


The prevalence of gastroesophageal reflux disease (GERD) has been reported to be increasing in recent years. However, there have been few reports on the prevalence of GERD during pregnancy in the Asian population. The aim of our study was to evaluate the prevalence and characteristics of GERD in Vietnamese pregnant women.
Materials and methodsThis cross-sectional study was conducted at the antenatal clinic of the Nhan Dan Gia Dinh Hospital, Ho Chi Minh, Vietnam. Four hundred females, at various stages of pregnancy, were enrolled. GERD was diagnosed if there was troublesome heartburn and/or acid regurgitation, at least once a week, during the current pregnancy.
ResultsThe overall prevalence of GERD in pregnancy was 38.5% (154/400). The prevalence of GERD in the third trimester was significantly higher than that in the second trimester (46.8% vs. 30.7%, P=0.008) and tended to be higher than its prevalence in the first trimester (46.8% vs. 35.4%, P=0.051). In the pregnant women with GERD, the frequency of regurgitation was significantly higher than that of heartburn (92.9% vs. 30.5%, P<0.001). Those typical symptoms were more prevalent in the daytime, compared with nighttime.
ConclusionOur study showed that GERD was prevalent during pregnancy in Vietnam. In the pregnant women with GERD, regurgitation was much more common than heartburn, and those typical reflux symptoms occurred more frequently in the daytime, compared with nighttime.
La prevalencia de la enfermedad por reflujo gastroesofágico (ERGE) ha aumentado en los últimos años. Sin embargo, hay pocos informes sobre el predominio de esta afección durante el embarazo en la población asiática. Nuestro objetivo fue evaluar la prevalencia y las características de la ERGE entre las mujeres embarazadas vietnamitas.
Material y métodosEste estudio transversal se llevó a cabo en el Hospital Nhan Dan Gia Din, en Vietnam. Se incluyó a 400 mujeres embarazadas en distintas fases del embarazo. La manera de diagnosticar la ERGE fue la observación de presencia de pirosis molesta o regurgitación ácida al menos una vez a la semana durante el embarazo.
ResultadosLa prevalencia de ERGE en el embarazo fue del 38,5% (154/400). Esa prevalencia en el tercer trimestre fue mayor que en el segundo trimestre (46,8 frente a 30,7%; p=0,008) y tendió a ser mayor que en el primer trimestre (46,8 frente a 35,4%; p=0,051). La frecuencia de regurgitación fue mayor que la de pirosis (92,9 vs. 30,5%; p<0,001). Estos síntomas típicos se manifestaron con mayor frecuencia durante el día que durante la noche.
ConclusionesNuestro estudio demostró que la ERGE era prevalente en el embarazo en Vietnam. Entre las mujeres embarazadas con ERGE, la regurgitación era mucho más común que la pirosis y estos síntomas típicos de reflujo ocurrían con más frecuencia durante el día que durante la noche.
Gastroesophageal reflux disease (GERD) is one of the most common gastrointestinal disorders in pregnant women, with a prevalence of 45-80%1. GERD may manifest for the first time during pregnancy, but it can also be exacerbated by pregnancy. The multifactorial pathophysiology of GERD in pregnancy involves both hormonal and mechanical factors. The decrease in lower esophageal sphincter pressure resulting from a progressive increase in circulating estrogen and progesterone during pregnancy is suggested to be the predominant factor2. Typical manifestations of GERD during pregnancy, such as heartburn and regurgitation, are reported to be comparable to those in the general population3. Although GERD is less prevalent in Asian countries than in Western countries, recent studies have revealed an upward trend in the prevalence of GERD, particularly in the Asian population4. However, there has been little evidence regarding the prevalence and characteristics of GERD during pregnancy in Asia. The aim of our study was to evaluate the prevalence and characteristics of GERD in Vietnamese pregnant women.
Materials and methodsA cross-sectional study was conducted during the period of January to June 2019. We enrolled women at various stages of pregnancy, aged 18 years or older, that visited the antenatal clinic of the Nhan Dan Gia Dinh Hospital, Ho Chi Minh City, Vietnam. The recruitment method was convenience sampling. The antenatal clinic receives approximately 100 visits per day. At the beginning of each workday, the investigators randomly selected 10 numbers from a box containing 100 numbers from 1 to 100. The pregnant women with the corresponding appointment numbers were invited to participate in the study. Recruitment activity was carried out only on the workdays when the investigators were available at the clinic, which did not include all weekdays. The subjects with a history of GERD and those on GERD therapy were also included. We excluded the pregnant women that could not fully answer the study questions due to having a mental disorder.
