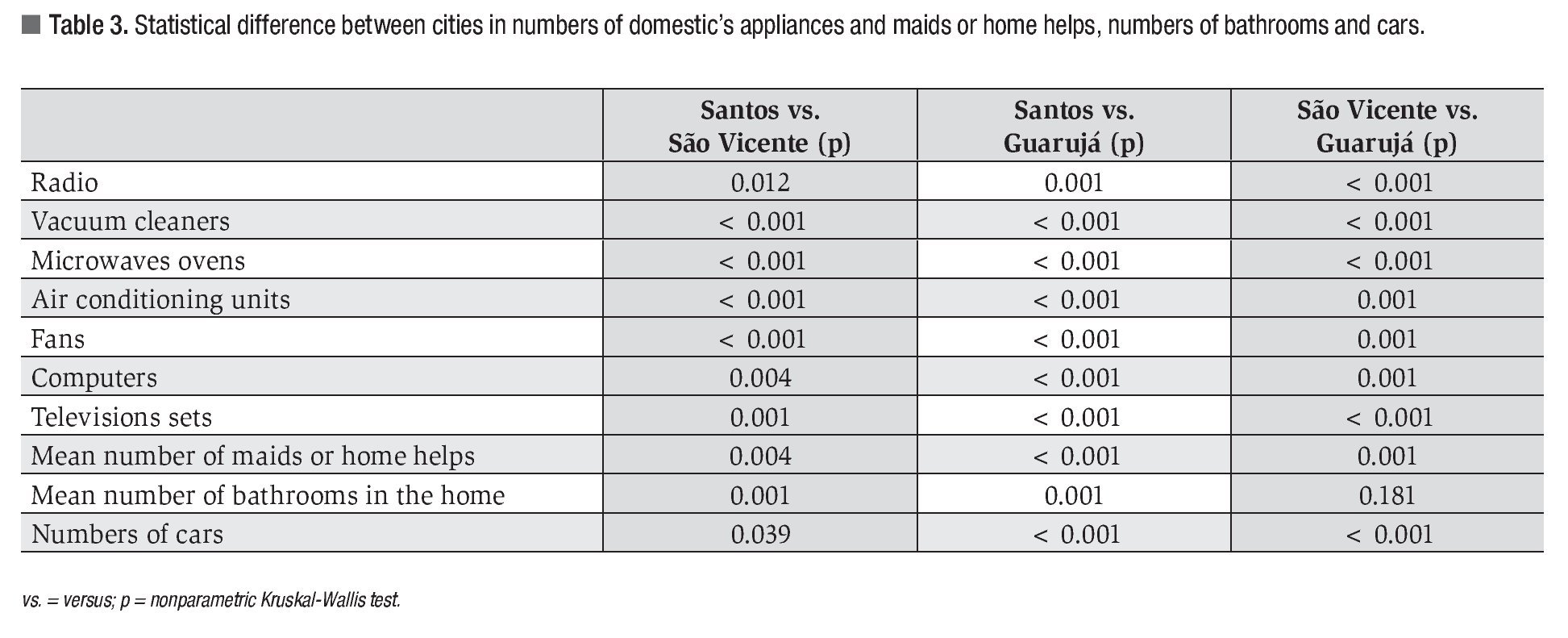
Comparing the three cities in relation to purchasing power, we inferred that the patients from Santos were in a better economic position than those from the other two cities. This was extrapolated in our study from the greater quantities of electrical equipment installed in the homes in Santos (Table 3). These results show that the people living in São Vicente were characterized by better economic conditions than among those living in Guarujá. The other characteristics that were evaluated also showed Santos as the higher economic status city (Table 3).
