
The growing elderly population and wide use of capsule endoscopy have led to a higher number of procedures in those patients. The aim of the present study was to assess the usefulness of capsule endoscopy in older patients.
Materials And MethodsAll consecutive patients undergoing capsule endoscopy at our center within the time frame of 2004-2016 were classified as older (≥75 years of age) and younger. Findings and diagnostic yield were comparatively assessed.
ResultsOf 2311 patients (mean age: 59.5 ± 19.23 years, 44.48% male), 648 were in the older group and 1663 in the younger group. Gastric transit time was shorter in the older patients (p=0.001), whereas small bowel transit time was shorter in the younger patients (p<0.001). Overall diagnostic yield in the elderly was higher (50.66% vs. 41.19%, p<0.001). Obscure gastrointestinal bleeding was the most frequent indication for capsule endoscopy in the elderly (90.4% vs. 53.77%, p<0.001), achieving a higher diagnostic yield than in the younger population (51.47% vs. 42.76%, p=0.002), whereas Crohn's disease, suspected or known neoplasms/polyps, malabsorption syndrome, and abdominal pain were the indications in the younger patient group. Such indications were rare in the older group. Vascular lesions and active bleeding were more frequently diagnosed in the older patients, whereas ulcers/erosions and mucosal atrophy were more common in the younger patients (p<0.001).
ConclusionsCapsule endoscopy achieved a higher overall diagnostic yield in the elderly patients. Obscure gastrointestinal bleeding indication for capsule endoscopy was much more frequent in the advanced-age group and had a higher diagnostic yield.
La creciente población anciana y el uso amplio de la endoscopia por cápsula han llevado a una cantidad mayor de procedimientos en aquellos pacientes. El objetivo del presente estudio fue valorar la utilidad de la endoscopia por cápsula en pacientes mayores.
Materiales y MétodosSe clasificó a todos los pacientes consecutivos en nuestro centro sometidos a cápsula endoscópica (CE) dentro del periodo de tiempo 2004-2016 como mayores (≥75 años) y más jóvenes. Los hallazgos y el rendimiento de diagnóstico se valoraron comparativamente.
ResultadosDe 2,311 pacientes (edad promedio: 59.5 ± 19.23 años, 44.48% hombres), 648 se encontraban en el grupo de mayores y 1,663 en el grupo de más jóvenes. El tiempo de tránsito gástrico fue más corto en los pacientes mayores (p=0.001), mientras que el tiempo de tránsito del intestino delgado fue más corto en el grupo de pacientes más jóvenes (p<0.001). El rendimiento de diagnóstico global fue más alto en los ancianos (50.66% vs. 41.19%, p<0.001). El sangrado gastrointestinal de origen oscuro fue la indicación más frecuente para la endoscopia por cápsula en los ancianos (90.4% vs. 53.77%, p<0.001), logrando un rendimiento de diagnóstico más alto que en la población más joven (51.47% vs. 42.76%, p=0.002), mientras que la enfermedad de Crohn, sospecha o conocimiento de neoplasmas/pólipos, síndrome de malabsorción, y dolor abdominal fueron las indicaciones en el grupo de pacientes más jovenes. Tales indicaciones fueron poco comunes en el grupo de mayores. Se diagnosticó con mayor frecuencia las lesiones vasculares y el sangrado activo en los pacientes mayores, mientras que las úlceras/erosiones y la atrofia muscular fueron más comúnes en los pacientes más jóvenes (p<0.001).
ConclusionesLa endoscopia por cápsula logró un rendimiento de diagnóstico global más alto en los pacientes ancianos. La indicación de sangrado gastrointestinal de origen oscuro para endoscopia por cápsula fue mucho más frecuente en el grupo de edad avanzada y presentó un rendimiento de diagnóstico mayor.
Capsule endoscopy (CE) has been shown to be a useful non-invasive procedure to assess small bowel (SB) pathology.1 Features predicting CE diagnostic yield have been evaluated, particularly in obscure gastrointestinal bleeding (OGIB).2 Furthermore, the growing elderly population and widespread use of CE have led to a higher number of procedures carried out in those patients. Twenty percent of elderly patients have a negative upper and lower endoscopy and two thirds of them have a lesion in the SB.3 However, the influence of aging on CE remains unclear.