The questionnaire covered sociodemographic characteristics (age, place of residence, occupation, educational level, pre-pregnancy body mass index, and increase in body mass index during gestation), pregnancy-related factors (gestational age, previous parity), GERD-related details (major and minor symptoms of GERD, frequency of those symptoms, aggravating factors, and relieving factors). The Gastroesophageal Reflux Disease Questionnaire (GERD-Q) was also used to collect data related to GERD symptoms5. A history of smoking and alcohol use, dietary habits, and a history of GERD, in previous pregnancies or before the current gestation, were also recorded. In the present study, the diagnostic criteria for GERD in pregnancy were the presence of troublesome heartburn and/or acid regurgitation, at least once a week, during the current gestation. Our evaluation of the risk factors of GERD and reflux-related insomnia in pregnancy has been published, utilizing some of the data collected in the present study6.
Statistical analysisAll data were analyzed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA) software. The qualitative variables were expressed as frequency. The quantitative data with normal distribution were presented as mean (standard deviation), whereas those with non-normal distribution were presented as median (range). The categorical data were expressed as percentages with a 95% confidence interval (CI) and compared using the Pearson chi-square test or Fisher’s exact test, as appropriate. The continuous variables with normal distribution were compared using the Student’s t test, whereas those with non-normal distribution were compared using the Mann-Whitney U test and the Kruskal-Wallis test. A p value<0.05 was considered statistically significant.
Ethical considerationsThe present study was conducted following the current regulations for bioethics research. The Board of Ethics in Biomedical Research of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam, approved this study (ethical code number 513/DHYD-HDDD, signed on December 28, 2018). Written statements of informed consent were obtained from all participants. The anonymity of participants has been completely preserved and encrypted to maintain confidentiality.
ResultsFour hundred pregnant women participated in the study, all of whom met the eligibility criteria of the study.
Prevalence of GERD in pregnancy and patient sociodemographic characteristics
A total of 154 (38.5%) subjects fulfilled the diagnostic criteria for GERD. When categorizing the pregnant participants into 3 trimesters, based on gestational age, the prevalence of GERD in the first, second, and third trimesters was 35.4, 30.7, and 46.8%, respectively. In pairwise group comparisons, prevalence of GERD in the third trimester was significantly higher (p=0.008) than that in the second trimester and tended to be higher (p=0.051) than prevalence in the first trimester. However, the difference in prevalence of GERD between the first trimester and the second trimester was not statistically significant (p=0.438) (Fig. 1).

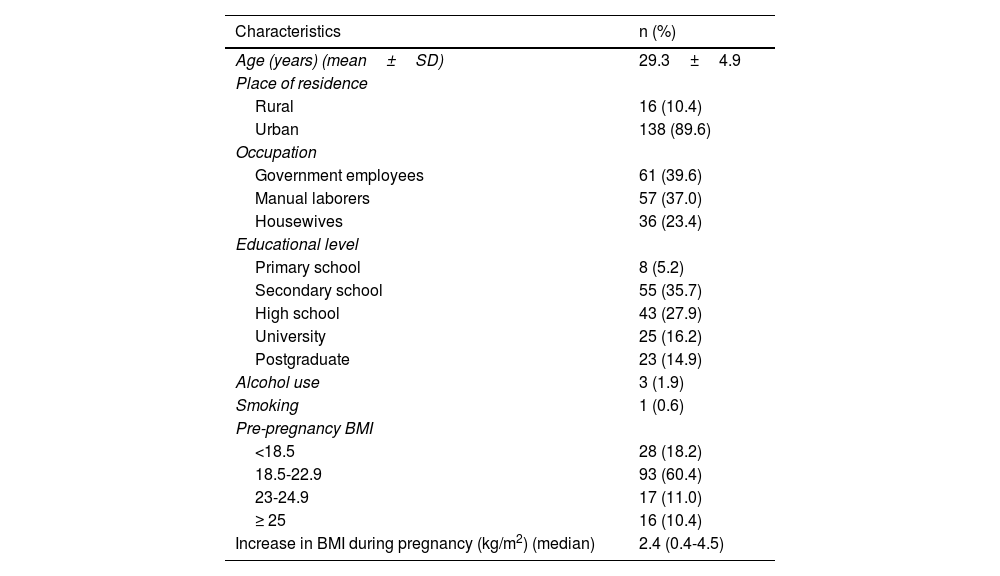
Table 1 summarizes the sociodemographic characteristics of 154 pregnant women with a diagnosis of GERD.