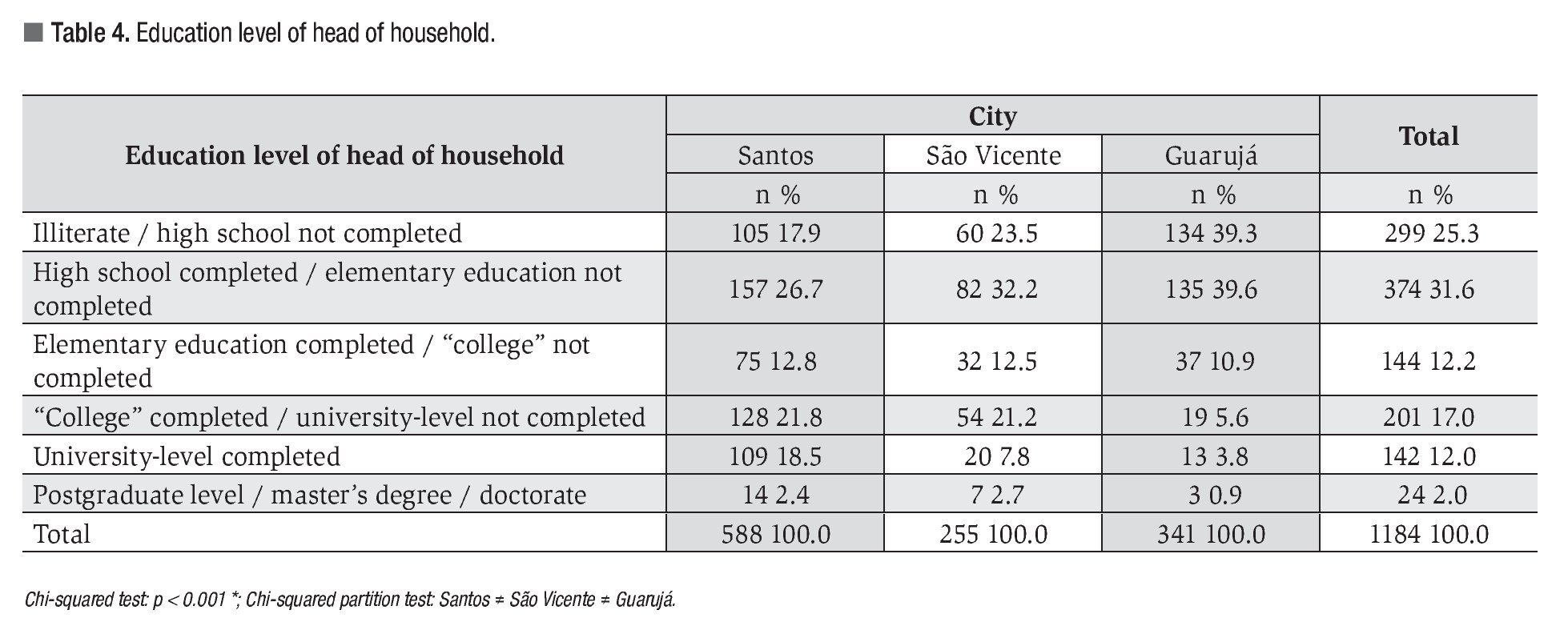
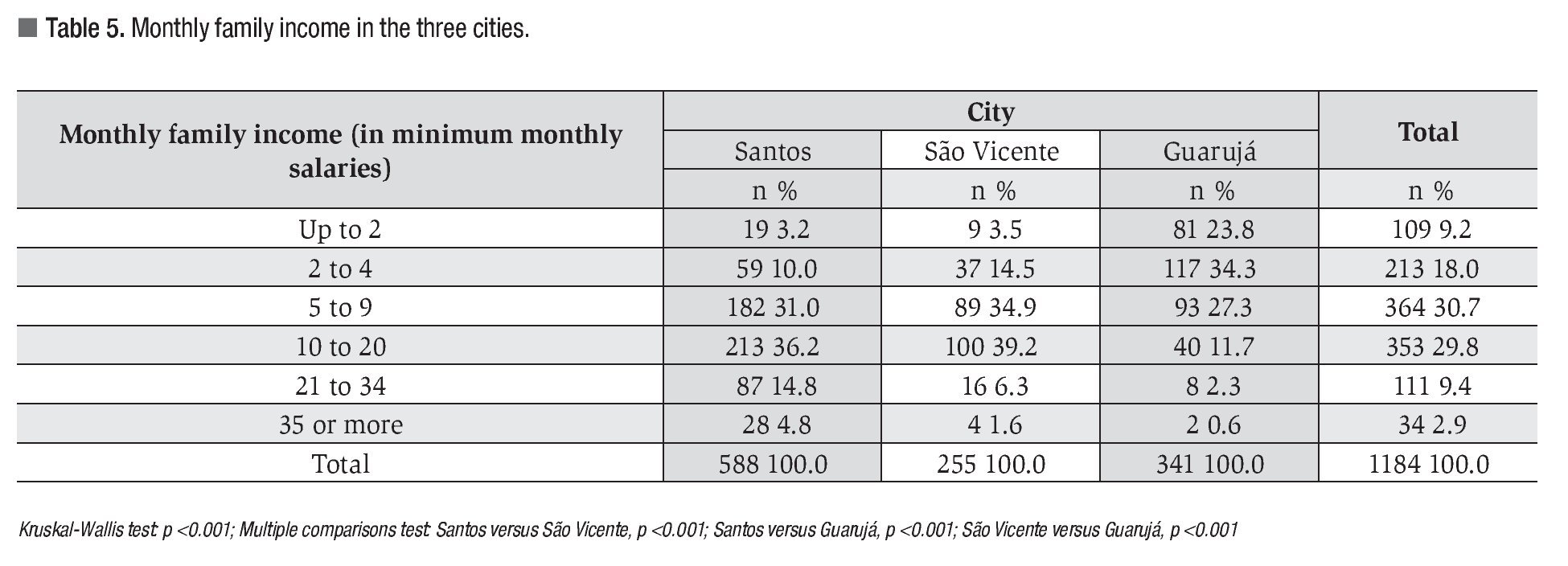
The multiple comparisons test showed that there were statistically significant differences between three cities regarding the education levels of heads of households of the patients attended (p <0.001) (Table 4). Furthermore, monthly family income among the individuals attended also presented statistically significant differences between the three cities (p <0.001), as shown by the multiple comparisons test (Table 5). The greater economic conditions of patients from Santos in relation to São Vicente and Guarujá reflects their greater purchasing power as shown through the significantly greater family income in Santos than in São Vicente, which in turn was greater than the family income among patients from Guarujá.
Other findings also demonstrated that the patients from Guarujá were the ones with the worst living conditions. They presented the highest number of people living in the same home and the homes of the patients from Guarujá had fewer bedrooms.
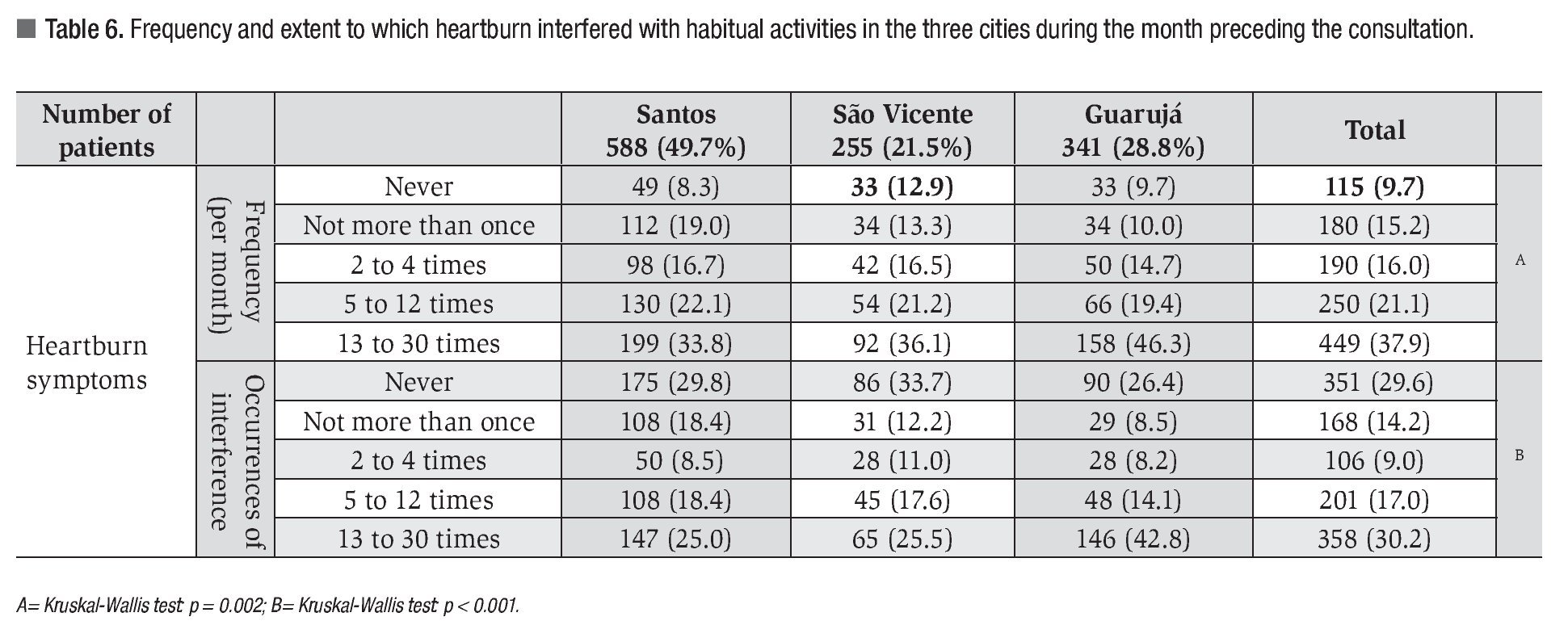
There was a statistically significant difference between the cities regarding the distribution of heartburn frequency during the month preceding the patients consultations (p = 0.002). Symptoms at frequencies of five to 30 occurrences over that month were reported by 