
Intussusception is an invagination of the intestinal wall into the lumen of the adjacent segment. It is uncommon in adults, responsible for only 1% of cases of intestinal obstruction. It is mainly caused by a neoplastic lesion in the intestinal wall, forming a prominence in the lumen that is displaced during peristalsis.1–3
Inflammatory fibroid polyp (IFP) is an uncommon benign lesion of the gastrointestinal tract that usually presents in the sixth decade of life. It affects both sexes, is generally solitary and sessile, measures from 2-5cm, and originates in the submucosa. IFP etiology is multifactorial and is associated with trauma, allergy, bacterial infection, and physical and chemical agents.4,5
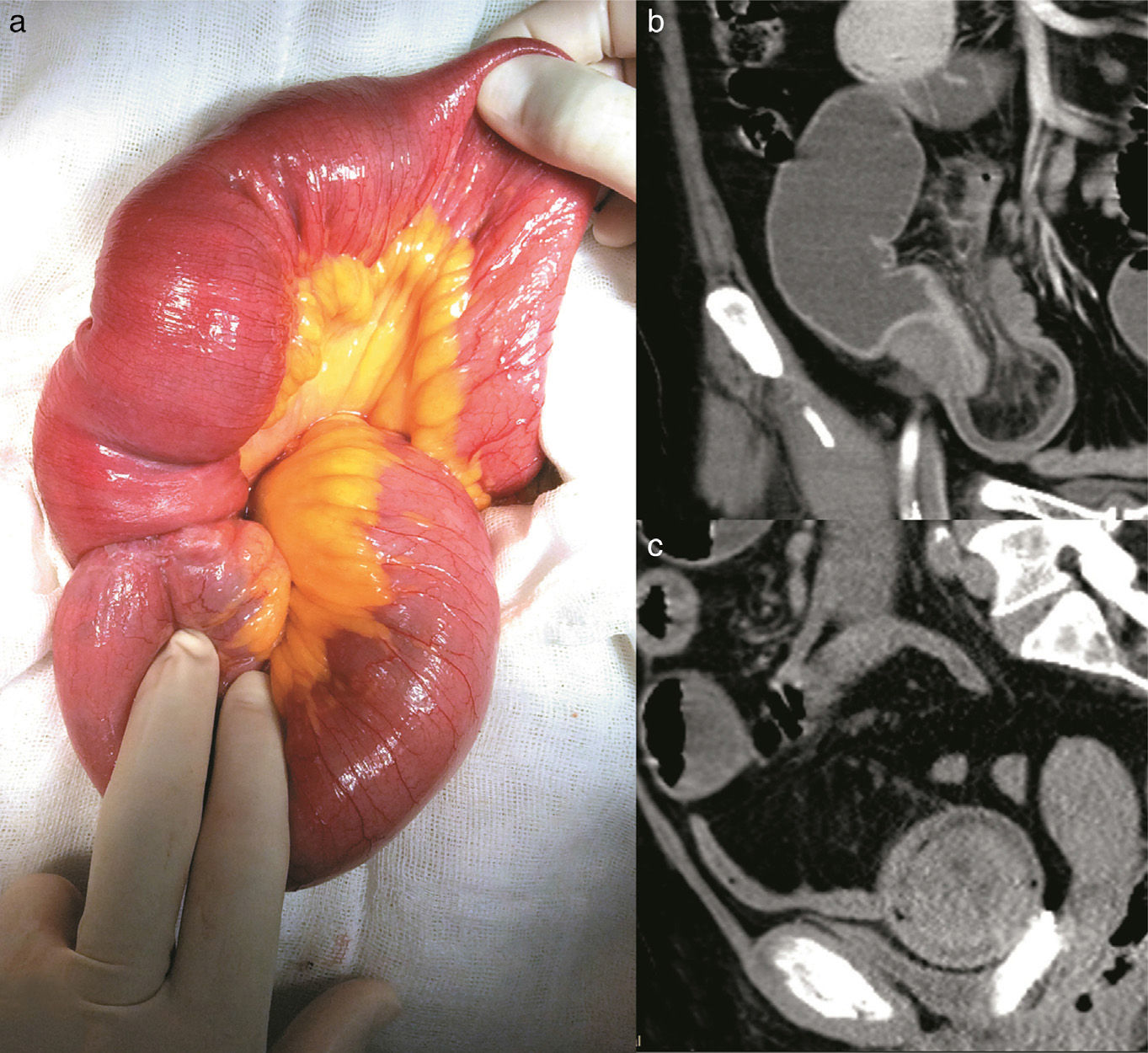
A 58-year-old woman with high blood pressure and dyslipidemia presented with non-radiating colicky abdominal pain of 4-month progression located in the epigastrium. Pain was associated with food ingestion and the patient had a 12-kg weight loss. She came to the emergency department due to intense exacerbation of the pain, abdominal distension, diarrheic stools, and vomiting. Physical examination revealed pale teguments, dehydration, and tachycardia. A deep, mobile, and painful tumor was palpated and so imaging studies were ordered. The Doppler ultrasound study showed a right, well defined, paraovarian cystic lesion measuring 48 x 40 x 41mm with no evidence of vascularity. An abdominal computerized tomography (CT) scan identified a loss of morphology in the terminal ilium, characterized by the absence of folds, a thinning of the wall, retraction and invagination of the adjacent mesentery, and dilated bowel segments, resulting in the diagnosis of intussusception (fig. 1a). An exploratory laparotomy revealed ileo-ileal intussusception (fig. 1b and c) 1 meter from the ileocecal valve that compromised 70cm of bowel segment. The affected bowel segment was resected and an end-to-end anastomosis was performed.
