

The SARS-CoV-2 virus that causes the COVID-19 disease is transmitted through the inhalation of droplets or aerosols and inoculation via the oronasal or ocular routes, transforming the management of swallowing disorders into a challenge for healthcare teams, given their proximity to the aerodigestive tract and the high probability of aerosol generation during patient evaluation and treatment.
AimTo provide essential guidance for Latin American multidisciplinary teams, regarding the evaluation and treatment of oropharyngeal and esophageal dysphagia, at the different levels of healthcare. The position statement was formulated for the purpose of maintaining medical service continuity, in the context of a pandemic, and minimizing the propagation and infection risks of the virus.
MethodsThirteen experts in swallowing disorders were summoned by the Latin American Dysphagia Society to formulate a series of clinical suggestions, based on available evidence and clinical experience, for the management of dysphagia, taking the characteristics of Latin American healthcare systems into account.
ResultsThe position statement of the Latin American Dysphagia Society provides a series of clinical suggestions directed at the multidisciplinary teams that manage patients with oropharyngeal and esophageal dysphagia. It presents guidelines for evaluation and treatment in different contexts, from hospitalization to home care.
ConclusionsThe present statement should be analyzed by each team or healthcare professional, to reduce the risk for COVID-19 infection and achieve the best therapeutic results, while at the same time, being mindful of the reality of each Latin American country.
El virus SARS-CoV-2, que causa la enfermedad COVID-19, se transmite por inhalación de pequeñas gotas o aerosoles e inoculación por vía oronasal u ocular, lo cual hace del manejo de la deglución para los equipos de salud un desafío, dada su proximidad al tracto aerodigestivo y la alta probabilidad de generar aerosol durante la evaluación y tratamiento de los pacientes.
ObjetivoBrindar orientación esencial a los equipos de salud multidisciplinarios de Latinoamérica para la evaluación y tratamiento de la disfagia orofaríngea y esofágica en los diferentes niveles de atención en salud. Este posicionamiento fue realizado con el propósito de mantener la continuidad de los servicios médicos en el contexto de una pandemia y minimizar los riesgos de propagación y contagio del virus.
MétodosCon base en la evidencia disponible y la experiencia clínica alcanzada hasta la fecha, 13 expertos en deglución convocados por la Sociedad Latinoamericana de Disfagia formularon una serie de sugerencias clínicas para el manejo de la disfagia, considerando las características de los sistemas de salud latinoamericanos.
ResultadosEl posicionamiento de la Sociedad Latinoamericana de Disfagia brinda a los equipos multidisciplinarios una serie de sugerencias clínicas para el manejo de personas con disfagia orofaríngea y esofágica y ofrece lineamientos para su evaluación y tratamiento en diferentes contextos, desde la hospitalización hasta la atención domiciliaria.
ConclusionesEste posicionamiento debe ser analizado por cada equipo o profesional de la salud, para reducir el riesgo de contagio por COVID-19 y lograr los mejores resultados terapéuticos, considerando siempre la realidad de cada país latinoamericano.
The World Health Organization declared the COVID-19 disease a global pandemic in March of 2020. In Latin America, as of mid-June of 2021, a total of 35,672,198 positive COVID-19 cases have been confirmed, accounting for 20% of the infected population worldwide. Unfortunately, 1,228,677 of those patients have died1. The disease produced by SARS-CoV-2 is highly transmissible, requiring clinicians to modify their practices and protocols for safety reasons. COVID-19 disease impacts the functioning of the respiratory system and is a risk factor for developing dysphagia in certain groups, such as the elderly, patients with pre-existing lung conditions, and patients with other comorbidities2. Conditions are exacerbated in patients that require prolonged periods of ventilation (more than 72 h), increasing the risk of dysphagia after extubation3. Therefore, it is not surprising that the incidence of dysphagia in COVID-19 patients can be as high as 80% in persons that required ventilatory support, and close to 30% in those that did not4,5.