65.7% of the patients from Guarujá, 55.9% from Santos and 55.7% from São Vicente. The multiple comparisons test showed that the patients from Guarujá differed significantly from those living in the other two cities. Table 6 shows the distribution of heartburn frequency and the extent to which this symptom interfered with daily activities over the month preceding the consultation, among the 1,184 patients studied. The extent of this interference differed significantly between the cities (p <0.001). Within the range of five to 30 occurrences per month, heart-burn symptoms interfered with the daily activities of 56.9% of the patients from Guarujá, 43.5% from Santos and 23.1% from São Vicente. The multiple comparisons test showed that Guarujá differed significantly from the other two cities (Table 2).
There were no statistically significant associations between heartburn symptoms and gender (p = 0.282), marital status (p = 0.447), age group (p = 0.102) or number of children (p = 0.491), among the patients attended.
¿ Discussion
It has been estimated that gastroesophageal reflux disease is the digestive system disease with the highest direct and indirect costs in the United States.18 Heartburn is the principal symptom of this disease and is present in approximately 89% of the individuals affected by this condition.19
We prospectively evaluated 1184 adult patients from three different coastal cities using preestablished methodology. We considered that the total number of patients evaluated was acceptable, even though studies with larger samples exist. The study by Jones and Lydeard20 evaluated 2066 patients who answered a questionnaire and sent it back to the investigator by mail. On the other hand, in the study by Tougas and collaborators21 1036 patients in several Canadian cities were evaluated in person. In this light, we believe that our sample was of significant size. Moreover, in our study, all the interviews were conducted in person and by the same investigator, thereby avoiding differences in evaluation criteria based on subjective interpretation. According to the international literature, although the interview method is more laborious, it certainly furnishes better quality data than from self-applied questionnaires. Interviews avoid the possibility of bias relating to patients concern not to displease their physician.19
Factors relating to housing conditions provide awareness of how patients live. Although the basic living conditions (electricity, plumbing and sewerage) among our patients were good, the number of people living in these homes was high. This may come to be reflected in problems relating to living together day-by-day or in various psychological disorders.