 Small bowel segment with ileo-ileal intussusception, (b) Coronal view of contrast-enhanced CAT scan showing retraction of fat and mesenteric vessels, and (c) Sagittal view of contrast-enhanced CAT scan showing the “target sign” image.")
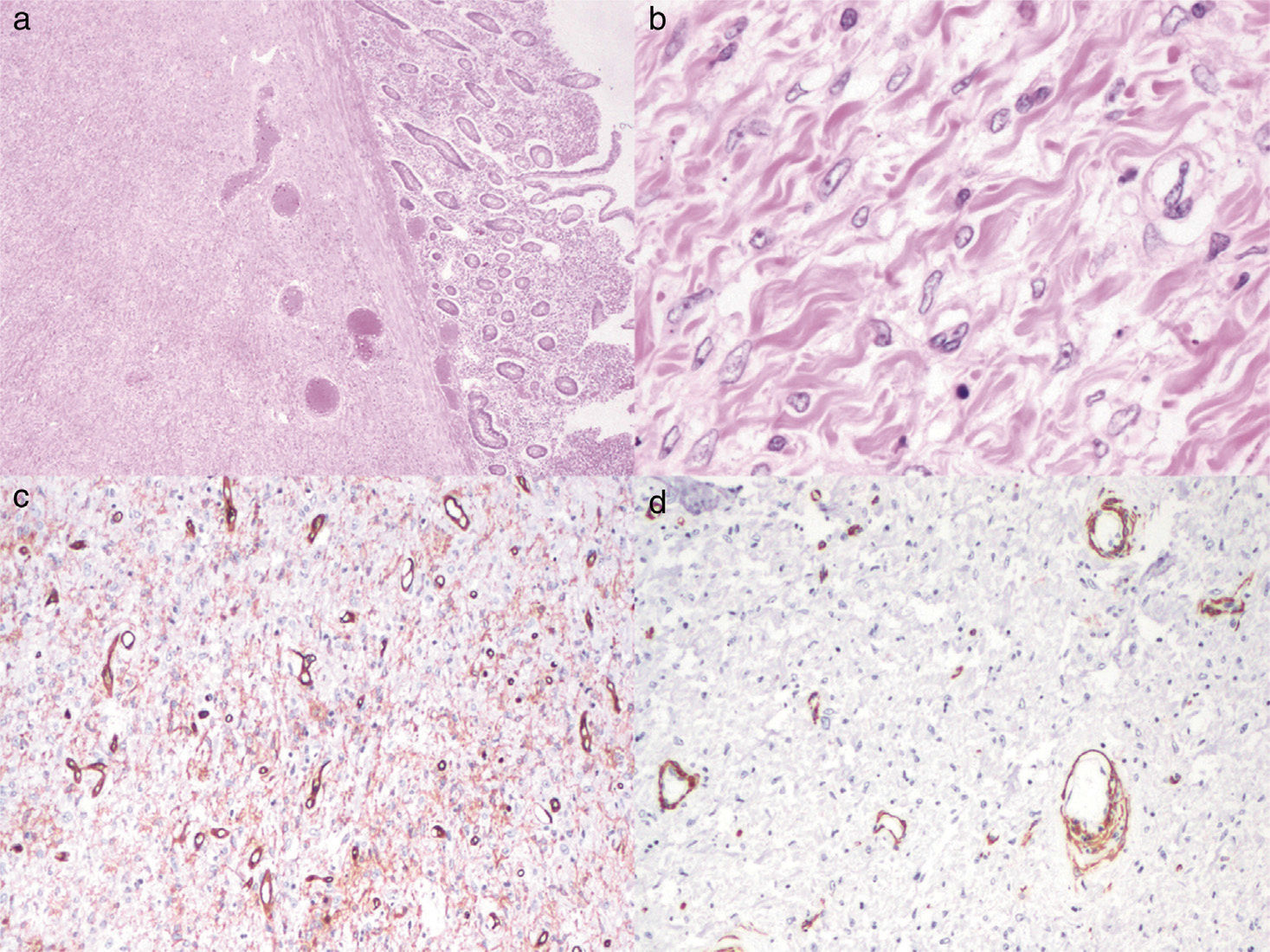
The morphologic analysis of the surgical specimen upon cutting revealed a bright red polypoid lesion partially covered by congestive mucosa that measured 6.3 x 2.9cm and the histologic study identified a submucosal lesion made up of thick collagen bundles, ovoid nuclei with disperse granular chromatin intermixed with lymphocytes, plasma cells, eosinophils, and polymorphonuclear cells. The immunoprofile was positive for CD34, negative for smooth muscle actin (SMA), ALK1, CD117, and Ki67 (fig. 2). Diagnosis was ulcerated IFP with secondary ileal intussusception. The patient was released 7 days after surgery. She was re-evaluated 3 weeks later and showed good progression, passing gases and having bowel movements.
 Histologic slice showing an ulcerated lesion located in the submucosa (hematoxylin & eosin stain x2). (b) Thick collagen bundles and spindle cells with fine granular chromatin nuclei are seen in the lesion (hematoxylin & eosin stain, x40). (c) Immunoreaction positive for CD34. (d) Negative smooth muscle actin.")
(a) Histologic slice showing an ulcerated lesion located in the submucosa (hematoxylin & eosin stain x2). (b) Thick collagen bundles and spindle cells with fine granular chromatin nuclei are seen in the lesion (hematoxylin & eosin stain, x40). (c) Immunoreaction positive for CD34. (d) Negative smooth muscle actin.
Intussusception in adults is uncommon and is associated with up to 90% of the cases of tumors located in the lumen, or is of idiopathic origin.6 The clinical manifestations are diverse, and can be acute, intermittent, or chronic. Bowel obstruction data are generally nausea, vomiting, and abdominal pain in benign neoplastic processes. Melena presents in malignant lesions.2 Depending on their location, they are classified as: ileo-colic, colo-colic, and entero-enteric (jejuno-jejunal, ileo-ileal).4,7 Imaging studies are essential for intussusception diagnosis and CT is the most precise method, demonstrating the presence of intraluminal bowel segments with or without the presence of fat and mesenteric vessels, as well as the classic “target sign”, which is the clear doughnut-shaped mass due to edema, in the transverse views.2,3,8