The overall diagnostic yield of CE has been shown to increase in older patients,4 especially in cases of iron deficiency anemia.5 At present, most studies assess the usefulness of CE in older patients in the OGIB setting. Vascular lesions have frequently been reported in the elderly population presenting with OGIB, with angioectasia as the most common finding.6 The difference in diagnostic yield in older and younger populations for other types of lesions, such as ulcers or tumours,7,8 remains controversial. In addition, there are currently few studies evaluating the usefulness of CE in the elderly for other indications. The aim of our study was to comparatively assess the indications and usefulness of CE in patients over and under 75 years of age.
Materials and methodsPatients and CE procedureAll data from consecutive patients undergoing CE at our referral center within the time frame of January 2004 and August 2016 were retrieved from a prospectively collected database. Age, sex, and demographic variables were registered. The CE wireless camera (PillCam SB1-SB3, Medtronic, Minneapolis, Minnesota, USA) was swallowed by the patient or administered by a capsule endoscopy camera delivery device (US Endoscopy, OH, USA), after an 8 to12-h fast. No bowel preparation or previous prokinetic agents were administered. Gastric and SB transit times were considered. Total enteroscopy of the entire SB was achieved when the CE reached the cecum within the recording time. A valid CE was established by the endoscopist, based on the quality of cleansing and CE-related adverse events. Expert endoscopists read the procedures (more than 500 explorations).
CE indications were classified as follows: obscure gastrointestinal bleeding (OGIB); suspected or known Crohn's disease; suspected or known neoplasm/polyps; malabsorption syndrome (including celiac disease); graft-versus-host-disease; Lynch syndrome; polyposis syndrome; chronic abdominal pain; control post-double balloon enteroscopy (DBE) therapy, and others. OGIB was categorized into overt OGIB and occult OGIB. Findings identified through CE were categorized into the followings groups: vascular lesions, ulcers or multiple erosions, polyp/mass, diverticulum, active bleeding with no identifiable cause, mucosal atrophy, stricture, and others. The lesions were considered clinically significant (positive diagnostic yield) if they could explain the clinical presentation of the patient in accordance with the CE indication. If that did not occur, the procedure was considered negative. In relation to SB bleeding, cases of lymphangiectasia, indeterminate red spots, isolated erosions, and any entity that could not explain the patient's clinical presentation were classified as negative. If several lesions with potential bleeding were diagnosed, only the one with the highest potential was retained for the analysis. Lesion location was determined by the transit time ratio relative to the pylorus and/or the ileocecal valve. CE-related complications were also considered. A written statement of informed consent prior to the procedure was provided in all cases.
Statistical AnalysisTo calculate the diagnostic yield of CE in the elderly, patients were classified into two groups, according to a cut-off point of 75 years of age or older at the time of CE. A comparative analysis between the two groups regarding CE indications, clinically significant lesions, and findings was carried out. Categorical variables were compared using the χ2-test or Fisher's exact test. The continuous variables with normal distribution were analyzed through the Student's t test, and those with non-normal distribution were analyzed through the Mann-Whitney U test. Data were presented as the mean ± standard deviation (SD) or median (range), respectively. The 95% confidence interval (CI) was calculated and a p-value < 0.05 was considered statistically significant. SPSS software version 23 was used (IBM; SPSS Inc., Chicago, IL, USA).
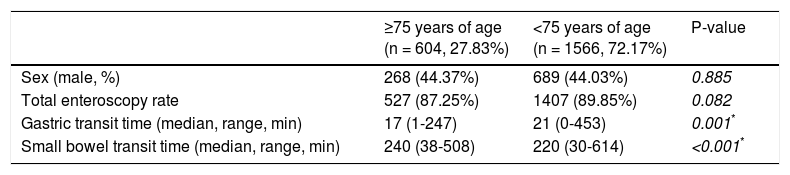
ResultsPatientsA total of 2311 underwent CE within the time frame of 2004 and 2016 at our referral center. Overall, 141 CEs were non-valid due to esophageal/gastric retention (n = 79), poor SB cleansing (n = 42), and failed technique (n = 20). Thus, 2170 patients (mean age: 59.5±19.23 years, 44.1% male) had a valid CE and were included in the study. Total examination of the SB was achieved in 89.12% of the cases. Gastric and SB median times were 20 (range: 0-453) and 226 (range: 30-614) minutes, respectively. A capsule endoscope introductory device was used in 12 (1.99%) patients above 75 years of age and 19 (1.21%) patients below 75 years of age (p=0.174). All patients with valid CE were classified as ≥75 (n = 604) and <75 years of age (n = 1566). Patient characteristics are shown in Table 1.
