


¿ Introduction
Common bile duct stones (CBD) extraction is usually performed by endoscopic sphincterotomy followed by removal by either a Dormia basket or extraction balloon catheter.1 This procedure has several associated risks, such as hemorrhage, perforation, and probably an increased incidence of ascending cholangitis.2 Some stones due to their size are not amenable to these procedures and mechanical lithotripsy or extracorporeal devices need to be used. Mechanical lithotripsy with an overall success rate of over 80%,3 involves usage of a basket that will be inevitably destroyed increasing costs to the patient and endoscopy unit. Use of extracorporeal wave shock lithotripsy is an alternative; however it is not available widely. Reports about the use of hydrostatic large caliber balloon dilator (≥ 12 mm), introduced by Staritz et al.4 aiding in the extraction of large caliber CBD stones have concluded that is a safe and feasible therapeutic alternative to BES in the management of choledocolitiasis.5 Hydrostatic large caliber balloon dilator (HLCBD) has been associated with lower incidence of complications, such as hemorrhage and perforation6 although it has shown a higher risk of acute pancreatitis compared to biliar endoscopic sphincterotomy (BES).7 Despite this advantage, HLCBD has some limitations due to technical difficulties: the biliary opening is not enlarged as it is in the BES, which makes it harder to remove large stones.8 For the retrieval of large stones some authors suggest the use of HLCBD after BES with a shorter procedure time.9 We present the case of a 25 mm x 30 mm CBD stone that could not be extracted using conventional methods. CBD dilation using HLCBD was performed after endoscopic sphincterotomy in an attempt to avoid mechanical lithotripsy.
¿ Case presentation
A 69 years old hispanic male with a 4 month history of painless jaundice who was diagnosed elsewhere with unresectable cholangiocarcinoma came to our institution looking for a second opinion and further treatment. Physical exam, except for jaundice was unremarkable. Liver function tests reported total bilirubin 6 mg/dL, direct bilirubin 4 mg/dL, alkaline phosphatase 290 U/L, gammaglutamyl transpeptidase (GGT) 180 U/L, aspartate aminotransferase (AST) 175 U/L and alanine aminotransferase (ALT) 160 U/L. Magnetic resonance cholangiography (MRCP) showed significant intra and extrahepatic bile duct dilatation and a hypointense area within the distal common bile duct (CBD) (Figure 1-A) suggesting a stone. An endoscopic retrograde cholangiopancreatography (ERCP) showed a large stone impacted within the distal CBD (Figure 1-B). The stone could not be retrieved using standard extraction procedures (biliary sphincterotomy, retrieval balloon and/or use of Dormia basket) due to size. Even though mechanical lithotripsy is the modality used most commonly, it was omitted to simplify the process of stone extraction and to reduce costs. In order to choose the right size of the balloon to be used, the bile duct and stone diameters were measured during ERCP with the external diameter (13.2 mm) of the distal end of the duodenoscope (Olympus Evis Exera TJF-160VF). The biliar sphincterotomy was extended and the balloon catheter (CRETM wireguided balloon dilator 15 - 18 mm, Boston Scientific) was passed over a guidewire and positioned at the biliary orifice. Then, the balloon was gradually filled up to 15 mm with water and diluted contrast medium by using an inflation device (ALLIANCE II, Boston Scientific). The fully expanded balloon was maintained in position for 45 seconds after it was collapsed and removed. A Dormia basket was then used to remove the stone. A 25 mm x 30 mm CBD stone was extracted uneventfully except for minor oozing that stopped spontaneously (Figure 2). After the procedure the patient was hospitalized for observation with no clinical evidence of bleeding or pancreatitis; hemoglobin and serum amylase levels were measured 18 hours after the procedure within normal limits. The patient was discharged without complications. One month after the endoscopic intervention no complications were observed.