Considering the abovementioned data, all healthcare professionals (HCPs) that are part of the dysphagia treatment team must take all the necessary measures to minimize the risk of contagion, recognizing that the treatment of dysphagia includes procedures that can lead to the production of droplets and aerosols, as well as to contact with the virus6–8. Therefore, the timing of the evaluation of dysphagia and the indication of treatment will most likely differ from the norm6, especially regarding the implementation of different procedures, in an effort to maintain the continuity of care and optimize patient turnover at the different hospitals and health facilities9.
The present position statement is a proposal for promoting the safety of the multidisciplinary team treating oropharyngeal and esophageal dysphagia, in the context of the COVID-19 pandemic. The aims of this statement are: (1) to provide essential guidance related to the diagnosis and rehabilitation of oropharyngeal and esophageal dysphagia and (2) to provide a guide for the multidisciplinary team working with COVID-19 patients that present with different clinical complexities of dysphagia (i.e., critical care patients, hospitalized patients, outpatients, patients receiving home care, and patients receiving telehealth services), to help reduce the risk of transmission of SARS-CoV-2.
The Latin American Dysphagia Society (LADS) formulated this position statement, with respect to clinical management, in the context of a crisis that is still present in several countries in the region, based on currently available information. Because the information is continuously developing, the statements contained herein are not evidence-based clinical practice guidelines and may require future evaluation and revision. Finally, the statements must be put into context, based on the characteristics of the health system of each country, access to resources, and the prevalence of COVID-19.q
MethodsThe board of directors of the LADS summoned 13 experts to participate in formulating the position statement. The participants were from Argentina, Brazil, Chile, Colombia, Mexico, Paraguay, and Peru, the countries that, as of March 2021, formed part of the dysphagia society. Each expert met the following criteria: (a) at least 10 years of experience in the treatment of dysphagia, (b) postgraduate training in dysphagia, and (c) currently working at a clinic, hospital, or academic institution. The multidisciplinary approach was favored by the participation of speech language pathologists, phoniatricians, gastroenterologists, and otolaryngologists.
The methodology previously described in similar documents was used6,20 and the statements were supported by recommendations, consensuses, and evidence available at the time, taking care to adapt them to the different scenarios that exist in Latin America. At a first meeting, and in accordance with the area of expertise of each participant, the sections were assigned for the bibliographic search, the summarization of the evidence collected, and the drafting of the recommendations for the first round of voting. The bibliography was available to all the participants. The recommendations were sent to the participants by means of an electronic survey system. The response options for each recommendation were: “I agree”, “I disagree”, and “text modification”, and the round of voting was carried out on October 19, 2020.
The participants had a final meeting on a virtual platform on October 21, 2020, to know the results of the survey and vote again, if necessary. Agreement of 80% was required for a recommendation to be established. Recommendations that did not reach 80% agreement were put to a vote, after making the suggested text modifications, and recommendations that had 80% approval were automatically accepted. Each section provides a summary of the evidence and the subsequent recommendations. No system was employed to classify the quality of the evidence. The final version of the document was reviewed and approved by all the participants.
Personal protection and prevention measuresThe SARS-CoV-2 virus is transmitted by inhalation of drops or aerosols21, or by contact and subsequent inoculation via the oronasal or ocular routes. It is highly transmissible, a situation that implies strict control, with respect to prevention measures and personal protection for the health team and towards patients22, which includes correctly putting on and taking off personal protection equipment (PPE)23. Both clinical and instrumental swallowing evaluations are considered aerosol-generating procedures (AGPs), because they involve interventions for assessing cough, phonation, the functioning of sphincter mechanisms, and pressures at the aerodigestive crossroads, for the protection of the airway6–8. Such interventions tend to involve an exposure time of more than fifteen min and a distance of less than 1.80 m, increasing the risk of transmission24.
