




¿ Introduction
Intussusception is primarily a disease of childhood; only about 5% to 10% occurs in adults. About 90% of adult intussusceptions have a demonstrable cause. Malignant lymphoma of the gastrointestinal tract is a cause of intussusceptions. Surgical resection without reduction of the affected segment is recommended because of the malignant etiology in at least 40% of the cases. In this patient, the etiology of the ileocolic intussusception was a Hodgkin´s lymphoma.
¿ Case report
A 32 year old male was admitted to the emergency room with sudden-onset, crampy abdominal pain, nausea, and vomiting lasting for 10 hours. He had presented with similar symptoms in the past. On physical examination the abdomen was distended, tender and a four centimeters olive-like mass was palpated in the right lower quadrant. Abdominal X-ray showed nonspecific dilation of small-bowel loops. An abdominal tomography was performed and a target sign image was found in proximity to the ileocecal area (Figure 1). A colonoscopy showed a large mass protruding into the cecum through the ileocecal valve (Figure 2). Colonoscopic and tomographic findings were consistent with the diagnosis of ileocolic intussusception and the patient was taken to the operating room for an emergent laparotomy. Intraoperative findings included dilated small bowel and an ileocolic intussusception. The intussusception was not reduced and a right hemicolectomy with stapled ileocolostomy was performed (Figure 3). Pathological examination was consistent with Hodgkin's lymphoma-scleronodular type as the cause of ileocolic intussusception (Figure 4). The patient received postoperative chemotherapy for six months (cyclophosphamide, doxorubicin, vincristine, and prednisone). At seven years follow-up the patient is asymptomatic without evidence of tumor activity and with normal gastrointestinal function.
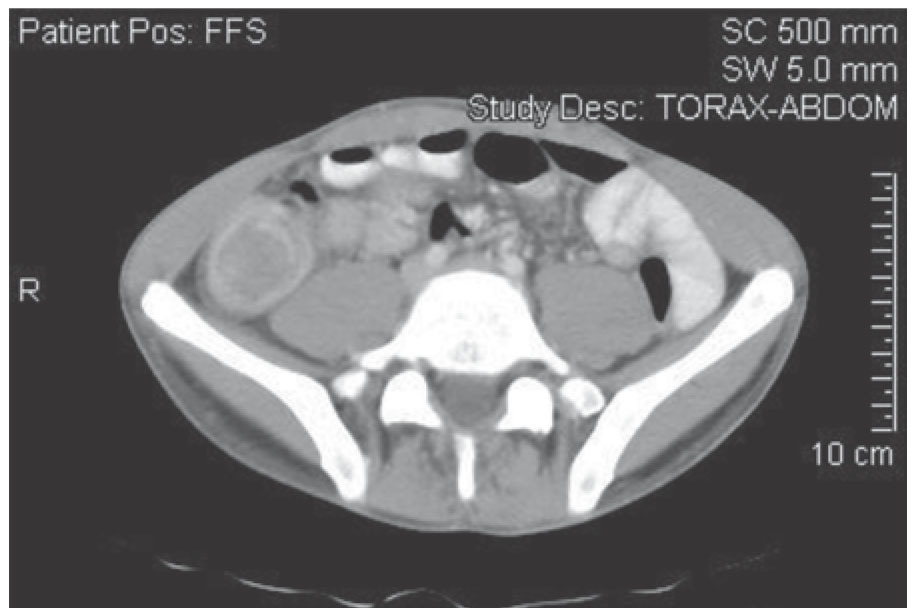
¿ Figure 1. Contrast enhanced CT scans demonstrated an ileocolic intussusception.
