



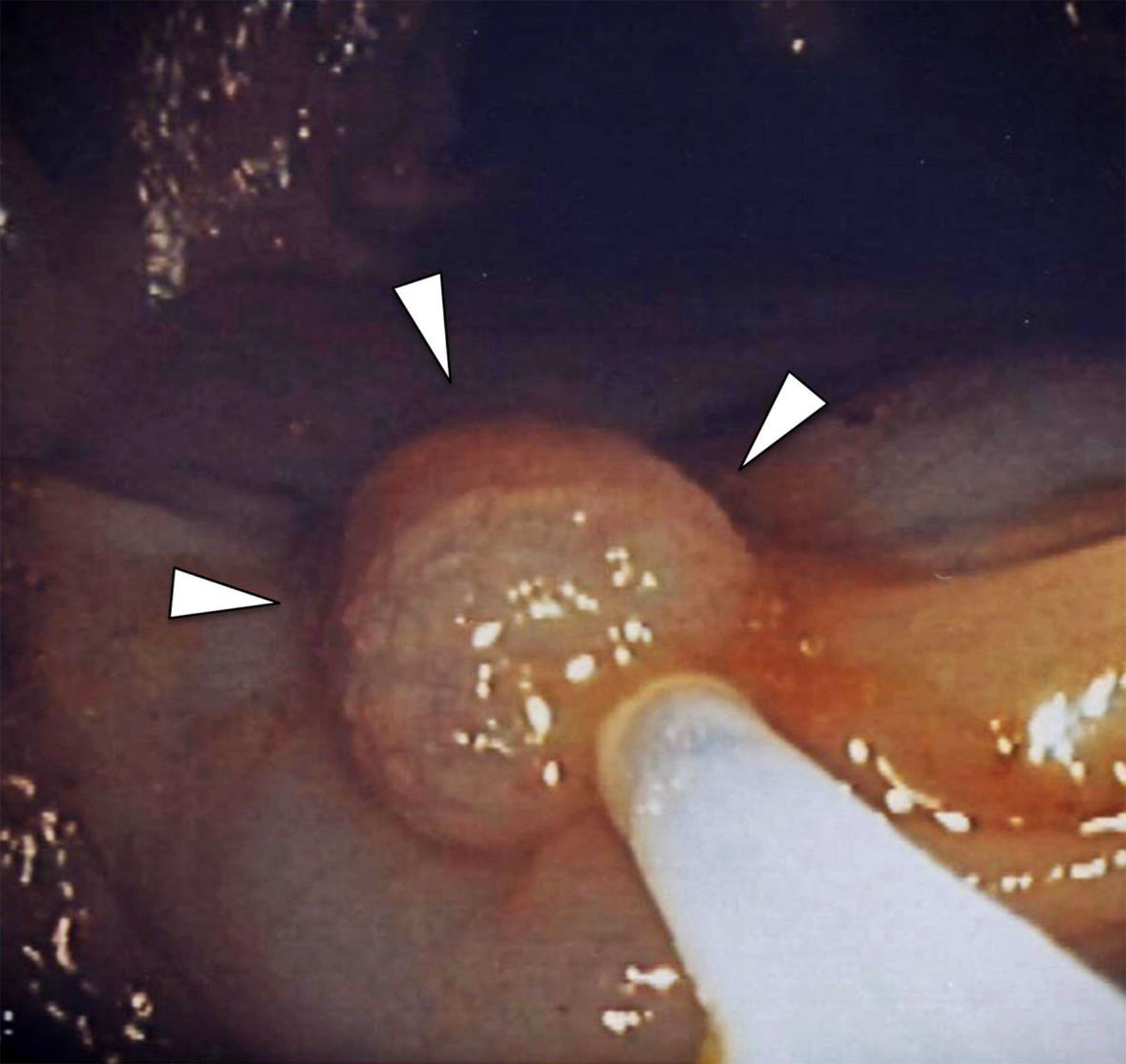
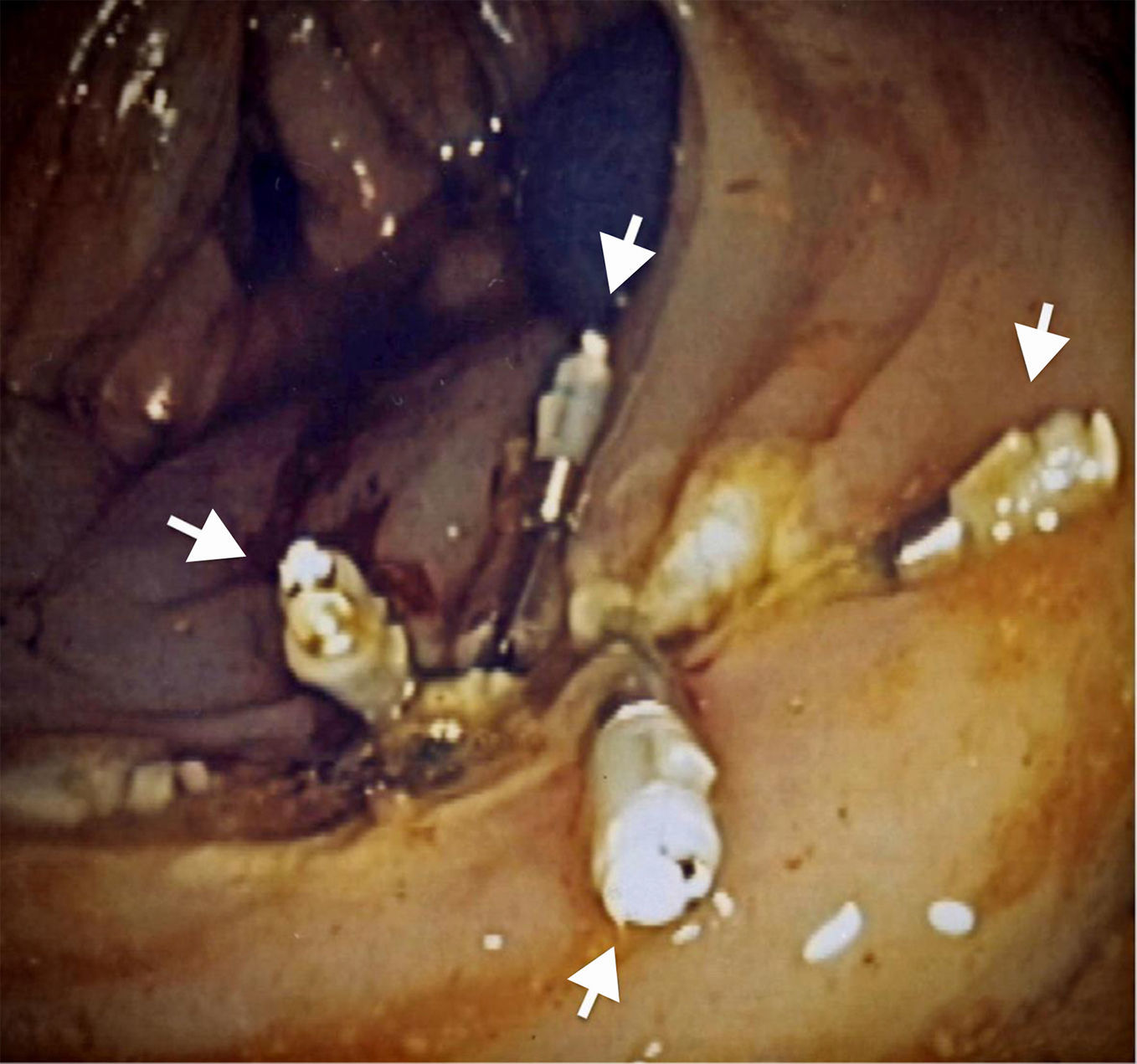
A 70-year-old man underwent endoscopy that revealed an adenomatous polyp in the ascending colon (fig. 1). It was removed in the same session through the placement of four endoscopic clips (fig. 2). Six hours after the endoscopic polypectomy, the patient presented with severe intermittent lower intestinal bleeding with an initial hemodynamically unstable status: heart rate > 80 bpm and systolic blood pressure <100mmHg. After multidisciplinary agreement, the patient underwent urgent selective digital subtraction angiography of the superior mesenteric artery that showed the presence of active bleeding in the ascending colon in the area of the previous endoscopic polypectomy (fig. 3A). Super-selective transarterial embolization of the active bleeding was performed with success (fig. 3 B and C). Lower intestinal bleeding disappeared and the patient was hemodynamically stable immediately after the transarterial embolization. The patient did not need a bowel resection.