For hospital wards of patients with suspected or confirmed COVID-19, maintaining negative pressure, with a minimum of 6–12 air exchanges per hour, is recommended, and if that is not possible, they should maintain a ventilation rate of at least 160 L/s25. The doors of the rooms should be kept closed the majority of the time. The air in those rooms must be exhausted directly to the outside or filtered through a high-efficiency particulate air (HEPA) filter, before recirculation25.
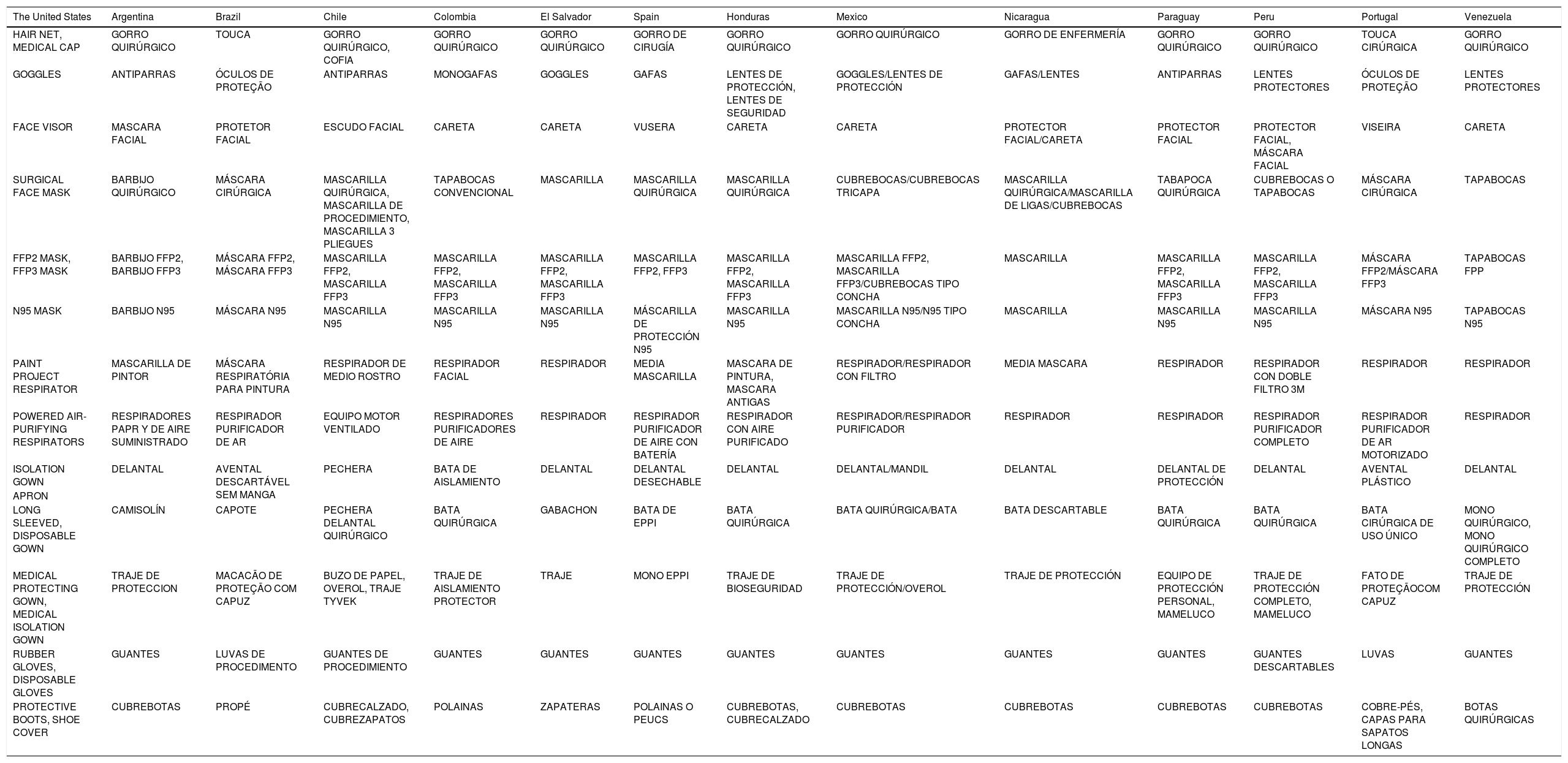
The PPE for AGP practices includes an N95 mask, covered by a disposable surgical mask, eye protection, a cap, disposable gloves, and a gown. An acrylic mask and shoe covers are optional. Because PPE goes by different names in each Latin American country, Table 1 shows a list of the corresponding synonyms. Whether Levels 1, 2, or 3 of PPE should be used, depends on the viral load status of the patient, local and institutional regulations, and the epidemiological situation of the specific region.