Patient characteristics (n = 2170).
| ≥75 years of age (n = 604, 27.83%) | <75 years of age (n = 1566, 72.17%) | P-value | |
|---|---|---|---|
| Sex (male, %) | 268 (44.37%) | 689 (44.03%) | 0.885 |
| Total enteroscopy rate | 527 (87.25%) | 1407 (89.85%) | 0.082 |
| Gastric transit time (median, range, min) | 17 (1-247) | 21 (0-453) | 0.001* |
| Small bowel transit time (median, range, min) | 240 (38-508) | 220 (30-614) | <0.001* |
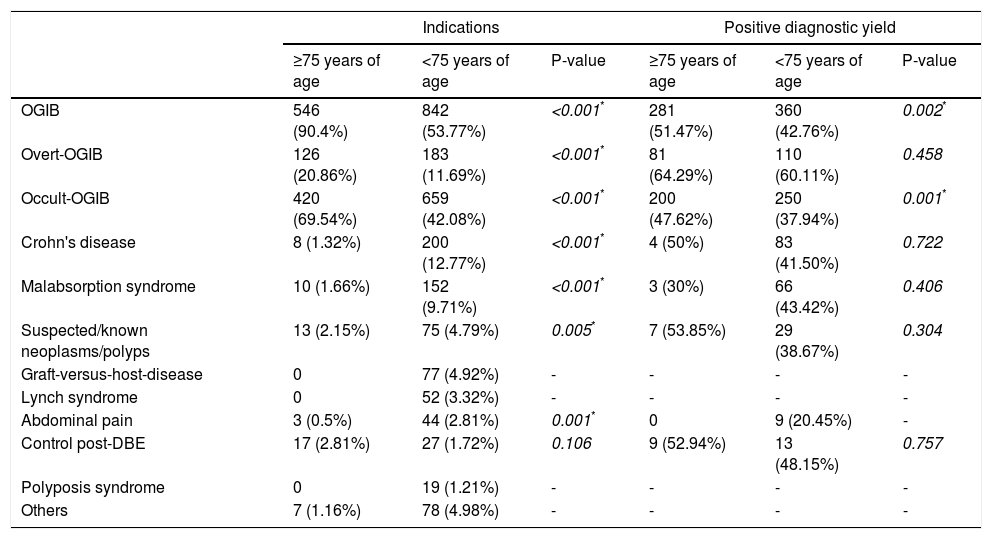
The most frequent indication for CE in both age groups was OGIB (Table 2). This indication was more common in the older patients (90.4% vs. 53.77%, p<0.001), achieving a higher CE diagnostic yield (51.47% vs. 42.76%, p=0.002). A different diagnostic yield in the elderly was not achieved in the overt OGIB subgroup analysis (64.29% vs. 60.11%, p=0.458). Crohn's disease, suspected or known neoplasms/polyps, malabsorption syndrome, and chronic abdominal pain were more frequent indications in the young patients.
Capsule endoscopy indications and associated positive diagnostic yield by age groups.
