
Introduction
The prevalence of inflammatory bowel disease (IBD) in Mexico is unknown. However, on the bases of studies carried-out in hospitalized patients, it has been suggested that it is low.1 On the other hand, the occurrence of familial cases has been ascribed to genetic influences (HLA-DR1 is associated with genetic susceptibility to IBD in the Mexican mestizo population [p= 0.003, OR= 3.9]),2 environmental factors, or a combination of both. So far the rarity of IBD in married couples has been considered against the importance of environmental factors.3,4 In the north of Europe and United States varies from four to eight cases per 100,000 people/year.5-7 It has been reported several cases of IBD in married couples.8,9
Case report
The patient, a 26-year-old woman, she was born in Mexico City without family history of IBD. She was referred to the hospital with a five months history of diarrhea with blood and blood watery stools. A colonoscopy and biopsy (Figure 1) confirmed ulcerative colitis (UC). Her symptoms were controlled after treatment. At the time of the diagnosis her marital status was single and she got married two years later. Currently she is under medical treatment for UC and she did not develop any complications related with UC. Her husband a 29 years old man born in Mexico City as well as his parents, but their grand parents came to Mexico from Spain. He was well for three years after he get married when he presented abdominal symptoms and the diagnosis of duodenal ulcer, tubulovillous colonic polyps, hepatic steatosis and hypercholesterolemia were made. One year later he developed diarrhea with blood. A colonoscopy and biopsy confirmed UC and no polyps (Figure 2) At the present time he is under treatment for UC and also for gastroesophageal reflux disease. He did not develop any complications related with UC.
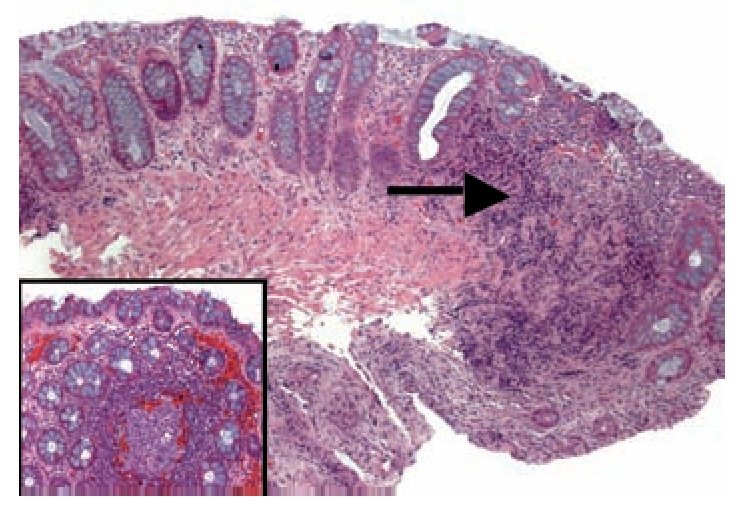
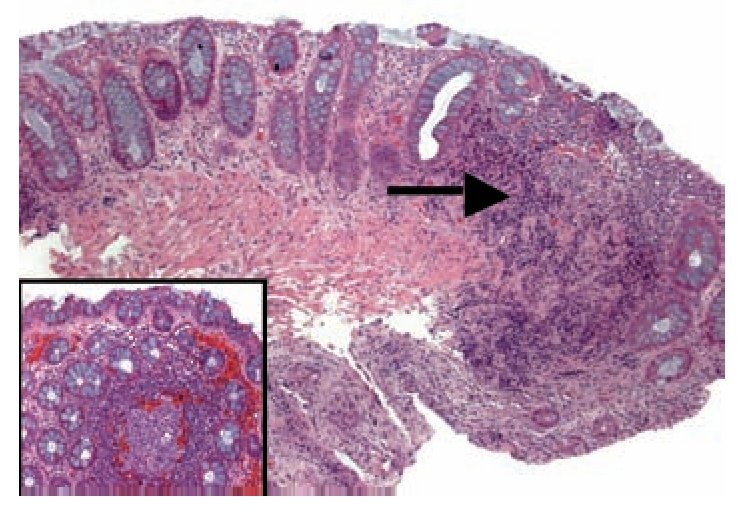
Figure 1. Biopsy of rectum has altered architectural pattern and lymphoplasmocitary infiltration (arrow). In other areas are nodular lymphoid hyperplasias with germinal center (inset), diminution of mucous production and Paneth cells metaplasia (arrow head)
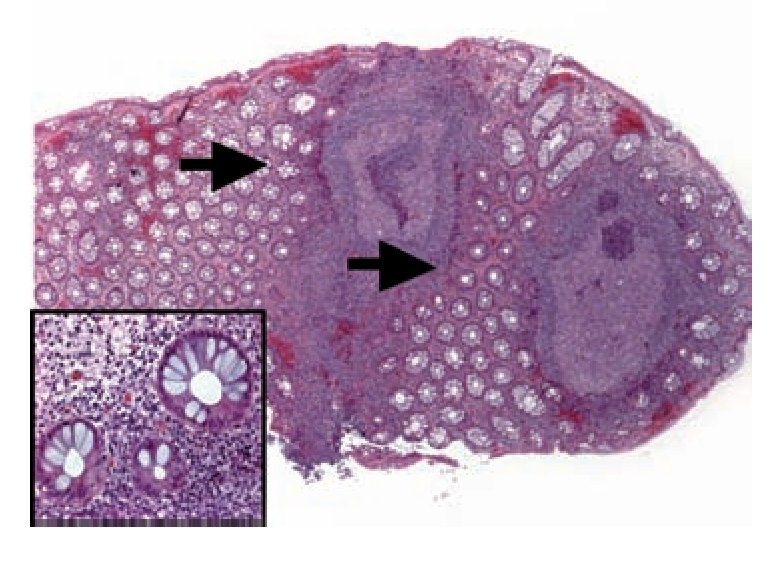
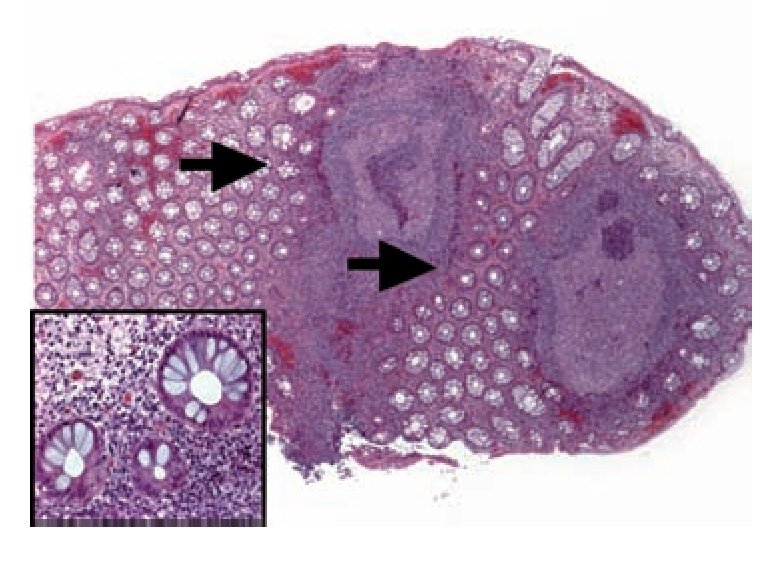
Figure 2. In the biopsy of rectum are lymphoplasmocitary infiltrations diffuse and nodular with germinal centers (arrows) with distortion architectural pattern. In the crypts are diminutions in the mucous production (inset)
DiscussionEpidemiological studies of IBD in Northern France and Belgium have shown a higher incidence of Crohn's disease (CD) than UC and the presence of many familial clusterings, some of which are extraordinary.10 In 1994 Comes et al.9 reported 10 instances conjugal IBD in Europe and the same group of researches reported the results of study carried-out in the same area. They registered thirty conjugal instances. Seventeen were concordant for CD and 3 for UC. In addition they found that most couples got the disease after cohabitation. According with their results they suggested and etiologic role for environmental factors.