Table of synonyms for personal protective equipment.
| The United States | Argentina | Brazil | Chile | Colombia | El Salvador | Spain | Honduras | Mexico | Nicaragua | Paraguay | Peru | Portugal | Venezuela |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HAIR NET, MEDICAL CAP | GORRO QUIRÚRGICO | TOUCA | GORRO QUIRÚRGICO, COFIA | GORRO QUIRÚRGICO | GORRO QUIRÚRGICO | GORRO DE CIRUGÍA | GORRO QUIRÚRGICO | GORRO QUIRÚRGICO | GORRO DE ENFERMERÍA | GORRO QUIRÚRGICO | GORRO QUIRÚRGICO | TOUCA CIRÚRGICA | GORRO QUIRÚRGICO |
| GOGGLES | ANTIPARRAS | ÓCULOS DE PROTEÇÃO | ANTIPARRAS | MONOGAFAS | GOGGLES | GAFAS | LENTES DE PROTECCIÓN, LENTES DE SEGURIDAD | GOGGLES/LENTES DE PROTECCIÓN | GAFAS/LENTES | ANTIPARRAS | LENTES PROTECTORES | ÓCULOS DE PROTEÇÃO | LENTES PROTECTORES |
| FACE VISOR | MASCARA FACIAL | PROTETOR FACIAL | ESCUDO FACIAL | CARETA | CARETA | VUSERA | CARETA | CARETA | PROTECTOR FACIAL/CARETA | PROTECTOR FACIAL | PROTECTOR FACIAL, MÁSCARA FACIAL | VISEIRA | CARETA |
| SURGICAL FACE MASK | BARBIJO QUIRÚRGICO | MÁSCARA CIRÚRGICA | MASCARILLA QUIRÚRGICA, MASCARILLA DE PROCEDIMIENTO, MASCARILLA 3 PLIEGUES | TAPABOCAS CONVENCIONAL | MASCARILLA | MASCARILLA QUIRÚRGICA | MASCARILLA QUIRÚRGICA | CUBREBOCAS/CUBREBOCAS TRICAPA | MASCARILLA QUIRÚRGICA/MASCARILLA DE LIGAS/CUBREBOCAS | TABAPOCA QUIRÚRGICA | CUBREBOCAS O TAPABOCAS | MÁSCARA CIRÚRGICA | TAPABOCAS |
| FFP2 MASK, FFP3 MASK | BARBIJO FFP2, BARBIJO FFP3 | MÁSCARA FFP2, MÁSCARA FFP3 | MASCARILLA FFP2, MASCARILLA FFP3 | MASCARILLA FFP2, MASCARILLA FFP3 | MASCARILLA FFP2, MASCARILLA FFP3 | MASCARILLA FFP2, FFP3 | MASCARILLA FFP2, MASCARILLA FFP3 | MASCARILLA FFP2, MASCARILLA FFP3/CUBREBOCAS TIPO CONCHA | MASCARILLA | MASCARILLA FFP2, MASCARILLA FFP3 | MASCARILLA FFP2, MASCARILLA FFP3 | MÁSCARA FFP2/MÁSCARA FFP3 | TAPABOCAS FPP |
| N95 MASK | BARBIJO N95 | MÁSCARA N95 | MASCARILLA N95 | MASCARILLA N95 | MASCARILLA N95 | MÁSCARILLA DE PROTECCIÓN N95 | MASCARILLA N95 | MASCARILLA N95/N95 TIPO CONCHA | MASCARILLA | MASCARILLA N95 | MASCARILLA N95 | MÁSCARA N95 | TAPABOCAS N95 |