| Indications | Positive diagnostic yield | |||||
|---|---|---|---|---|---|---|
| ≥75 years of age | <75 years of age | P-value | ≥75 years of age | <75 years of age | P-value | |
| OGIB | 546 (90.4%) | 842 (53.77%) | <0.001* | 281 (51.47%) | 360 (42.76%) | 0.002* |
| Overt-OGIB | 126 (20.86%) | 183 (11.69%) | <0.001* | 81 (64.29%) | 110 (60.11%) | 0.458 |
| Occult-OGIB | 420 (69.54%) | 659 (42.08%) | <0.001* | 200 (47.62%) | 250 (37.94%) | 0.001* |
| Crohn's disease | 8 (1.32%) | 200 (12.77%) | <0.001* | 4 (50%) | 83 (41.50%) | 0.722 |
| Malabsorption syndrome | 10 (1.66%) | 152 (9.71%) | <0.001* | 3 (30%) | 66 (43.42%) | 0.406 |
| Suspected/known neoplasms/polyps | 13 (2.15%) | 75 (4.79%) | 0.005* | 7 (53.85%) | 29 (38.67%) | 0.304 |
| Graft-versus-host-disease | 0 | 77 (4.92%) | - | - | - | - |
| Lynch syndrome | 0 | 52 (3.32%) | - | - | - | - |
| Abdominal pain | 3 (0.5%) | 44 (2.81%) | 0.001* | 0 | 9 (20.45%) | - |
| Control post-DBE | 17 (2.81%) | 27 (1.72%) | 0.106 | 9 (52.94%) | 13 (48.15%) | 0.757 |
| Polyposis syndrome | 0 | 19 (1.21%) | - | - | - | - |
| Others | 7 (1.16%) | 78 (4.98%) | - | - | - | - |
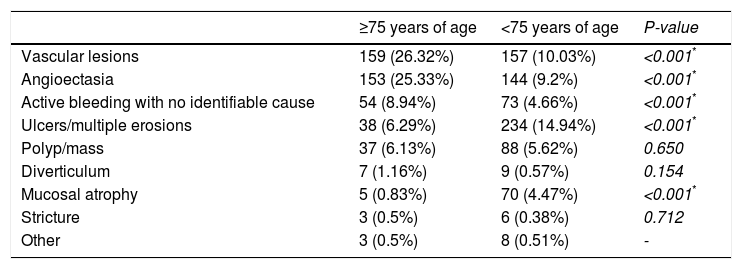
Overall diagnostic yield in the elderly population was higher than in the young patients (50.66% vs. 41.19%, p<0.001). Vascular lesions and active bleeding were more frequent in the elderly patients, whereas ulcers/erosions and SB atrophy were more common in the young patients (p<0.001) (Table 3). Regarding location, jejunal lesions were more frequent in the advanced age patients (60.46% vs. 50.54%, p<0.001), whereas ileal lesions were more common among the patients under 75 years of age (17.32% vs. 28.84%, p<0.001). There were no differences in the non-SB location rate (stomach and colon) between the two groups (12.09% vs. 8.37%, p=0.069). There were no lesions located in the esophagus observed through CE. Vascular lesions (n = 159, 26.32%) were the most frequent findings in patients aged 75 years or older. Almost all the lesions (97.48%) were diagnosed when the CE indication was OGIB (Table 4) and were duodenal (n = 17, 10.76%), jejunal (n = 109, 68.99%), ileal (n = 23, 14.47%) or non-SB (n = 10, 6.29%). Angioectasia (n = 153, 25.33%) was the most common finding; 72 (47.05%) patients had multiple lesions and 50 (32.68%) had active bleeding. The presence of multiple angioectasias was not statistically different in the older and younger groups (47.05% vs. 39.58%, p=0.194). Dieulafoy's lesion (n = 2), varices (n = 2), and arteriovenous malformation (n = 2) were also found. Bleeding as the sole finding was mainly detected in the jejunum (n = 26, 48.15%) and the ileum (n = 8, 14.81%), but 14 patients (25.93%) presented with colonic active bleeding and no identified lesion. All SB diverticula (n = 7) were diagnosed in patients with CE indication for OGIB.
Findings by capsule endoscopy according to age groups for all indications.