The present case is the first Mexican report of a couple with IBD. According with characteristics of this case, we can speculate that the environmental and infectious etiology might play some role in the development of IBD.
Whether this factor is related to the increased intestinal permeability observed in spouses of patients with CD is unknown. Firstly, as we mention above the prevalence of IBD in Mexico is low. Secondly, husband and wife were not consanguineous and both of them are mestizo. Thirdly, they have not family history of IBD and, fourth they were not smokers.
The clinical spectrum of IBD in this couple shown that the spouse presented the disease before cohabitation. The time period among the experienced first symptoms and the diagnosis between spouse and husband was four years. In the study by Söderholm et al.,11 all spouses with an increased baseline permeability had lived with their CD partner for more than 10 years; suggesting barrier dysfunction as an early event in mucosal inflammation.
Some studies have shown an increase in intestinal permeability in response to acetylsalicylic acid in 30%-40% of CD relatives, suggesting a hereditary disturbance of the mucosal defense system. Acetylsalicylic acid has been found to increase tight juction permeability via an effect on mitochondrial oxidative phosphorylation.12,13
They were concordant for UC compared with other series where CD was the most frequent diagnosis.4,8,9
Finally, it has been suggested that infectious gastroenteritis (IGE) is responsible to the development of several secondary or chronic health conditions, such as IBD. In fact, Porter et al.14 in an elegant study found that IGE increased the risk of IBD (odds ratio, 1.40; 95% confidence interval, 1.19 -1.66). The risk was slightly higher for Crohn's disease compared with ulcerative colitis.
Considering the present data of this Mexican couple with IBD, we can conclude that IBD is heterogeneous disorder of mutifactorial etiology in which hereditary (genetic) and environmental (microbial, behaviour) factors interact to produce the disease. However, more studies are necessary to understand the relation between microflora and the immune system in healthy and UC patients.
Correspondence author: Nahum Méndez-Sánchez, M.D.,PhD.
Departments of Biomedical Research and Gastroenterology. Medica Sur Clinic & Foundation, Puente de Piedra 150, Col. Toriello Guerra, Tlalpan, 14050 Mexico City, Mexico. Phone: (+525) 55606-6222 ext. 4215; Fax: (+525) 55666-4031;
E-mail:nmendez@medicasur.org.mx
Received: January 17th, 2008 Accepted on: June 25th, 2009