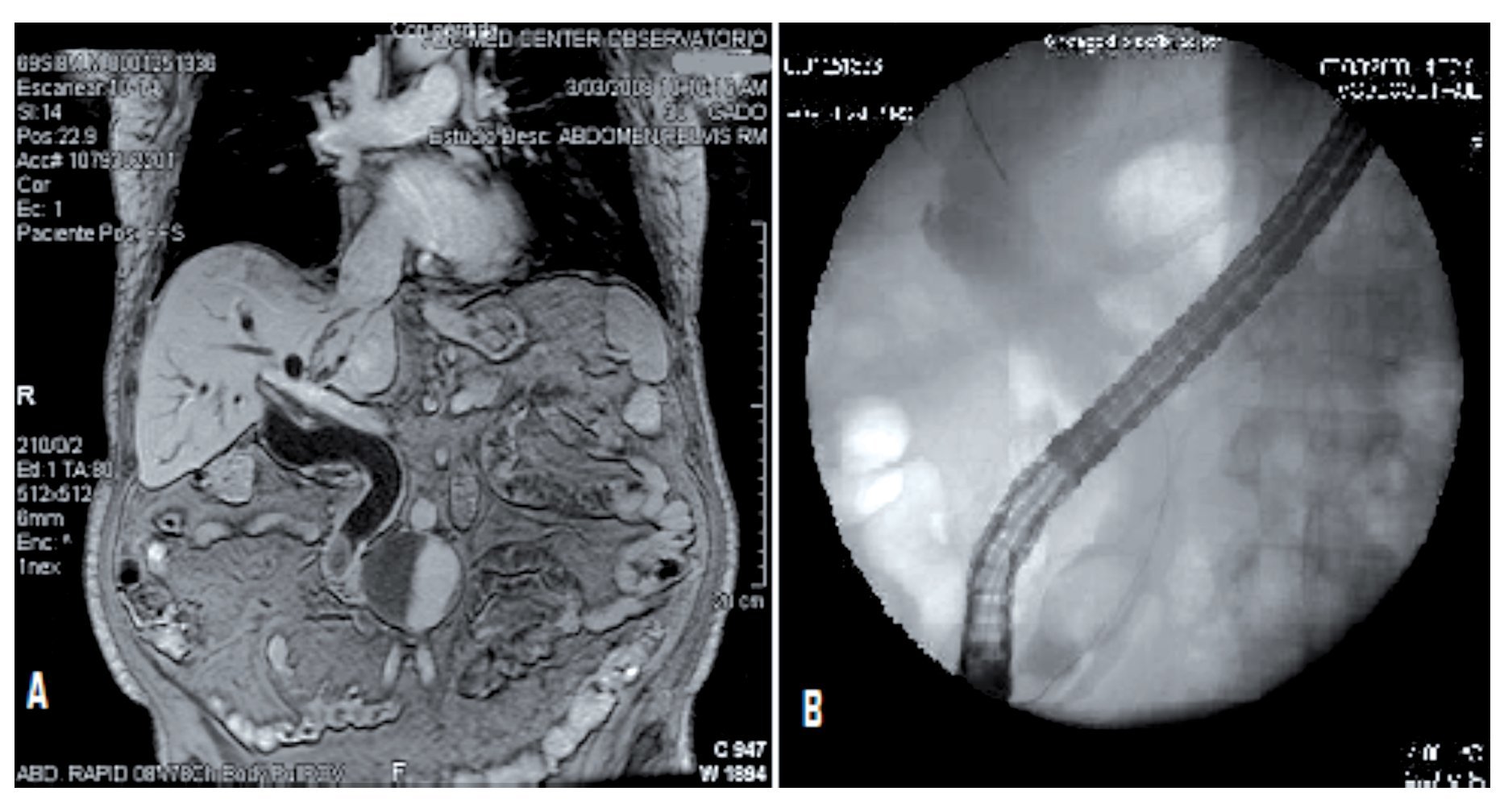
¿ Figure 1. A MRCP image; B ERCP fluoroscopic image showing a large stone impacted on distal CBD.
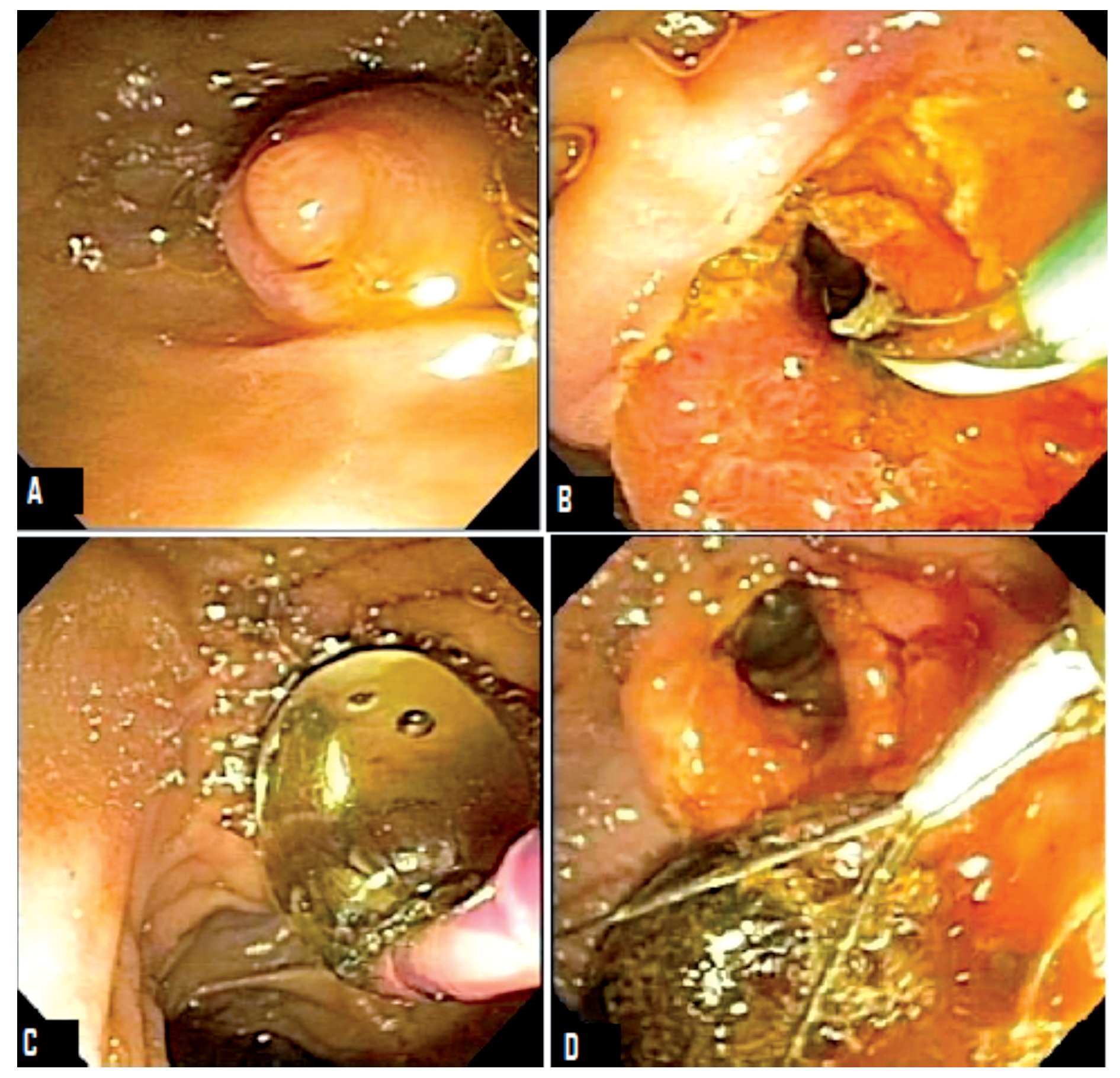
¿ Figure 2. ERCP images: A) Prominent papilla, B) Large biliary sphincterotomy, C) Large caliber balloon dilation, D) CBD stone extracted with Dormia basket.
¿ Discussion
We present the case of a large biliary stone that could not be treated with conventional endoscopic methods; HLCBD after BES was performed with successful removal of the stone.
Approximately 10% of biliary stones are difficult to extract during ERCP using conventional stone extraction techniques due to large stone diameter 9 as in the present case. BES plus stone withdrawal using biliary balloon extraction and/or a Dormia Basket is the most commonly used technique for the removal of bile-duct stones,10 however is not a good method if the stones are too large. Endoscopic balloon dilation alone as an alternative method, does not enlarge the sphincter of Oddi to the same extent as BES, so large stone removal is difficult and mechanical lithotripsy is required more often than with BES.11 Mechanical lithotripsy is an alternative for removal of large stones, however this procedure is time consuming and approximately 30% of the cases are not resolved during the first attempt, needing to undergo a second procedure.12 It should be noted that during mechanical lithotripsy, a Dormia basket is destroyed, increasing costs of the procedure to the patient and the endoscopy unit. Another option is the use of extracorporeal wave shock lithotripsy but unfortunately this is not available widely. Lastly, surgical removal, although safe and effective it carries a higher morbidity, risks of general anesthesia and in some cases, prolonged hospital stay.
One of the first descriptions of BES plus HLCBD for large CBD stone extraction was reported by Ersoz et al.9 Hydrostatic balloons with a diameter range between 12-20 mm were used in cases in which CBD stones that could not be removed due to tapering of distal CBD or the presence of large, squared, and barrel shaped stones. They reported an 83% success rate in the first session, 