





¿ Introduction
Colorectal polyps (CP) are classified as either nonneoplastic or neoplastic. Non-neoplastic polyps include hyperplastic, juvenile and inflammatory types. Neoplastic polyps refer to carcinoid tumors, polypoid carcinomas, non-epithelial tumors and adenomas, which can also be divided by the histological pattern as tubular, tubulo-villous and villous. The histological progression of an adenoma to carcinoma may take 7 to 12 years and this is one of most important rationales for recommending screening for adenomas so they can be removed for preventing colorectal cancer (CRC).1
Several variables have been considered as risk factors for colonic neoplasia such as age, low dietary fiber intake, high saturated fat intake, sedentary behavior, tobacco use, alcohol use, family history of colorectal cancer (FHCRC) and an elevated body mass index (BMI).2,3 However, some patients may not have any risk factors documented.4
In the UK, a study using flexible sigmoidoscopy (FSIG) found a prevalence of 25% for distal polyps, 12% for advance adenomas and 0.3% for carcinomas.5 In the United States of America, the prevalence of colonic adenomas is estimated to be approximately 37% by age 50 and 65% by age 70.6,7 The Hispanic population in the USA appears to have the same polyp prevalence as other ethnic groups. For Hispanic men and women, colorectal cancer is the second and third cause of death, respectively.8,9 In addition, the adherence rate for CRC screening in the USA is lower among the Hispanic population as compared to Caucasians.10
In Mexico, few studies addressing the prevalence of CP have been published. The existing studies were done in patients with suspected colorectal lesions, in patients with FHCRC and in autopsy series; the range of the prevalence of polyps reported in these studies was from 1.5% to 30%.11-13 In 1990, the Mexico General Hospital conducted a study of 1 352 patients who underwent sigmoidoscopy and found 13 patients with CP.11 Another retrospective study using colonoscopy in 428 patients older than 50 years with and without symptoms, found an adenoma prevalence of 19.3%.14
In the USA, the risk of CRC in the general population is 5% (the CRC rate is 23 to 32 patients per 100 000 persons). The standardized mortality rate for CRC in Mexico reached 2.8 persons per 100 000 inhabitants.15,16 The past decade in Mexico has observed an increase of approximately 100% in the CRC prevalence reported, with the highest prevalence in Northern Mexico, a geographic area with high industrial and socioeconomic development. Monterrey is the second largest city in the country and has one of the highest income rate reported in Mexico.
Currently, different methods for colorectal cancer screening are used; these include the fecal occult blood test, fecal DNA test, FSIG, double contrast barium enema, colonoscopy and more recently other radiological studies such as the computed tomographic (virtual) colonography. To our knowledge, there have been no studies to date in Mexico among asymptomatic patients using FSIG as a screening method in the detection of CP and/ or adenomas. The objective of this research is to determine the prevalence and risk factors for colorectal polyps detected during flexible sigmoidoscopy (FSIG) in asymptomatic patients.
¿ Patients and methods
From 1995 to 2008, we performed FSIG in asymptomatic adult patients referred to our institution for a complete medical evaluation (check-up) as a screening method to detect CP. We analyzed the clinical history, laboratory and pathology results and FSIG reports. Also, in all patients we obtained information on the following risk factors: age, gender, body mass index (BMI), total cholesterol, HDL and LDL cholesterol, triglycerides, tobacco (present or past history) and alcohol use (2 to 3 times per week) and a family history of CRC, with only first degree relatives with colon cancer considered as a positive factor.
Inclusion criteria featured patients living in the northeast region of Mexico for the past five years and being asymptomatic for colorectal diseases at the time of FSIG. We excluded patients with a past history of colonic tumors or colorectal surgery. Patients were prescribed one bisacodyl tablet the night before and a commercial phosphate enema the day of the FSIG. We used a FS4V Pentax endoscope for the procedure. During FSIG, a 60 cm depth insertion was intended. The exam was interrupted if fecal material made it impossible to review the colonic mucosa above the site or patients reported severe discomfort or pain. Ninety percent of FSIG were performed by two gastroenterologists participating in the study (JAG, HMG). Any procedure-related complications were recorded. FSIG findings were entered in a data base designed to meet the purposes of the current study.