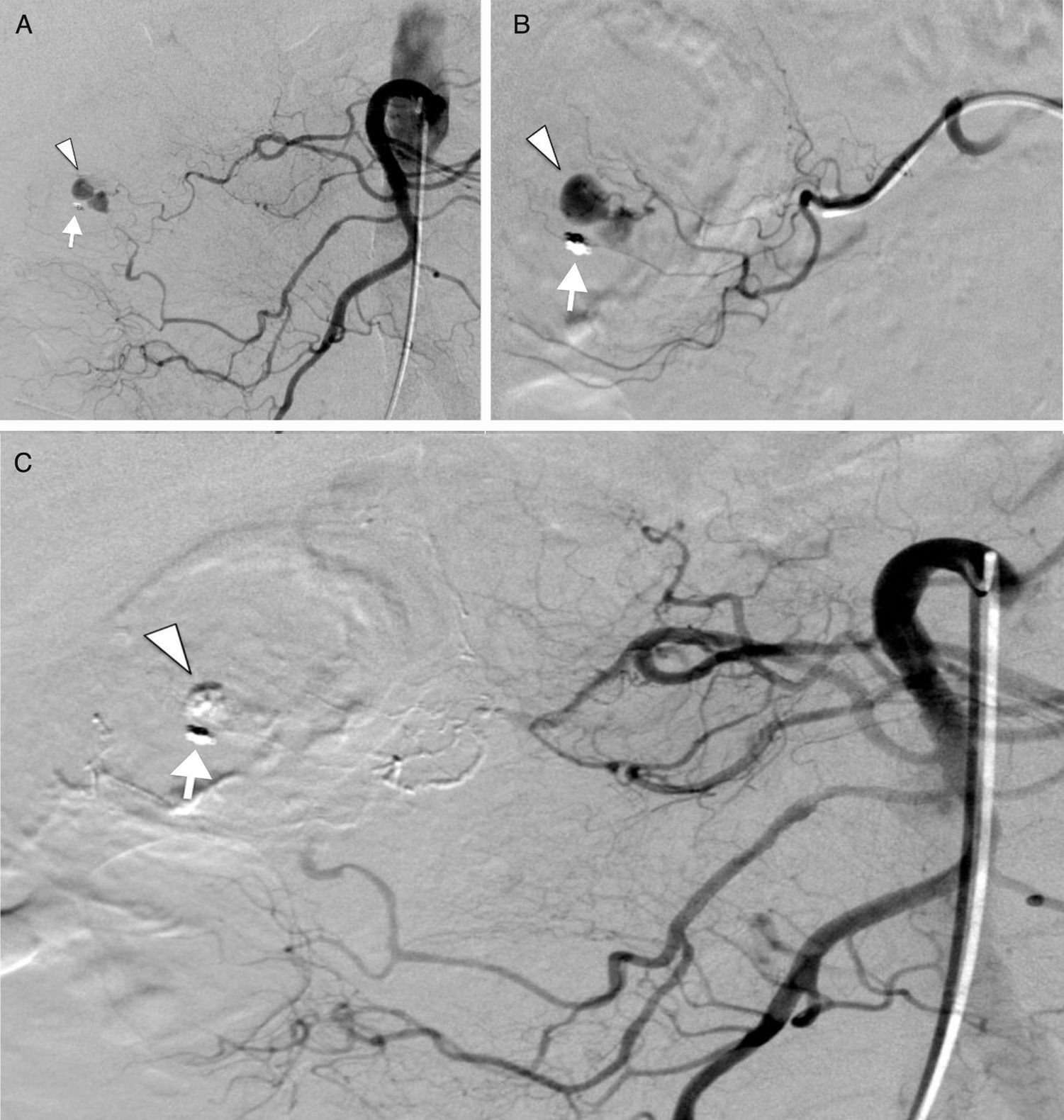
A) Selective digital subtraction angiography of the superior mesenteric artery that shows the presence of contrast extravasation (arrowhead) from the vasa recta of a distal arcade of the right colic artery, next to the only remaining endoscopic clip (arrow). B) Super-selective catheterization of the distal arcades of the right colic artery with contrast extravasation from the vasa recta (arrowhead) near the endoscopic clip (arrow). C) Final selective digital subtraction angiography of the superior mesenteric artery that shows the complete exclusion of the vasa recta of a distal arcade of the right colic artery embolized by n-butyl cyanoacrylate with the absence of contrast extravasation (arrowhead) near the endoscopic clip (arrow).
Lower intestinal bleeding after endoscopic polypectomy can be seen up to 2 weeks after the procedure. However, acute post-polypectomy bleeding is due to: insufficient hemostasis of the vessels, or sloughing of the surface coagulum1. Despite advances in medical management, acute lower intestinal bleeding after endoscopic polypectomy remains a major complication with high morbidity and mortality. Interventional endoscopy and angiography are the fastest and least invasive therapies for controlling this major complication2,3. Nevertheless, endovascular embolization is the preferred therapy when there is massive hemorrhage or in clinically unstable patients3.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Rossi UG, Rubis-Passoni G, Torcia P, Cariati M. Hemorragia intestinal aguda después de polipectomía endoscópica: embolización superselectiva en un paciente clínicamente inestable. Revista de Gastroenterología de México. 2017;82:341–343.