| PAINT PROJECT RESPIRATOR | MASCARILLA DE PINTOR | MÁSCARA RESPIRATÓRIA PARA PINTURA | RESPIRADOR DE MEDIO ROSTRO | RESPIRADOR FACIAL | RESPIRADOR | MEDIA MASCARILLA | MASCARA DE PINTURA, MASCARA ANTIGAS | RESPIRADOR/RESPIRADOR CON FILTRO | MEDIA MASCARA | RESPIRADOR | RESPIRADOR CON DOBLE FILTRO 3M | RESPIRADOR | RESPIRADOR |
| POWERED AIR-PURIFYING RESPIRATORS | RESPIRADORES PAPR Y DE AIRE SUMINISTRADO | RESPIRADOR PURIFICADOR DE AR | EQUIPO MOTOR VENTILADO | RESPIRADORES PURIFICADORES DE AIRE | RESPIRADOR | RESPIRADOR PURIFICADOR DE AIRE CON BATERÍA | RESPIRADOR CON AIRE PURIFICADO | RESPIRADOR/RESPIRADOR PURIFICADOR | RESPIRADOR | RESPIRADOR | RESPIRADOR PURIFICADOR COMPLETO | RESPIRADOR PURIFICADOR DE AR MOTORIZADO | RESPIRADOR |
| ISOLATION GOWN | DELANTAL | AVENTAL DESCARTÁVEL SEM MANGA | PECHERA | BATA DE AISLAMIENTO | DELANTAL | DELANTAL DESECHABLE | DELANTAL | DELANTAL/MANDIL | DELANTAL | DELANTAL DE PROTECCIÓN | DELANTAL | AVENTAL PLÁSTICO | DELANTAL |
| APRON | |||||||||||||
| LONG SLEEVED, DISPOSABLE GOWN | CAMISOLÍN | CAPOTE | PECHERA DELANTAL QUIRÚRGICO | BATA QUIRÚRGICA | GABACHON | BATA DE EPPI | BATA QUIRÚRGICA | BATA QUIRÚRGICA/BATA | BATA DESCARTABLE | BATA QUIRÚRGICA | BATA QUIRÚRGICA | BATA CIRÚRGICA DE USO ÚNICO | MONO QUIRÚRGICO, MONO QUIRÚRGICO COMPLETO |
| MEDICAL PROTECTING GOWN, MEDICAL ISOLATION GOWN | TRAJE DE PROTECCION | MACACÃO DE PROTEÇÃO COM CAPUZ | BUZO DE PAPEL, OVEROL, TRAJE TYVEK | TRAJE DE AISLAMIENTO PROTECTOR | TRAJE | MONO EPPI | TRAJE DE BIOSEGURIDAD | TRAJE DE PROTECCIÓN/OVEROL | TRAJE DE PROTECCIÓN | EQUIPO DE PROTECCIÓN PERSONAL, MAMELUCO | TRAJE DE PROTECCIÓN COMPLETO, MAMELUCO | FATO DE PROTEÇÃOCOM CAPUZ | TRAJE DE PROTECCIÓN |
| RUBBER GLOVES, DISPOSABLE GLOVES | GUANTES | LUVAS DE PROCEDIMENTO | GUANTES DE PROCEDIMIENTO | GUANTES | GUANTES | GUANTES | GUANTES | GUANTES | GUANTES | GUANTES | GUANTES DESCARTABLES | LUVAS | GUANTES |
| PROTECTIVE BOOTS, SHOE COVER | CUBREBOTAS | PROPÉ | CUBRECALZADO, CUBREZAPATOS | POLAINAS | ZAPATERAS | POLAINAS O PEUCS | CUBREBOTAS, CUBRECALZADO | CUBREBOTAS | CUBREBOTAS | CUBREBOTAS | CUBREBOTAS | COBRE-PÉS, CAPAS PARA SAPATOS LONGAS | BOTAS QUIRÚRGICAS |
The following recommendations are suggested:
- a)
To perform the swallowing assessment, the use of PPE that includes all the elements for practices that generate droplets and aerosols is suggested.