¿ Statistical analysis
The computer program SPSS software version 13.0 (SPSS Inc, Chicago Il) was used for statistical analysis. In descriptive statistics the means, ranges and standard deviations are given for continuous variables. Percent distributions are given for categorical variables. The Student´s t-Test, Chi-square or Fisher´s exact test were used for comparisons. Multiple logistic regression analysis was used to evaluate risk factors for CP and adenomas, and odds ratios and 95% confidence intervals are reported. The statistical significance level was set at a p-value of <0.05.
¿ Results
We evaluated 1 073 patients and 946 were included in the study. We excluded 127 patients; 107 who were not residents of the northeast region of Mexico, 16 with previous colon surgery and 4 with a history of CP. The mean age was 48.8 years (range 21-91). We evaluated 794 male and 152 female patients. Alcohol or tobacco use was reported by 41% and 14% of the study subjects, respectively. Two percent of our population had a positive FHCRC. The median level of the total serum cholesterol for patients with and without polyps was 211.4 mg/dL ± 36 mg/dL and 206.3 ± 39 mg/dL (p = 0.013); for triglycerides 175 ± 101 mg/dL and 146 ± 87 mg/ dL (p = 0.027); for HDL cholesterol, 43.8 ± 33 mg/dL and 46.7 ± 9 mg/dL; for LDL cholesterol 140 ± 44 mg /dL and 137 + 34 mg/dL, respectively.
Univariate analyses for CP showed significant associations with positive FHCRC, triglycerides > 130 mg/dL, age > 50 years and BMI > 25, but in the multivariate analysis, only BMI > 25 and positive FHCRC reached statistical significance, as shown in Table 1. The univariate analysis of colonic adenomas was significant for positive FHCRC, age > 50 years and BMI > 25. However, in the multivariate analysis, only BMI > 25 and positive FHCRC were found significant, as shown in Table 2.