Demographic characteristics of 154 pregnant women with GERD.
| Characteristics | n (%) |
|---|---|
| Age (years) (mean±SD) | 29.3±4.9 |
| Place of residence | |
| Rural | 16 (10.4) |
| Urban | 138 (89.6) |
| Occupation | |
| Government employees | 61 (39.6) |
| Manual laborers | 57 (37.0) |
| Housewives | 36 (23.4) |
| Educational level | |
| Primary school | 8 (5.2) |
| Secondary school | 55 (35.7) |
| High school | 43 (27.9) |
| University | 25 (16.2) |
| Postgraduate | 23 (14.9) |
| Alcohol use | 3 (1.9) |
| Smoking | 1 (0.6) |
| Pre-pregnancy BMI | |
| <18.5 | 28 (18.2) |
| 18.5-22.9 | 93 (60.4) |
| 23-24.9 | 17 (11.0) |
| ≥ 25 | 16 (10.4) |
| Increase in BMI during pregnancy (kg/m2) (median) | 2.4 (0.4-4.5) |
BMI: body mass index; SD: standard deviation.
Of the 154 pregnant women with the diagnosis of GERD, 62 (40.3%) were primigravida, 92 (59.7%) were multigravida, and 84 (54.5%) had already given birth. The median gestation age was 26.0 weeks (range 6.0-39.4). Only 31 (20.1%) of the pregnant women had a history of GERD diagnosis. Up to 78 (50.6%) experienced regurgitation before their current pregnancy or during previous pregnancies. A history of heartburn was less common, reported by 23 (14.9%) of the pregnant women with GERD.
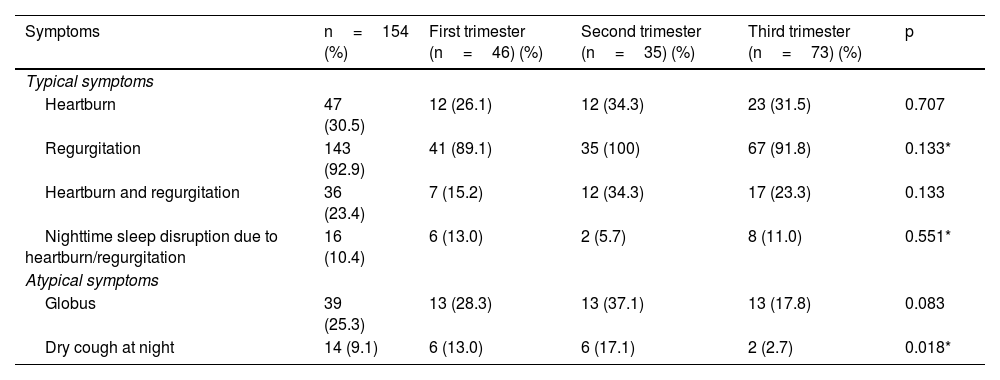
Reflux symptomsThe distribution of typical and atypical symptoms of GERD in each trimester is summarized in Table 2.
The distribution of typical and atypical symptoms of GERD in each trimester.
| Symptoms | n=154 (%) | First trimester (n=46) (%) | Second trimester (n=35) (%) | Third trimester (n=73) (%) | p |
|---|---|---|---|---|---|
| Typical symptoms | |||||
| Heartburn | 47 (30.5) | 12 (26.1) | 12 (34.3) | 23 (31.5) | 0.707 |
| Regurgitation | 143 (92.9) | 41 (89.1) | 35 (100) | 67 (91.8) | 0.133* |
| Heartburn and regurgitation | 36 (23.4) | 7 (15.2) | 12 (34.3) | 17 (23.3) | 0.133 |
| Nighttime sleep disruption due to heartburn/regurgitation | 16 (10.4) | 6 (13.0) | 2 (5.7) | 8 (11.0) | 0.551* |
| Atypical symptoms | |||||
| Globus | 39 (25.3) | 13 (28.3) | 13 (37.1) | 13 (17.8) | 0.083 |
| Dry cough at night | 14 (9.1) | 6 (13.0) | 6 (17.1) | 2 (2.7) | 0.018* |
Considering the typical symptoms of GERD in the pregnant women with a diagnosis of GERD, the frequency of regurgitation was 3 times higher than that of heartburn (92.9 vs. 30.5%, p<0.001). Only 36 (23.4%) presented with both heartburn and regurgitation. Among the subjects with heartburn, 20 (42.6%) had the symptom at night, whereas up to 42 (89.4%) reported having heartburn in the daytime. In the group of pregnant women with GERD that reported symptoms of regurgitation, up to 129 (90.2%) developed regurgitation in the daytime, whereas only 40 (28.0%) had nocturnal regurgitation.