10% more resolved during a second procedure. Mechanical lithotripsy was required in 7% of the patients. Complications occurred in 15.5% of patients and mild pancreatitis developed in 2 patients (3.4%). Recently, multiple published series have shown that the overall first session success rates of stone removal with HLCBD following BES ranged from 80% to 100%.13,14,15 The overall mortality rate of this procedure is 0.25%, related to severe bleeding and perforation.16 Perforation of the biliary tract seems to be related to a deficient balloon insertion technique. It is recommended to always verify the correct position of the balloon over a wire by fluoroscopic image before inflating it, particularly in patients with low cystic duct insertion, or dilated cystic duct, since these variants increase the risk of misplacing the balloon within the cystic duct.13 The presence of hemorrhage after HLCBD plus BES is similar to the reported in BES alone. It is thought that the balloon tamponade of the sphincterotomy site achieved with large balloons might play a role in decreasing the incidence of bleeding.15 The long term complications related to this technique are difficult to determine at this time because the majority of cases series reported in the literature are conformed wiht a small number of patients. However, a large-scale study is required to clarify long term complications and outcomes related to this technique.17
¿ Conclusion
Performing HLCBD after BES might be a relatively safe and efficient procedure in cases of large biliary tract stones that are difficult to manage with conventional endoscopic methods. It appears to be cheaper and easier to perform compared to mechanical lithotripsy. The exact role in managing difficult and large bile duct stone needs further prospective studies with larger number of patients and should be performed by experienced endoscopists in high volume referral centers
Correspondence: Edgar Vázquez Ballesteros.
MD. Observatorio, Sur 136 N° 116, Colonia Las Américas, México D. F., México.
Teléfono y Fax: 5272-49-19.
Correo electrónico: edvazball@yahoo.com.mx
Recibido el 7 de enero de 2010;
aceptado el 23 de abril de 2010.

