
Anastomotic leaks present in 8.3 to 5.9% of patients after esophagectomy and gastrectomy, respectively.1 Saliva and gastric juice leakage into the mediastinum is responsible for 30-40% of postoperative deaths.1 The use of self-expanding metal stents has been reported to aid in cicatrization and reduce mortality.2 The aim of this report was to present our experience in 7 cases of postoperative leakage after esophagogastric oncologic surgery treated through fully covered self-expanding metal stents (FCSEMSs).
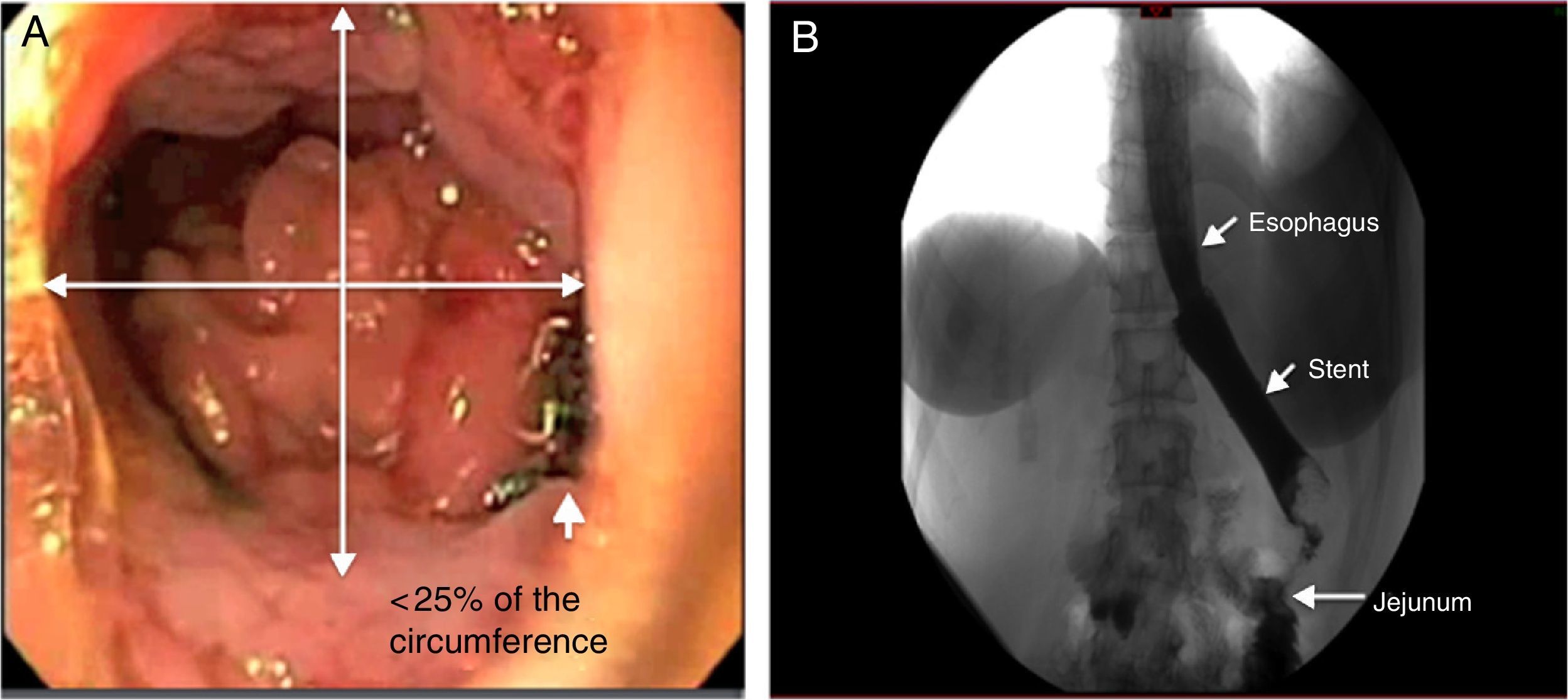
Between January 2013 and October 2014, 7 patients with postoperative leakage were treated (Table 1). Four were men and 3 were women and their ages ranged from 30 to 64 years. The etiologic diagnosis was cancer of the gastroesophageal junction in 2 patients, gastric adenocarcinoma in 4, and esophageal adenocarcinoma in one patient. All the patients were candidates for surgical resection. Esophagojejunal anastomosis was the surgical reconstruction performed in 5 patients and esophagogastric anastomosis was performed in 2. During the endoscopic check-up, the approximate anastomotic defect percentage was calculated as follows: ¼ of the circumference = 25%, ½ = 50%, and ¾ =75%. The endoscopic study revealed defects at the level of the anastomosis of < 25 to 70% of the circumference (Fig. 1). The time lapse between the surgery and diagnosis of the leak was from 4 to 20 days and it varied from 5 to 40 days between the surgery and stent placement. A FCSEMS (SX-ELLA Stent Esophageal HV, Czech Republic) with an 85mm length and distal, mid, and proximal diameters of 25, 20, and 24mm, respectively, was placed in all the cases under sedation and fluoroscopic control (Fig. 1). It was a silicone-covered nitinol stent. Six of the 7 patients had immediate occlusion of the leak after contrast medium instillation under fluoroscopic control (Fig. 1). Leakage output stopped within 24h after stent placement in 6 patients and was confirmed clinically and through a barium swallow (Fig. 1). Oral diet was begun 1-3 days after stent placement in 5 patients, one patient received parenteral nutrition due to a swallowing disorder secondary to a cerebral hemorrhage, and one patient had surgical reintervention without beginning the oral diet. The FCSEMSs were removed using conventional biopsy forceps, putting pressure on the stent loop. The stents were easily removed with no complications 27-40 days after placement in 6 patients. Endoscopic check-up and barium swallow showed no evidence of leakage after stent removal. There was one case of partial stent displacement, but it continued to cover the leakage site. Granulation tissue was found in the same patient at the distal end of the stent. The stent covering was undamaged at the time of extraction in 6 of the 7 patients. We had no stent-related complications or deaths.