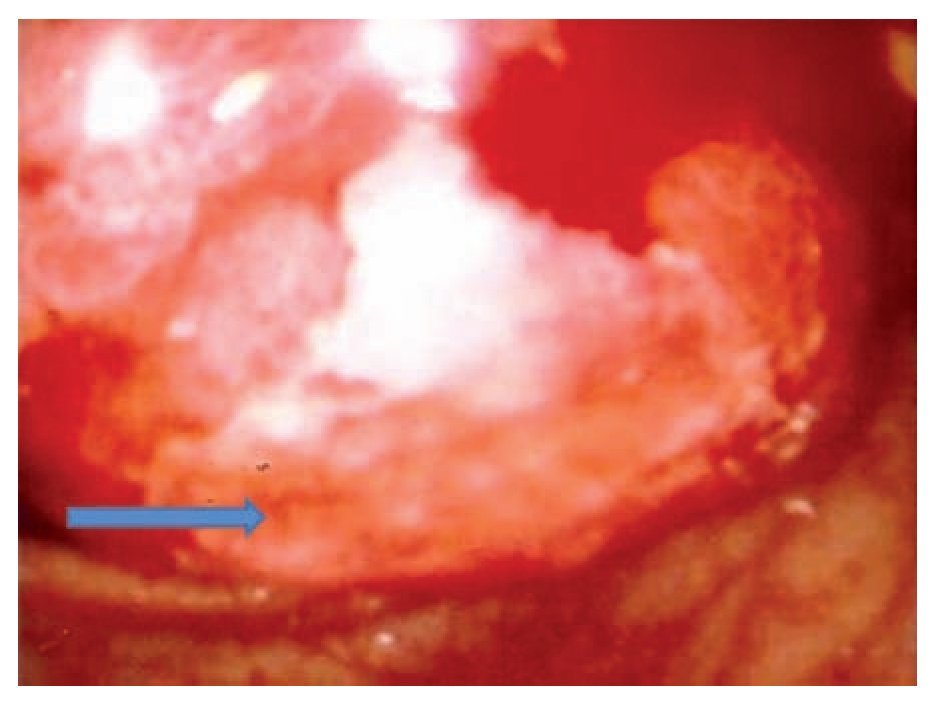
¿ Figure 2. An intracolonic mass is observed during colonoscopy and is consistent with the intussuscepted ileon.

¿ Figure 3. Surgical specimen showing peri-colonic lymphatic nodes increased in size.
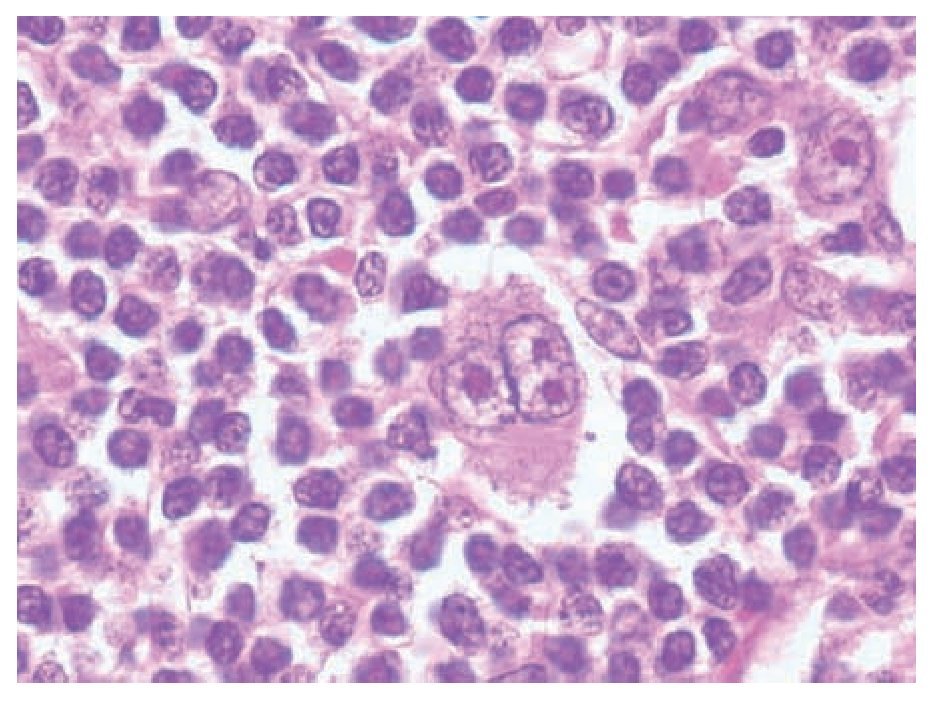
¿ Figure 4. Microscopic view of the tumor. These cells are diagnostic of Hodgkin´s disease.
