




Gastrointestinal perforations are one of the most frequent surgical emergencies. They can be produced by endoluminal disease, foreign bodies, or by an iatrogenic event. Even though surgery continues to be the standard treatment of gastrointestinal perforations, the increase in both diagnostic and therapeutic endoscopic procedures has led to the development of new systems for attempting endoscopic closure of small perforations. The OVESCO system is one of the most widely used and consists of a preinstalled clip of biocompatible material that brings together, compresses, and closes the edges of perforations measuring up to 3cm.1
We describe herein a case, in which, after attempting the closure of an iatrogenic duodenal perforation produced during a diagnostic endoscopic ultrasound (EUS), utilizing the OVESCO system, an endoscopic instrument became trapped.
A 73-year-old woman with an unremarkable past medical history, underwent EUS due to suspicion of a lesion in the head of the pancreas. During the procedure, the linear echoendoscope was introduced into the second part of the duodenum and in the course of its withdrawal, a circular perforation, measuring approximately 1.5cm, was detected at the lateral surface of the second part of the duodenum. Given that finding, a conventional endoscope was then introduced, and after CO2 insufflation, an OVESCO device was placed to close the perforation, trapping the endoscopic forceps inside it, making it impossible to be moved or removed.
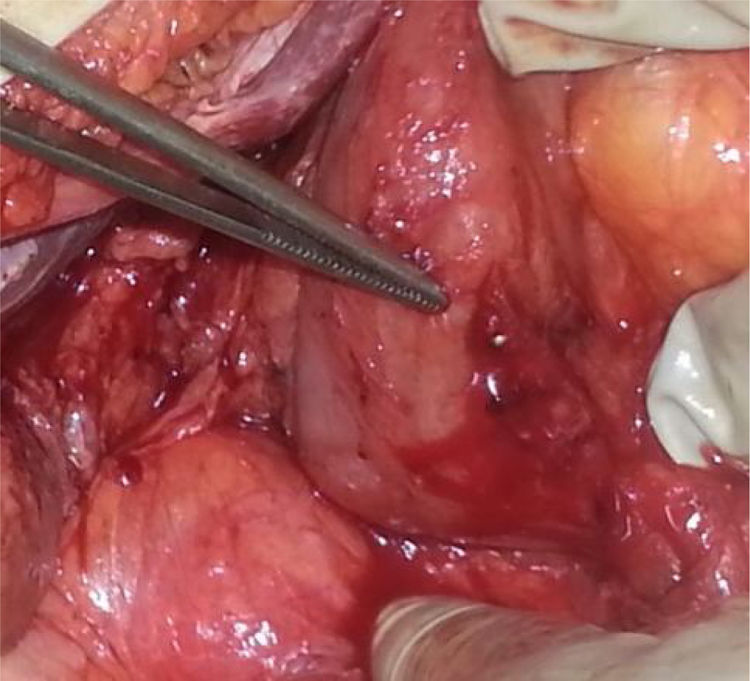
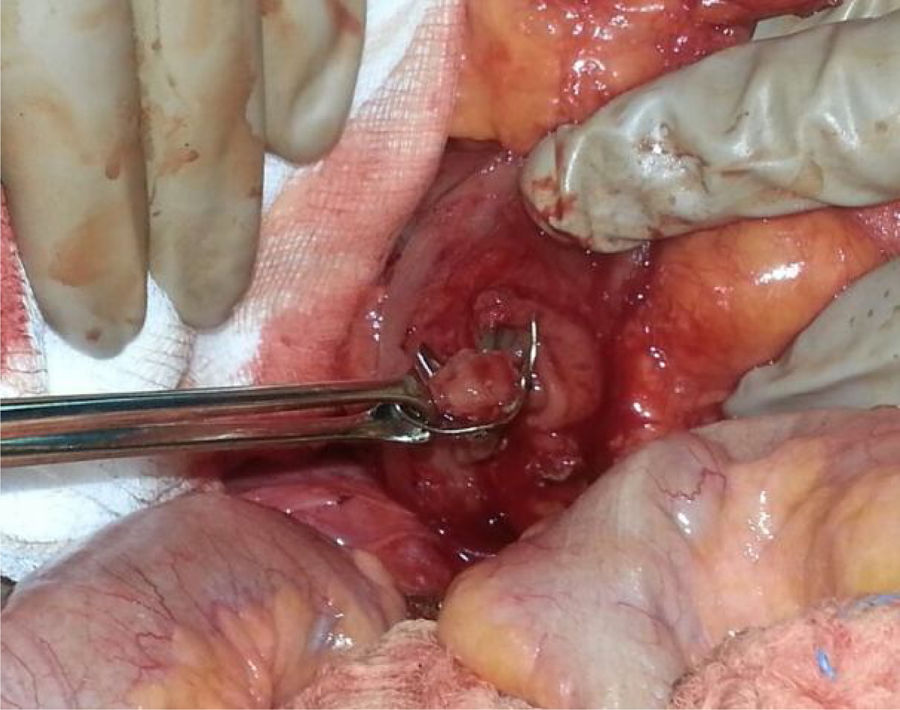
The patient underwent emergency surgery. An approximately 2cm perforation in the posterior wall of the duodenum was partially occluded by the OVESCO, with an endoscopic forceps trapped in the occlusion and coming out through the duodenal wall (Fig. 1). A wide Kocher maneuver was performed, along with duodenotomy to extract the forceps (Fig. 2), and single-layer closure of the perforation with omentoplasty was carried out. A feeding jejunostomy was placed. The patient progressed favorably, resuming oral diet with good tolerance, and was released on postoperative day 14.