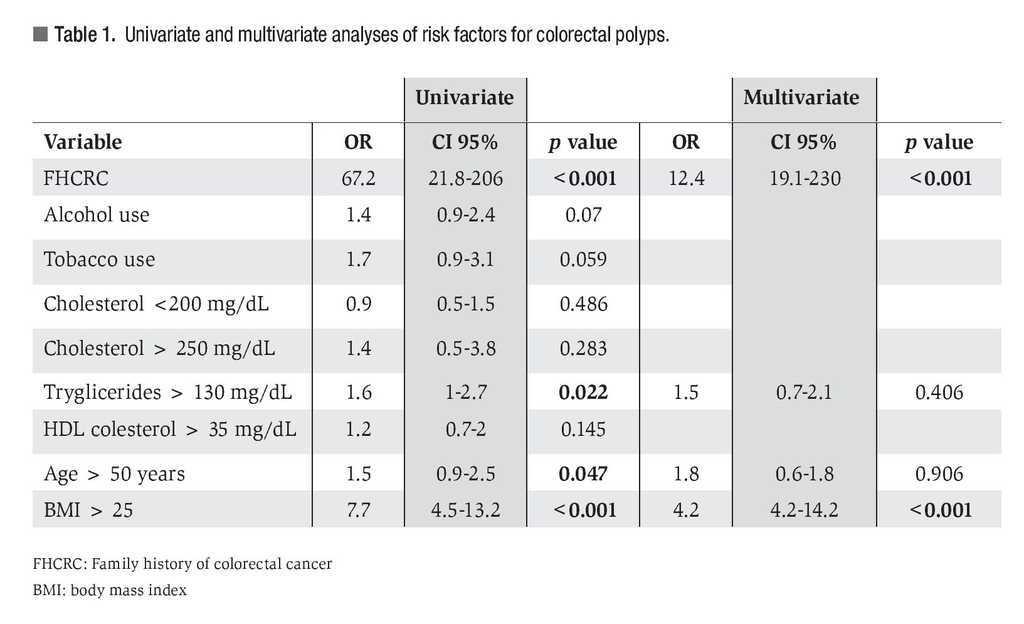
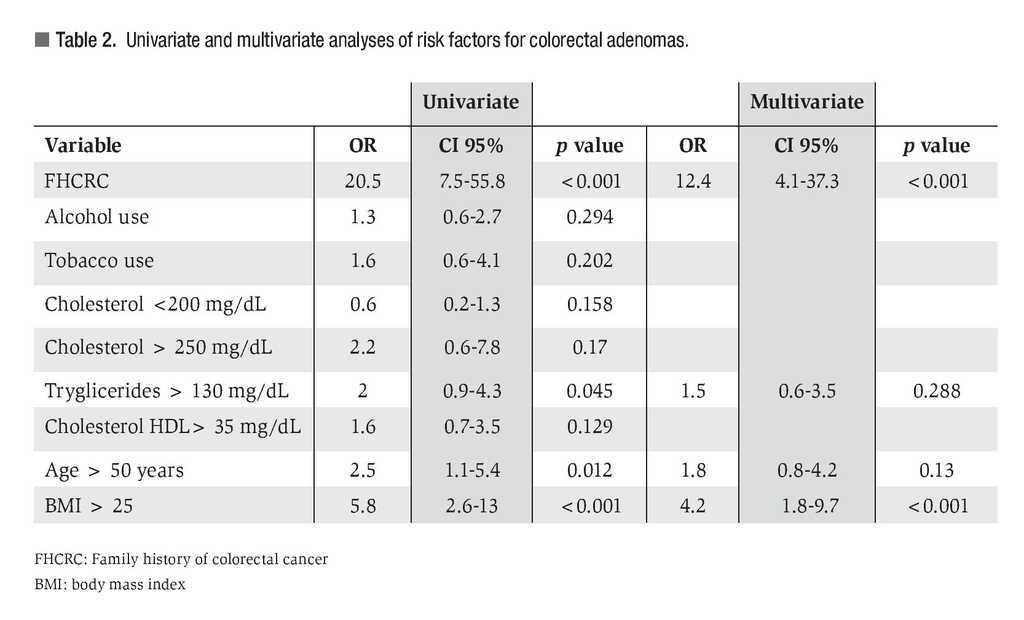
The variables gender, alcohol use, tobacco use, total cholesterol, HDL and LDL cholesterol were not significant risk factors for CP or adenomas.
The FSIG mean depth of insertion was 46 cm (for males, the mean depth was 45 cm (SD + 9.3) and for females, the mean depth was 39 cm (SD + 8.5). Total FSIG insertion (60 cm) was reached in 20% of the patients. No difference was found between patients with and without polyps with regards to the depth of insertion. Five patients developed vagal symptoms during FSIG with immediate recovery and another patient reported anal irritation within 24 hours after the study. No colonic perforations occurred.
Of the 946 patients, 72 patients had polyps (7.6%), with 65 polyps (90.3%) occurring in males and 7 polyps occurring in female (9.7%). Of the 72 polyps, 29 were adenomas (3%), 30 were hyperplastic (3.2%) and 13 were inflammatory (1.4%). We found 24 adenomas <1 cm in size and 5 adenomas > 1 cm. The adenoma histological pattern was tubular in 27 and tubule-villous in 2 patients. Most of the polyps (70%) were diagnosed at > 20 cm from the anal verge. The mean polyp size was 5.7 mm (range 1 to 15 mm). One rectal carcinoid tumor (5 mm) and two polyps higher than 2 cm were diagnosed and successfully treated with endoscopic resection. The polyp distribution by age group is shown in Table 3.

In 357 patients older than 50 years, we found 32 CP (8.9%) and 17 adenomas (4.8%). In all patients with colonic adenomas, a total colonoscopy was recommended.