¿ Discussion
Although intussusception is frequent during childhood, it is a rare condition in adults.1-4 The first description of intussusception appeared in 1793 by Hunter.5 In adults this condition represents 1% to 5% of the total cases of intestinal obstruction with and incidence of 2-3 cases for 1,000,000 inhabitants.1-4 Adults with intussusception have an organic lesion within the intussusception in 70% to 90% of cases.6 In 20% to 55% the etiologic agent is a primary or secondary malignancy.1,2,6,7 and 15% to 25% of cases are due to non-neoplastic conditions including postoperative adhesions, Meckel's diverticulum, infectious lymphoid hyperplasia, trauma, celiac disease, cytomegalovirus colitis, lymphoid hyperplasia secondary to lupus, Henoch-Schönlein purpura,1-7 Non-Hodgkin lymphoma,8 and Wiskott-Aldrich syndrome.9 Intussusception also complicates cystic fibrosis in approximately 1% of patients. Patients with Peutz-Jeghers syndrome, familial polyposis, nephritic syndrome, mesenteric nodes and inverted appendiceal stump are also predisposed to developing intussusceptions.5
The most common age of presentation is around the sixth decade and this is due to the higher incidence of colonic neoplasms in this population.1-3 The clinical presentation of adult intussusception varies considerably. The most common presenting symptoms are abdominal pain, nausea and vomiting, in the acute presentation. Intermittent abdominal pain and vomiting are the major symptoms of subacute or chronic presentations.6 Several imaging techniques may help to establish the diagnosis. These studies include a plain abdominal X-ray which may show an intestinal obstruction and contrast studies that can help to identify the site and cause of intussusception. An upper gastrointestinal series may show "stacked coin" or "coiled spring" appereance. A barium enema examination may be useful in patients with colonic or ileocolic intussusception in which a cup-shaped filling defect is a characteristic finding. Classic ultrasound findings include the target and doughnut sign on a transverse view and the pseudokidney sign in the longitudinal view.6 The computerized tomography (CT) findings of intussusception are virtually pathognomonic.10 In this study the intussusception appears as a mass lesion, representing a thickened segment of bowel which corresponds to the intussusceptum and the intussuscepiens which contains a relatively central area of fat which may show vessels that enhance with the intravenous contrast.6,10 The magnetic resonance imaging (MRI) findings of adult intussusception are similar to those in CT.10 Flexible sigmoidoscopy and colonoscopy are of paramount importance in evaluating intussusception presenting with subacute or chronic large-bowel obstruction.6 Endoscopically, intussusception is seen as an intraluminal mass directed centrally and distally.7 However, the diagnosis made by colonoscopy is rare and most of the times the diagnosis is performed during surgery. In our case, the diagnosis was made prior to surgery on the basis of clinical picture, imaging studies and colonoscopic findings. The treatment of adult intussusception is not universally agreed upon.10 Most authors agree that laparotomy is mandatory, based on the likelihood of an underlying pathologic lesion.6,10 The principle of resection without reduction should be used whenever possible, especially if there is a known neoplasm or if the cause of intussusception is unknown.1,5 The theoretic objections to reduction of grossly viable bowel with mucosal necrosis are: 1) intraluminal seeding and venous embolization of malignant cells in the region of ulcerated mucosa, 2) possible perforation during manipulation, and 3) increased risk of anastomotic complications in the face of edematous and inflamed bowel.6 In patients with small bowel intussusception, reduction must be initially attempted unless signs of bowel ischemia or inflammation are present or if malignancy is suspected.1,6
¿ Conclusion
Intussusception in adults is a rare condition and represents a challenge for the surgeon. Imaging studies are essential to establish the diagnosis preoperatively. During surgery, when malignancy is suspected to be the cause of the intussusception, it is best to perform a resection of the affected bowel without reduction of the bowel to avoid the dissemination of neoplastic cells.
Correspondence: Enrique Luque de León M.D.
Carlos Graef Fernández 154-517, Col. Tlaxala, CP 05300, México City.
Fax: (5255) 1664 7164.
E-mail: eluque@prodigy.net.mx
Recibido el 14 de mayo de 2010;
aceptado el 13 de julio de 2010.