Comparing purchasing power between the three cities it could be seen that the patients from Santos were in a better situation than those from the other two cities. This inference was extrapolated from the patients' domestic equipment ownership and housing characteristics. Other factors, such as education levels (highest in Santos), also affirm for the economic superiority of Santos in relation to São Vicente and of the latter in relation to Guarujá.
There was no statistically significant difference in heartburn prevalence between the genders in the present study. Likewise, there are studies on gastroesophageal reflux that also did not find greater prevalence for one gender or the other.22,23 We also did not find any statistical differences regarding race/ethnicity, number of children, marital status or age group. However extrapolating from the typical symptoms of gastroesophageal reflux disease there are studies showing greater prevalence among older age groups and among divorced, separated and widowed patients.22
The city of Guarujá presented statistical significance regarding the frequency of heartburn symptoms and their interference with activities during the month preceding the consultation. It has been shown that the impairment of quality of life is directly proportional to the severity of the symptoms.24,19 According to Nocon and collaborators25 the quality of life is worse among individuals with nocturnal heartburn.
We observed that the patients in lower socioeconomic situations presented greater frequency of heartburn that interfered in their daily activities. A study by Nouraie and collaborators26 showed that there was no greater prevalence of gastroesophageal reflux disease in relation to any education level among patients. On the other hand, another study showed an inverse relationship between educational level and the presence of gastroesophageal reflux.16 However, the patients in those studies were evaluated in relation to gastroesophageal reflux disease, rather than the symptom of heartburn. Hence, our finding differed from these other studies, in that the lower the education level was, the greater the prevalence of heartburn symptoms.
We also found in our study that the patients from Guarujá presented statistically significant lower body mass index than that of patients from Santos and São Vicente. It is known that heartburn may be a consequence of acid reflux from the stomach to the esophagus but several other causes that trigger these symptoms have been implicated. Chemical or mechanical stimulation as well as hyperalgesia may cause the symptom.2
Our study made us aware of several factors that might interfere with the approach taken and therapeutic success among patients with heart-burn. We emphasize that heartburn is closely related to the economic situation of the patients. This directly reflects how the patient reacts to heart-burn eventually exacerbating the symptom. It is important to evaluate patients with heartburn beyond the medical history placing importance on the environment within which they live.
It was observed that heartburn in patients without gastroesophageal reflux disease present etiopathogenic factors triggering the symptom that are more complex than those in patients with gastroesophageal disease. Some of these patients may already present non-erosive esophagitis or even functional heartburn a clinical condition compatible with gastroesophageal reflux disease. What may be of greater importance is that these patients may present the symptom before developing gastroesophageal reflux disease. Further studies should be conducted with this aim and in order to achieve greater understanding of heartburn with and without gastroesophageal reflux. Knowledge of the epidemiology and risk factors for heartburn within a region is the first step towards formulating prevention and treatment strategies.
¿ Conclusions
The presence of heartburn was directly related to the low socioeconomic conditions of the city in which the patients lived. The prevalence and severity of heartburn were unrelated to gender, marital status, race/ethnicity, age or number of children. The less favored social class evaluated by a variety of socioeconomic factors presented greater incidence of heartburn than did the more favored social class.
Correspondence author: Tomas Navarro-Rodriguez MD.
Department of Gastroenterology - Clinical Gastroenterology. Av Dr Enéas de Carvalho Aguiar 255. 9th floor - room 9159. São Paulo, Brazil. ZIP 05403-000.
Telephone: 5511-3069 7830, fax: 5511 3069 7830.
E-mail: tnavarro@usp.br.
Received March 25th, 2011;
accepted April 15th, 2011.