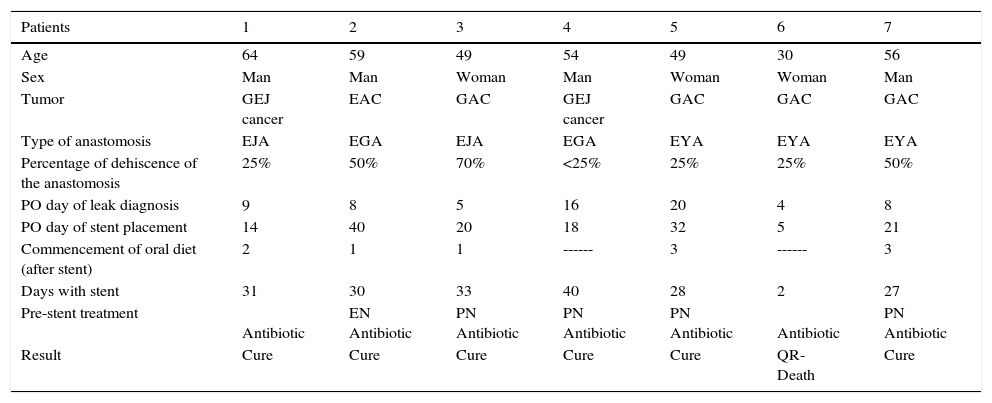
Patient characteristics and results.
| Patients | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Age | 64 | 59 | 49 | 54 | 49 | 30 | 56 |
| Sex | Man | Man | Woman | Man | Woman | Woman | Man |
| Tumor | GEJ cancer | EAC | GAC | GEJ cancer | GAC | GAC | GAC |
| Type of anastomosis | EJA | EGA | EJA | EGA | EYA | EYA | EYA |
| Percentage of dehiscence of the anastomosis | 25% | 50% | 70% | <25% | 25% | 25% | 50% |
| PO day of leak diagnosis | 9 | 8 | 5 | 16 | 20 | 4 | 8 |
| PO day of stent placement | 14 | 40 | 20 | 18 | 32 | 5 | 21 |
| Commencement of oral diet (after stent) | 2 | 1 | 1 | ------ | 3 | ------ | 3 |
| Days with stent | 31 | 30 | 33 | 40 | 28 | 2 | 27 |
| Pre-stent treatment | Antibiotic | EN Antibiotic | PN Antibiotic | PN Antibiotic | PN Antibiotic | Antibiotic | PN Antibiotic |
| Result | Cure | Cure | Cure | Cure | Cure | QR-Death | Cure |
EAC: esophageal adenocarcinoma; EGA: esophagogastric anastomosis; EJA: esophagojejunal anastomosis; EN: enteral nutrition; GAC: gastric adenocarcinoma; GEJ: gastroesophageal junction; PN: parenteral nutrition; PO: postoperative; QR: surgical reintervention
 The endoscopic image shows the leakage site. B) The x-ray shows the esophageal stent with no contrast agent leakage.")
Important considerations in the treatments of leaks include their etiology, size, and the clinical condition of the patient. Different studies have shown the feasibility of placing self-expanding metal stents in patients with anastomotic leakage that would otherwise require a surgical intervention.2–4 In our cases, clinical success reached 85.7%, coinciding with other studies that have reported success rates of 48-100%, with no difference between the result and the type of stent used.5–9 Studies in animals suggest that stent placement for 30 days is sufficient for tissue cicatrization.10 In our patients, the stents were in place for 27-40 days, a length of time similar to that of a previous study.10 With respect to the precise time for stent placement, some authors favor placement within 24h of leak diagnosis to limit contamination of the cavity and promote cicatrization.1,10 However, there have also been reports stating that late placement can result in closure of the anastomotic leak.1,6 In our short experience, the stents were removed 5 to 32 days after surgery and cicatrization was achieved in 6 of the 7 patients. One report suggests that to be successful, the leaks should be smaller than 70% of the circumference of the anastomosis and there should be no ischemia.1 Our findings were similar, except in one patient with 25% dehiscence of the anastomosis. In that case the leak became larger after stent placement, which was documented through tomography, and the patient underwent surgical reintervention.
FCSEMS placement appears to be a feasible and less invasive option in patients with postoperative leaks after esophagogastric oncologic surgery. We used a stent with a larger distal diameter and a proximal ring designed to prevent migration. Such characteristics can be useful in patients with postoperative leaks. It is important to consider surgical reintervention when there are unsatisfactory results.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Alonso-Lárraga JO, de la Mora Levy JG, Hernández Guerrero A, Rodarte-Shade M, Ramírez-Solís ME. Prótesis metálicas totalmente cubiertas para el tratamiento de las fugas después de cirugía oncológica esófago-gástrica. Revista de Gastroenterología de México. 2017;82:100–102.