Regarding atypical symptoms, globus sensation was reported in 25.3% of the pregnant women with GERD, whereas dry cough at night (9.1%) was uncommon. The frequency of dry cough at night differed significantly between the 3 trimesters (p=0.018). Compared with the third trimester, the pregnant women with GERD presented with dry cough at night more frequently in the first trimester (13.0 vs. 2.7%, OR 7.7, 95% CI: 1.8-31.9, p=0.005). The proportion in the second trimester was also significantly higher than that in the third trimester (17.1 vs. 2.7%, OR 7.4, 95% CI: 1.4-38.5, p=0.014).
A total of 153 (99.4%) of the 154 pregnant women diagnosed with GERD reported that their reflux symptoms were aggravated by several factors, including stress and the consumption of fatty, spicy, or sour foods.
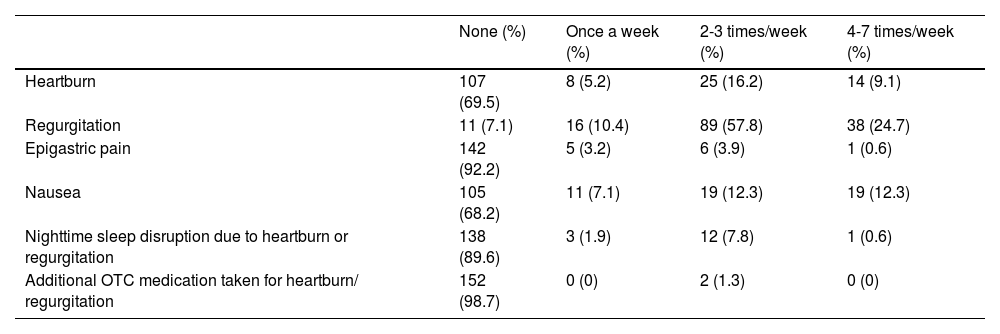
GERD-Q scores and frequency of symptomsTable 3 describes the frequency of reflux symptoms indicated by the results of the GERD-Q. The median GERD-Q score of the pregnant women with GERD was 8.0 (4-16). Said score was significantly higher in the second trimester (8.0, 5-12) and in the third trimester (8.0, 5-16), compared with the first trimester (7.0, 4-14) (p=0.002 and p<0.001, respectively) (Fig. 2).
Frequency of reflux symptoms indicated by the GERD-Q results.
| None (%) | Once a week (%) | 2-3 times/week (%) | 4-7 times/week (%) | |
|---|---|---|---|---|
| Heartburn | 107 (69.5) | 8 (5.2) | 25 (16.2) | 14 (9.1) |
| Regurgitation | 11 (7.1) | 16 (10.4) | 89 (57.8) | 38 (24.7) |
| Epigastric pain | 142 (92.2) | 5 (3.2) | 6 (3.9) | 1 (0.6) |
| Nausea | 105 (68.2) | 11 (7.1) | 19 (12.3) | 19 (12.3) |
| Nighttime sleep disruption due to heartburn or regurgitation | 138 (89.6) | 3 (1.9) | 12 (7.8) | 1 (0.6) |
| Additional OTC medication taken for heartburn/ regurgitation | 152 (98.7) | 0 (0) | 2 (1.3) | 0 (0) |
OTC: over-the-counter.

The present study showed a significant prevalence of GERD in pregnancy (38.5%), with the highest prevalence in the third trimester. In pregnant women with GERD, regurgitation and heartburn developed more frequently in the daytime, and regurgitation was the most common symptom.
The overall prevalence of GERD in Vietnamese pregnant women was 38.5%, which concurs with results from previous studies in Asia. The prospective study by Ho et al. conducted on Singaporean pregnant women reported a prevalence of GERD in pregnancy of 39.9%7. In another longitudinal study in India, the overall prevalence of GERD in pregnant women was 45.5%.