¿ Discussion
As part of a routine annual medical evaluation, 946 patients who were residents of northeast Mexico were submitted to a first FSIG procedure as a screening method to detect CP. Their mean age was 48.8 years and most of them (84%) were men. Among women, 4.6 % had CP and 2.6% had adenomas.
The adenoma prevalence in patients younger than 40 years, 40 to 50 years and older than 50 years was 1%, 2.2% and 4.8% of patients, respectively.
Recently, a study on alcohol consumption showed that drinking five or more drinks per week was not associated with the risk of developing CP.17 In our study, we considered a positive history of alcohol use when the patient drink alcohol at least 2 to 3 times per week and a positive history of tobacco use as having smoked in the past 5 years or currently smoking at the time of study entry. Neither alcohol nor tobacco use was an independent risk factor for CP or adenomas; these data differ from the results of a recent meta-analysis report.18 Univariate analysis showed that age > 50 years, triglycerides > 130 mg/dL, positive FHCRC and BMI > 25 were significant for CP and adenomas and in the multivariate analysis only the positive FHCRC (OR 12.4) and BMI > 25 (OR 4.2) were statistically significant. Several studies have found that FHCRC is a risk factor for CP and adenomas.19,20
Body fat distribution, the timing of becoming overweight or obese and racial or ethnic differences could all be considered as risk factors for CP and adenomas. BMI has been associated with the development of CP and adenomas. The biologic mechanisms include the release of growth factors by the adipose tissue, insulin resistance, and changes in insulin-like growth factors in overweight or obesity that increase the risk of CP and the development of adenomas.21-23 The difference in several variables that did not reached statistical significance in the multivariate analysis such as age could be related to a statistical beta error.
In our study, we intended to have a representative cohort of the population of northeast Mexico. When analyzing the occurrence of CP by patient's BMI status, we found 20 adenomas (7.3%) among 272 patients with BMI > 25, 12 adenomas (6.2%) among 193 patients with BMI 25-30, and 8 adenomas (10.2%) among 79 patients with BMI > 30. Of the 674 patients with BMI > 25, we found 20 polyps (2.9%) and only 3 adenomas (0.04%). Thus, older patients with higher BMI have an increased risk for adenomas while patients with normal body weight have a very low prevalence of CP and adenomas. The prevalence of CP and adenomas in patients > 50 years was 8.9% and 4.8%, respectively. These estimates are higher than those from the Mexican autopsy study (0.9%), but lower than the
19.3% CP prevalence in patients > 50 years that was reported by Lascurain.11,14
Most polyps found in this study were less than 5 mm in size. These polyps are considered as diminutive polyps, which have a very low risk for cancer (0.02%), but may be relevant as a marker for synchronous proximal colonic adenomas.24 The FSIG depths of insertion for men and women were 45 cm and 39 cm respectively, similar to previous reports.25,26 No statistical significance was found when comparing FSIG depths of insertion in patients with and without polyps. A large study of FSIG as a screening method for adenomas reported a very high acceptance for FSIG and a 23% prevalence of CP using FSIG.27 One major inconvenience of screening polyps by FSIG is the limited colonic examination that results in a risk of undetected CP of almost 30%. Recently, a high frequency of proximal CP in different ethnic populations has been reported.7,28,29 In our study, the 4.8% CP using FSIG may underestimate the true prevalence. A multicenter prospective trial about risk factors for CP and adenomas in asymptomatic patients using colonoscopy in Mexico is thus needed.
In conclusion, our study found that patients younger than 40 years and women rarely have adenomas. The BMI > 25 and positive FHCRC are independent risk factors for the occurrence of CP and adenomas. The adenoma prevalence in patients older than 50 years is lower than the prevalence reported in developed countries.
Correspondence author: Dr. José Alberto González.
Facultad de Medicina y Centro Regional para el Estudio de Enfermedades Digestivas (CREED).
Hospital Universitario Dr. José Eleuterio González. UANL. Monterrey, NL. México.
E-mail:joseagonz@yahoo.com