Treatment is almost always surgical in adults, compared with children, and invariably involves resection of the affected bowel segment together with primary anastomosis.7
IFP is a rare lesion of the gastrointestinal tract and was first described by Vanek in 1949. Also known as inflammatory pseudotumor (IP) or eosinophilic granuloma, IFP is often an incidental discovery during endoscopic procedures or laparotomies. It is generally asymptomatic, but may present with symptoms depending on its location. Its most frequent sites are the stomach (66-75%) and small bowel (18-20%). In the latter location, as in our patient, IFP can cause intussusception in 5-16% of cases.4,9
IFP can be confused with inflammatory myofibroblastic tumor (IMFT) because both were commonly called inflammatory pseudotumor or eosinophilic granuloma. They are histologically different entities. IFPs have more eosinophils, fibrosis, and fewer lymphoid cells than IMFTs. IFPs originate in the submucosa and do not involve the serosa or muscle layer, sites that are generally affected by IMFTs. The immunohistochemical profile of the two lesions is also different: IFPs express CD34, whereas IMFTs express ALK1, smooth muscle actin, and sometimes CD117. It is important to differentiate between the two lesions, given that IFPs do not present with recurrence, whereas IMFTs tend to relapse.10
We present herein a case of IFP that caused intussusception and in which immunohistochemical reactions were used to make the correct diagnostic classification. This is the first case of intussusception secondary to IFP reported in Mexico.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Forasté-Enríquez CF, Mata-Hernández R, Hernández-Villaseñor A, Alderete-Vázquez G, Grube-Pagola P. Oclusión intestinal en el adulto por intususcepción ileal secundaria a pólipo fibroide inflamatorio: reporte de un caso. Revista de Gastroenterología de México. 2017;82:263–265.