| ≥75 years of age | <75 years of age | P-value | |
|---|---|---|---|
| Vascular lesions | 159 (26.32%) | 157 (10.03%) | <0.001* |
| Angioectasia | 153 (25.33%) | 144 (9.2%) | <0.001* |
| Active bleeding with no identifiable cause | 54 (8.94%) | 73 (4.66%) | <0.001* |
| Ulcers/multiple erosions | 38 (6.29%) | 234 (14.94%) | <0.001* |
| Polyp/mass | 37 (6.13%) | 88 (5.62%) | 0.650 |
| Diverticulum | 7 (1.16%) | 9 (0.57%) | 0.154 |
| Mucosal atrophy | 5 (0.83%) | 70 (4.47%) | <0.001* |
| Stricture | 3 (0.5%) | 6 (0.38%) | 0.712 |
| Other | 3 (0.5%) | 8 (0.51%) | - |
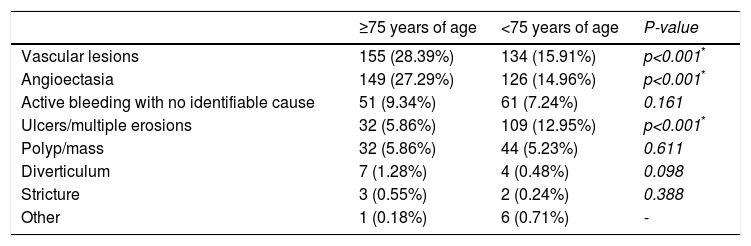
Findings by capsule endoscopy in the obscure gastrointestinal bleeding setting.
| ≥75 years of age | <75 years of age | P-value | |
|---|---|---|---|
| Vascular lesions | 155 (28.39%) | 134 (15.91%) | p<0.001* |
| Angioectasia | 149 (27.29%) | 126 (14.96%) | p<0.001* |
| Active bleeding with no identifiable cause | 51 (9.34%) | 61 (7.24%) | 0.161 |
| Ulcers/multiple erosions | 32 (5.86%) | 109 (12.95%) | p<0.001* |
| Polyp/mass | 32 (5.86%) | 44 (5.23%) | 0.611 |
| Diverticulum | 7 (1.28%) | 4 (0.48%) | 0.098 |
| Stricture | 3 (0.55%) | 2 (0.24%) | 0.388 |
| Other | 1 (0.18%) | 6 (0.71%) | - |
The elderly patients presenting with ulcers or multiple erosions (n = 38, 6.29%) underwent a CE because of occult OGIB (n = 29), overt OGIB (n = 5), Crohn's disease (n = 3), and suspicion of SB tumor (n = 1). They were finally diagnosed with NSAID-induced enteropathy (n = 10), non-specific enteropathy (n = 8), anastomotic ulcer (n = 6), Crohn's disease (n = 5), isolated non-specific ulcer (n = 5), portal hypertensive enteropathy (n = 3), and radiation enteropathy (n = 1). Only 5 patients presented with atrophy revealed through CE that was indicated for suspicion of complicated celiac disease. Of the 648 patients ≥75 years of age that underwent a CE, two had video capsule retention in the SB (0.31%) resolved by double-balloon enteroscopy. One of the patients with capsule endoscope retention in the SB had a capsule-related perforation and underwent emergency surgery.
Discussion and conclusionsAs the population ages, there is a trend towards performing many more CE studies in elderly patients because of the less-invasive and virtually complete exploration of the SB it provides. Thus, knowledge of possible differences in indications, diagnostic yield, complete study rate, and adverse events could be crucial. We reported on a large case series of 2311 patients classified as ≥75 (n = 648) years of age and <75 years of age (n = 1663) that underwent CE.
There is no consensus on the effect elderly populations have on video capsule transit times and total SB visualization rates.9,10 Gastric retention and delayed gastric emptying are major limitations in CE explorations, because they indirectly influence capsule transit times. Diabetes and advanced age have been described as factors related to increased gastric time. There are few studies regarding the relationship of SB transit time with ageing and that association remains unclear. Papadopoulos et al.6 reported no difference in SB transit time between patients over and under 65 years of age, whereas other authors11 described a longer SB transit time in older patients. In the present study, gastric transit time was shorter in older patients and SB transit time was shorter in younger patients. We found longer SB transit times in the elderly, but no differences for total enteroscopy rates, even though completion rates in elderly patients are expected to be lower due to multiple factors (drug therapies, in-patient status, comorbidities, etc.).