- b)
Each professional must be adequately trained in the use of PPE, according to the protocols established by the health center.
- c)
The elements and instruments used in the practices must be disposable or properly disinfected after each use.
- d)
It is important to categorize the different procedures by risk and correlate the risks with the viral load (Table 2).
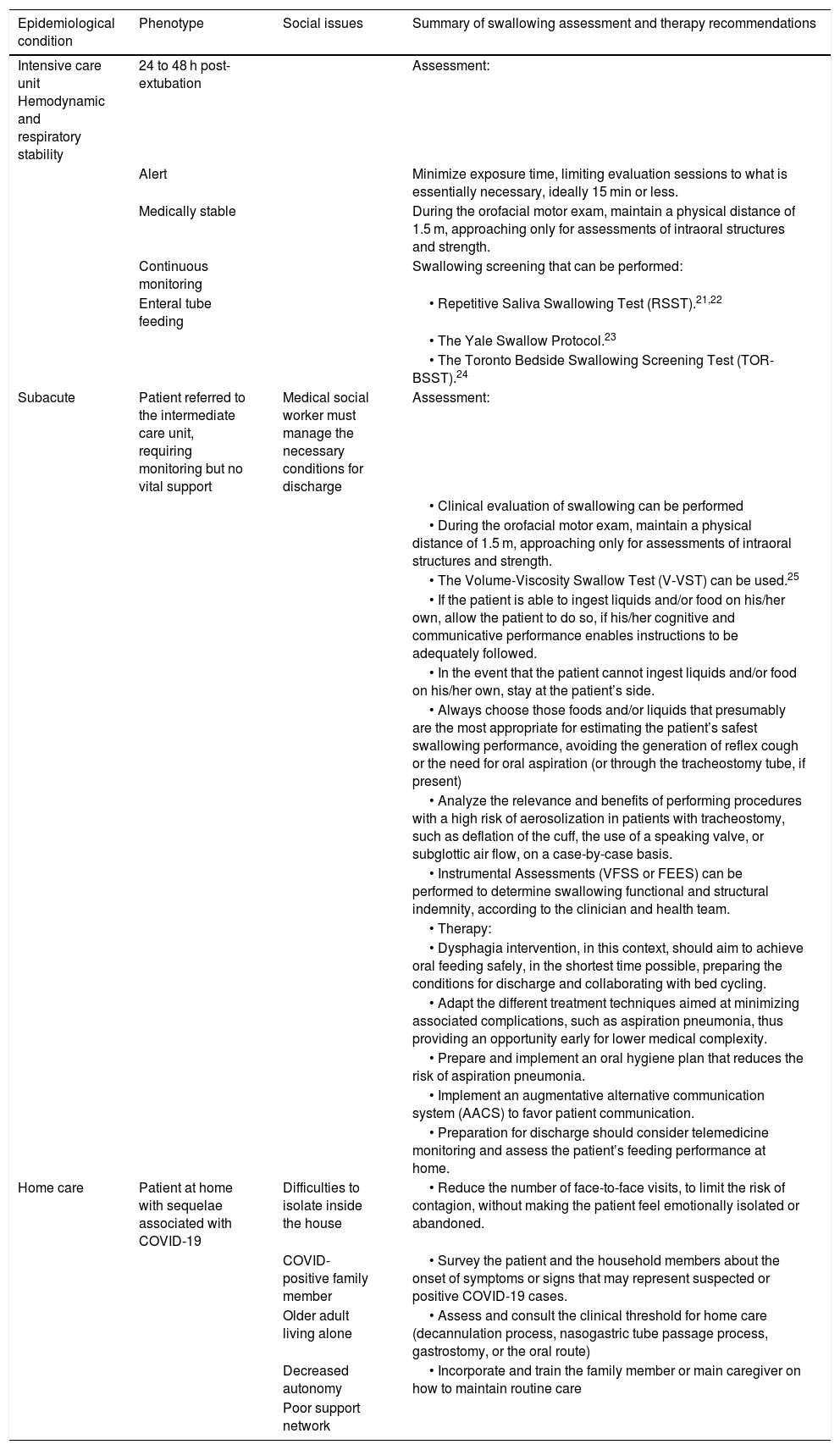
Table 2.Risk and viral load categorization table.
