

Peutz-Jeghers syndrome is an autosomal dominant inherited pathology characterized by gastrointestinal hamartomatous polyps, predominantly in the small bowel, and pigmented mucocutaneous lesions. Guidelines suggest polypectomy with a balloon-assisted enteroscope when polyps are larger than 10mm. Complications in adults can be as high as 6.8%, but there is little information on pediatric populations. Our aim was to describe the safety and efficacy of polypectomy in a group of pediatric patients with Peutz-Jeghers syndrome using balloon-assisted enteroscopy.
Materials and methodsA retrospective study was conducted at the Hospital de Especialidades del Centro Médico Nacional Siglo XXI on pediatric patients with Peutz-Jeghers syndrome that required balloon-assisted enteroscopy and polypectomy within the time frame of January 2010 and December 2015. Patients that underwent polypectomy with a push enteroscope were excluded from the study.
ResultsA total of 35 polypectomies were performed on 4 patients (female/male: 3/1). The mean age of the patients was 13.7 years (range:11-16). Twelve enteroscopies were carried out, 8 of which were anterograde. A single-balloon enteroscope was used in 7 procedures and a double-balloon enteroscope in 5. The mean size of the polyps was 1.6cm (range: 1-4cm). A major complication (acute pancreatitis) presented in only one case (8.3%). No other major complications associated with the procedures were observed.
ConclusionBalloon-assisted enteroscopy with polypectomy in children is a safe and effective procedure, with complications similar to those reported in adults.
El síndrome de Peutz-Jeghers (SPJ) es una enfermedad hereditaria, autosómica dominante caracterizada por la presencia de pólipos hamartomatosos en el tubo digestivo de predominio en el intestino delgado y que se acompañan de lesiones mucocutáneas pigmentadas. Algunas guías proponen la realización de polipectomía con enteroscopio asistido por balones (EAB) cuando los pólipos sean mayores de 10mm. Las complicaciones en población adulta puede ser tan altas como 6.8%, sin embargo, en población pediátrica hay poca información. Nuestro objetivo es describir la seguridad y eficacia de la polipectomía en un grupo de pacientes pediátricos con SPJ tratados con EAB.
Material y métodosEs un estudio retrospectivo realizado en el Hospital de Especialidades del Centro Médico Nacional Siglo XXI entre enero del 2010 y diciembre del 2015. Se incluyó a todos los pacientes pediátricos con SPJ que requirieron EAB y polipectomía. Se excluyeron las polipectomías realizadas con enteroscopia de empuje.
ResultadosSe realizaron un total de 35 polipectomías en 4 pacientes (femenino/masculino: 3/1). La edad media de los pacientes fue 13.7 (11-16) años. Se llevaron a cabo 12 enteroscopias, 8 de ellas anterógradas. El enteroscopio monobalón se utilizó en 7 procedimientos y el doble-balón en 5. El tamaño promedio de los pólipos fue de 1.6cm (1-4cm). Se presentó una complicación mayor (pancreatitis aguda) en un solo caso (8.3%). No se observaron otras complicaciones mayores.
ConclusiónEl uso de EAB con polipectomía en niños es un procedimiento seguro y efectivo con complicaciones similares a las reportadas en adultos.
Peutz-Jeghers syndrome (PJS) is an autosomal dominant inherited pathology characterized by gastrointestinal hamartomatous polyps, predominantly in the small bowel, and pigmented mucocutaneous lesions.1 The mean age of presentation of polyps is between 11 and 13 years and approximately 50% of patients will present with some type of symptom before 20 years of age. The most common symptoms in PJS are anemia, rectal bleeding, abdominal pain, obstruction, or intussusception.2 The current American Society of Gastrointestinal Endoscopy and the European Society of Gastrointestinal Endoscopy guidelines recommend polypectomy with enteroscopy in adult patients with polyps larger than 10mm, previously observed through radiologic methods or capsule endoscopy.3,4 Enteroscopy for intestinal polyp resection in adult patients with PJS has been reported to be successful and safe,5 but there is little information on the efficacy and safety of small bowel polypectomy through enteroscopy in children with JPS. The aim of the present study was to report on the experience in this respect at a tertiary care hospital center.
Materials and methodsA retrospective, descriptive, and observational study was carried out in which the data were reviewed of all patients with PJS that underwent balloon-assisted enteroscopy (BAE) with either a single balloon (SBE) or a double balloon (DBE) at the Endoscopy Service of the Hospital de Especialidades del Centro Médico Nacional Siglo XXI of the Instituto Mexicano del Seguro Social, within the time frame of January 2010 and December 2015. All the patients with PJS under 18 years of age that underwent small bowel polypectomy for polyps larger than 1cm using SBE or DBE were included in the study, and all the patients that had push enteroscopy or intraoperative enteroscopy were excluded. The polypectomy technique consisted of submucosal injection of adrenaline diluted with saline solution (1:20,000) to raise the polyps and then resect them with a polypectomy loop, using the cut and clot method (fig. 1). Hemoclips were placed when there was bleeding after the cut. Minor complications were defined as those that were not life-threatening for the patient and that did not warrant hospital surveillance. Major complications were those that put the patient's life at risk and that required hospitalization.
 Polyp in the small bowel before resection and B) after resection.")
For the statistical analysis, the means of the variables and their ranges (minimum and maximum) were calculated.