The prevalence of GERD increased in the third trimester, which may be attributed to a cumulative weight gain in that trimester, when the enlarged gravid uterus increases abdominal pressure and promotes reflux symptoms. Said finding is in accordance with several previous studies evaluating the evolution of GERD during pregnancy8,9. In contrast to our finding, the result of the study by Ramya et al. in India was that GERD prevalence decreased across the 3 trimesters10. In that analysis, weight gain was not associated with the risk of GERD in pregnancy. In another Indian study by Rey et al., the prevalence of GERD was similar over the 3 trimesters of gestation, reported to be approximately 25% in each trimester3. The discrepancy could be due to the difference in the research methodology utilized in the studies. Our study is a cross-sectional analysis, whereas the others are longitudinal studies. In Mexico, the prevalence of heartburn or regurgitation, at least once a week, in the general population was 12.1%11. To the best of our knowledge, there are no reports in the literature on the prevalence of GERD during pregnancy in Latin America.
Our study revealed that regurgitation manifested more commonly than heartburn in pregnant women with GERD. That observation concurs with other previous studies that reported the clinical characteristics of GERD in pregnancy10,12. Moreover, our finding is in agreement with another study in Vietnam that reported on the more prevalent manifestation of regurgitation, compared with heartburn, in the general population with GERD13. A majority of our pregnant women with a diagnosis of GERD experienced regurgitation and/or heartburn in the daytime. Although it has been reported that there was an association between supine posture and reflux symptoms, the 24-h esophageal pH monitoring study by Al-Amri et al. demonstrated the predominance of typical reflux symptoms in the daytime, observing that there were more frequent episodes of upright reflux than supine reflux in pregnancy12,14. Most of the pregnant women with GERD in our study complained that their reflux symptoms were aggravated by stress and the consumption of fatty, spicy, or sour foods. Those findings suggest that GERD symptoms are troublesome and impair the quality of life of pregnant women.
In the present study, 20.1% of the pregnant women with GERD had a history of GERD diagnosis. Regurgitation and heartburn before their current pregnancy or during their previous pregnancies were experienced in 50.6 and 14.9% of the pregnant women with GERD, respectively. Those findings indicate that pregnancy might aggravate the existing symptoms of GERD or predispose to the development of GERD.
Among the atypical manifestations of GERD in pregnancy, dry cough at night was reported in 9.1% of our pregnant women with the diagnosis of GERD. That symptom occurred more commonly in the first and second trimesters (13.0 and 17.1%, respectively), compared with the third trimester (2.7%). Our findings were comparable to those of another study conducted in Spain that reported the frequency of cough in each trimester at 8.2, 23.8, and 17.8%, respectively, in pregnant women with typical GERD symptoms15. The mechanisms of cough in GERD include the stimulation of respiratory receptors due to gastric content, aspiration, or the triggering of the esophageal-tracheobronchial cough reflex caused by the presence of acid in the distal esophagus16.
Among our pregnant women with GERD, there was a significant difference in the median GERD-Q scores between the 3 trimesters. The GERD-Q scores were significantly higher in the second and third trimesters (median GERD-Q=8), compared with the first trimester (median GERD-Q=7). Those scores indirectly indicate a marked increase in the frequency of GERD symptoms in the second and third trimesters, compared with the start of the period of gestation.
The first limitation of the present study was the fact that it was not possible to accurately estimate the prevalence of GERD or to accurately compare the GERD reflux symptoms over the course of pregnancy due to its cross-sectional design. We were also unable to evaluate the change of reflux symptoms in pregnancy, compared with the pre-pregnancy period, in individuals with a history of GERD. Therefore, a prospective longitudinal study is needed to evaluate the progression of GERD during pregnancy in the Vietnamese population. The second limitation was that, in our effort to document the overall presence of GERD in pregnancy, the GERD-Q scores could have been affected by our having recruited subjects with GERD that were under treatment. However, since the GERD-Q scores were not the diagnostic criteria of GERD in this study, we believe that the results of the prevalence of GERD in pregnancy were not affected.
In conclusion, our study showed that GERD was prevalent during pregnancy in Vietnam. In the pregnant women with GERD, regurgitation was much more common than heartburn, and those typical reflux symptoms occurred more frequently in the daytime, compared with nighttime.
Financial disclosureNo specific grants from funding agencies in the public, commercial, or non-profit sectors were received in relation to this research.
Conflict of interestThe authors certify that they have no conflicts of interest.
Y-L.T. Le and M.N. Luu equally contributed to the present work.
Please cite this article as: Le Y-LT, Luu MN, Mai LH, Hoang AT, Nguyen TT, Quach DT. Prevalencia y características de la enfermedad por reflujo gastroesofágico en mujeres embarazadas. Rev Gastroenterol Méx. 2023;88:341–346.


www.publicationethics.org.