Complications associated with EUS vary from 0.04 to 0.6%, and include infections, bleeding, pancreatitis, perforations, and sedation-related events. In the hands of an expert operator, the prevalence of complications is similar to that of conventional upper gastrointestinal endoscopy (0.1-0.5%).2 The incidence of gastrointestinal perforation during EUS varies from 0 to 0.4%, and is the most serious complication, with high morbidity and mortality (16–18%).3,4 Esophageal perforation is the most frequent perforation associated with EUS, performed with a radial echoendoscope. However, the duodenum is the most susceptible site of perforation with a linear echoendoscope, especially in areas of angulation, stricture, and diverticula. Known risk factors for duodenal perforation in those types of procedures include a lack of training of the endoscopist, the presence of duodenal diverticula, deficient insufflation of the lumen, and sphincterotomy.2
The important increase in the performance of endoscopic procedures has led to the development of different devices to avoid complications without the need for surgery. The first endoscopic clips were introduced in 1975 by Hayashi, for the purpose of resolving gastrointestinal bleeds.5,6 Since then, they have been used for nonsurgical closure of the gastrointestinal wall involving fistulas, anastomotic wound dehiscence, and spontaneous, as well as iatrogenic, perforations.6 New systems, such as the OVESCO, have recently been developed for the nonsurgical management of fistulas, leaks, gastrointestinal perforations, and for controlling gastrointestinal bleeding.7 Their use has also been extended to include the treatment of tissue defects in the gastrointestinal tract. The OVESCO utilizes clips that are preinstalled on a plastic cap at the distal end of the endoscope. Once the perforation is located, the edges of the perforation are placed inside the cap, utilizing aspiration or endoscopic approximation instruments, such as a double grasping forceps or anchor forceps. The clip is released, bringing the edges of the perforation together and compressing them.1 In our case, the grasper forceps became trapped by the clip, upon closing the perforation. The OVESCO system has a complication rate of approximately 2%7 and a risk for severe complications of 0.6%.8 Complications are not related to any specific pattern.9 Cases of inappropriate device placement, esophageal or intestinal wall laceration, perforation, enteral stricture, peritonitis, accidental neighboring organ entrapment, bleeding, and other rarer events have been described.9 Selecting the adequate clip, awareness of its type and size, appropriate use of the approximation accessories, precise placement, and the experience and skill of the endoscopist are all factors that will aid in preventing complications, such as the one described herein.9
The complication in our case involved the placement of the second clip by the endoscopist, and the aspects of location in the duodenum and inexperience, combined with other factors stated above, could have helped bring it about. Wedi et al. reported the same complication in the distal esophagus and its costly endoscopic resolution.10 Surgical resolution was required in our patient. At present, ours is the second case describing this type of complication.10 Its communication is important, so that opportune precautions during said procedures are always taken.
As reported in the current literature, devices like the OVESCO system can be a valid alternative in older patients that have perforations and associated comorbidities, as long as the perforations are small (under 2cm), the device is placed by a trained endoscopist, and surgery is available, should it be required. Despite the development of those devices, the gold standard in the treatment of gastrointestinal perforations, whether spontaneous or iatrogenic, continues to be surgery.
Ethical considerationsPermission was requested of the patient to use the images but authorization by our center’s ethics committee was not required, given that no experimental drug or device was utilized. The patient’s anonymity was preserved at all times, the article contains no personal information that could identify the patient.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Rahy-Martín AC, Jiménez-Díaz L, Rodríguez-Pérez RM, Acosta-Mérida MA, Marchena-Gómez J. Una complicación del cierre endoscópico de perforación duodenal con sistema OVESCO. Rev Gastroenterol Méx. 2022;87:268–270.