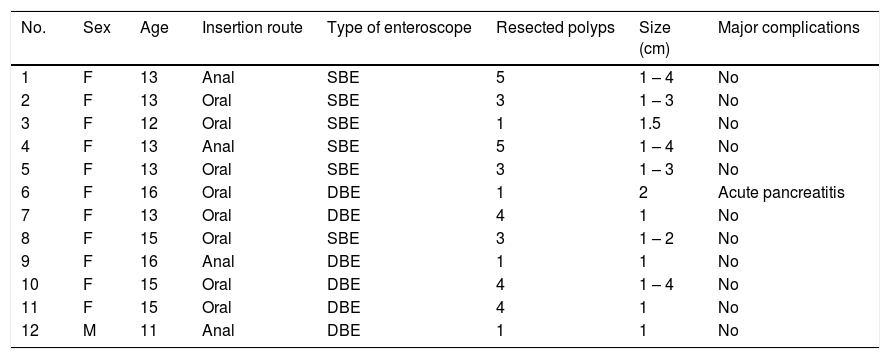
ResultsA total of 35 polypectomies in 12 enteroscopies were performed on 4 patients, three of whom were girls. The mean age of the patients was 13.7 years (range: 11-16 years). Eight anterograde enteroscopies and 4 retrograde enteroscopies were carried out. SBE was utilized in 7 procedures and DBE in 5. A mean of 2.9 polyps were resected per enteroscopy (range: 1-5 polyps) and the mean size of the polyps was 1.6cm (range:1-4cm). One patient required the placement of 2 hemoclips secondary to bleeding after polypectomy during the same enteroscopy. The only major complication registered was in one female patient that underwent polyp resection through anterograde DBE. She presented with acute pancreatitis secondary to the procedure, demonstrated through laboratory studies, and needed 4 days of hospitalization. No other major complications were demonstrated in the other procedures (Table 1).
Characteristics, results, and complications of the enteroscopies.
| No. | Sex | Age | Insertion route | Type of enteroscope | Resected polyps | Size (cm) | Major complications |
|---|---|---|---|---|---|---|---|
| 1 | F | 13 | Anal | SBE | 5 | 1 – 4 | No |
| 2 | F | 13 | Oral | SBE | 3 | 1 – 3 | No |
| 3 | F | 12 | Oral | SBE | 1 | 1.5 | No |
| 4 | F | 13 | Anal | SBE | 5 | 1 – 4 | No |
| 5 | F | 13 | Oral | SBE | 3 | 1 – 3 | No |
| 6 | F | 16 | Oral | DBE | 1 | 2 | Acute pancreatitis |
| 7 | F | 13 | Oral | DBE | 4 | 1 | No |
| 8 | F | 15 | Oral | SBE | 3 | 1 – 2 | No |
| 9 | F | 16 | Anal | DBE | 1 | 1 | No |
| 10 | F | 15 | Oral | DBE | 4 | 1 – 4 | No |
| 11 | F | 15 | Oral | DBE | 4 | 1 | No |
| 12 | M | 11 | Anal | DBE | 1 | 1 | No |
F: female; M: male; SBE: single-balloon enteroscope; DBE: double-balloon enteroscope
Different studies have shown that the resection of intestinal polyps larger than 1cm is safe in adults with PJS. In addition, that procedure significantly reduces the number of future surgeries required. Endoscopic treatment should always be initially attempted, given that the effectiveness of polypectomy through enteroscopy is considerably reduced when there has been a previous surgery.6,7 Complications ranging from 0 to 6.8% have been reported in small bowel polypectomy that include bleeding, acute pancreatitis, and perforation. The last two are the most common, at 2.7 and 5%, respectively.6–8 There is little information on the safety and efficacy of polypectomy through enteroscopy in the pediatric population with PJS. One article describes 52 polypectomies in 14 patients utilizing DBE, with no major complications.9 In another study, the authors report on endoscopic polypectomies with DBE in 46 cases, in which the only complication was post-polypectomy bleeding in 4 patients (7.1%), with a directly proportional association between bleeding and polyp size.10
In our study, there was a case of acute pancreatitis after enteroscopy as the only major complication (8.1%), but it was associated with the enteroscopy and not the polypectomy. The incidence of pancreatitis after enteroscopy in the general population can range from 0.311 to 12.5%.12 There are several theories as to the cause and they include pancreatic compression from a loop caused by the enteroscope,13 ischemia secondary to mechanical torsion of the pancreatic vasculature due to excessive rectifications,14 or, the most widely accepted, maintaining the inflated balloon near the Ampulla of Vater, causing inflammation of the papillae and pancreatic reflux.15 Even though most of the studies have reported pancreatitis in anterograde enteroscopies, it has also been seen in retrograde procedures.16 There is little evidence on the safety of enteroscopy in the pediatric population. Nishimura et al. presented a case series of 92 enteroscopies in which there were no major complications related to the procedure.17 Few cases of pancreatitis after enteroscopy have been described in the pediatric population. The only case series reporting pancreatitis in children is that by Yokoyama et al. in which there were 3 cases in 257 enteroscopies performed. All cases of pancreatitis were in the patients that had the anterograde procedure,10 as was the case in our study.
In conclusion, small bowel polypectomy with BAE in pediatric patients with PJS was a safe and efficacious procedure. The complications that presented in our case series were similar to those reported in adult populations. Pancreatitis after enteroscopy in children is a complication that has not been reported often, but then there are few case series conducted on the pediatric population. The greatest limitation of our study was the number of patients. More case series with a larger number of patients are needed to confirm the safety of those procedures in the pediatric population.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Blanco-Velasco G, Hernández-Mondragón OV, Blancas-Valencia JM, Paz-Flores V, Fuentes-Hernández D, Rodríguez-González P, et al. Seguridad y eficacia de la polipectomía en intestino delgado utilizando enteroscopio asistido por balones en pacientes pediátricos con síndrome de Peutz-Jeghers. Revista de Gastroenterología de México. 2018;83:234–237.