Cases of OGIB significantly increased with the intake of oral antithrombotic agents among the elderly, because of prolonged small intestine transit time.12 Muhammad et al.5 demonstrated that the diagnostic yield of CE progressively increased with advancing age and was highest among patients over 85 years of age. In our study, diagnostic yield in the elderly patients was also higher than in the young patients (50.66% vs. 41.19%, p<0.001), mainly due to a high angioectasia detection rate. OGIB was a more frequent indication in the elderly patients (90.4% vs. 53.77%, p<0.001) and achieved a higher diagnostic yield than in the younger population (51.47% vs. 42.76%, p=0.002). Other indications in patients 75 years of age or older were rare. Vascular lesions and active bleeding with no identifiable cause were more frequently diagnosed in the older patients, whereas ulcers/erosions and mucosal atrophy were more common in the younger patients (p<0.001). Interestingly, we found that angioectasias were mainly distributed in the proximal SB (jejunum). This observation was recently described by Kaufman et al.13 in a retrospective study in which video capsule transit time in the SB was divided and studied in quartiles. Vascular lesions were located in the first quartile of said transit time in more than 60% of the cases.
Most studies to date assess the role of CE in elderly populations that underwent the procedure because of OGIB or iron deficiency anemia, using different age cut-off points (65-85 years) to classify the older patients. In a prospective study of 48 patients referred for OGIB, Scaglione et al.14 concluded that advanced age (>65 years) was associated with increased CE yield. We also confirmed a higher overall diagnostic yield in patients 75 years of age or older (50.66% vs. 41.19%, p<0.001). A significant correlation between age and the rate of SB angioectasia has also been described.12,15 However, other studies reported a lower rate of angioectasia in patients ≥80 years of age.8 In our study, OGIB was a more frequent indication for CE in the elderly patients (90.4% vs. 53.77%, p<0.001), achieving a higher diagnostic yield than in the younger population (51.47% vs. 42.76%, p=0.002). Occult OGIB presentation was the main indication for CE in the older patients (76.92%), achieving a 47.62% diagnostic yield. Notably, 20.86% of the advanced-age patients presented with overt OGIB, compared with 11.69% in the younger population. The non-negligible impact of acute overt OGIB in advanced-age patients with comorbidities may be more severe than in younger patients.16 There were no differences in the diagnostic yield of overt presentation between the two age groups in our analysis. According to previous descriptions, more patients presenting with OGIB in the older group were diagnosed with angioectasia (28.39% vs. 14.96%, p<0.001). A total of 14.94% of young patients presented with ulcers or multiple erosions, compared with 6.29% in the older group of patients (p<0.001). That could be related to a much higher indication for CE due to Crohn's disease in younger patients.17 On the other hand, NSAID-induced enteropathy was the main cause of SB ulcers in the elderly.
Thus, CE indications other than OGIB are much less frequent in older patients.4 In our study, the 2.15, 1.66, 1.32, and 0.5% of the older patients underwent CE because of suspected or known neoplasms, malabsorption syndrome, Crohn's disease, and chronic abdominal pain, respectively. CE was only indicated for graft-versus-host-disease, Lynch syndrome, and polyposis syndrome (Peutz-Jeghers syndrome in all cases) in patients under 75 years of age. In addition, the high prevalence of CE indication for graft-versus-host-disease in our case series may have increased the retention rates.18,19 Colon capsule endoscopy has also been described as an alternative approach for the examination of the colon in patients that refuse colonoscopy or that have had incomplete colonoscopy,20,21 but this technique was not considered in our study.
The main strength of the present study was the evaluation of the large number of patients with various CE indications. Among the limitations of our study were: the retrospective and single-center nature of the study, the lack of data regarding comorbid conditions for patients undergoing CE, patient hospitalization status, and the extensive period of study. Referral bias also may have influenced the results.
In conclusion, the present study confirmed the usefulness of CE in an elderly population and showed that CE achieved a higher diagnostic yield in the advanced-age population than in the younger patients. As expected, the primary CE indication was significantly different between the two age groups. OGIB as the indication for CE was much more frequent in the older group of patients and had a higher diagnostic yield, due to the angioectasia detection rate. Indications other than OGIB were rare and ulcers/erosions were less frequent.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Pérez-Cuadrado-Robles E, Zamora-Nava LE, Jiménez-García VA, Pérez-Cuadrado-Martínez E. Indicaciones y rendimiento diagnóstico de la cápsula endoscópica en el anciano. Revista de Gastroenterología de México. 2018;83:238–244.