Epidemiological condition Phenotype Social issues Summary of swallowing assessment and therapy recommendations Intensive care unit Hemodynamic and respiratory stability 24 to 48 h post-extubation Assessment: Alert Minimize exposure time, limiting evaluation sessions to what is essentially necessary, ideally 15 min or less. Medically stable During the orofacial motor exam, maintain a physical distance of 1.5 m, approaching only for assessments of intraoral structures and strength. Continuous monitoring Swallowing screening that can be performed: Enteral tube feeding • Repetitive Saliva Swallowing Test (RSST).21,22 • The Yale Swallow Protocol.23 • The Toronto Bedside Swallowing Screening Test (TOR-BSST).24 Subacute Patient referred to the intermediate care unit, requiring monitoring but no vital support Medical social worker must manage the necessary conditions for discharge Assessment: • Clinical evaluation of swallowing can be performed • During the orofacial motor exam, maintain a physical distance of 1.5 m, approaching only for assessments of intraoral structures and strength. • The Volume-Viscosity Swallow Test (V-VST) can be used.25 • If the patient is able to ingest liquids and/or food on his/her own, allow the patient to do so, if his/her cognitive and communicative performance enables instructions to be adequately followed. • In the event that the patient cannot ingest liquids and/or food on his/her own, stay at the patient’s side. • Always choose those foods and/or liquids that presumably are the most appropriate for estimating the patient’s safest swallowing performance, avoiding the generation of reflex cough or the need for oral aspiration (or through the tracheostomy tube, if present) • Analyze the relevance and benefits of performing procedures with a high risk of aerosolization in patients with tracheostomy, such as deflation of the cuff, the use of a speaking valve, or subglottic air flow, on a case-by-case basis. • Instrumental Assessments (VFSS or FEES) can be performed to determine swallowing functional and structural indemnity, according to the clinician and health team. • Therapy: • Dysphagia intervention, in this context, should aim to achieve oral feeding safely, in the shortest time possible, preparing the conditions for discharge and collaborating with bed cycling. • Adapt the different treatment techniques aimed at minimizing associated complications, such as aspiration pneumonia, thus providing an opportunity early for lower medical complexity. • Prepare and implement an oral hygiene plan that reduces the risk of aspiration pneumonia. • Implement an augmentative alternative communication system (AACS) to favor patient communication. • Preparation for discharge should consider telemedicine monitoring and assess the patient’s feeding performance at home. Home care Patient at home with sequelae associated with COVID-19 Difficulties to isolate inside the house • Reduce the number of face-to-face visits, to limit the risk of contagion, without making the patient feel emotionally isolated or abandoned. COVID- positive family member • Survey the patient and the household members about the onset of symptoms or signs that may represent suspected or positive COVID-19 cases. Older adult living alone • Assess and consult the clinical threshold for home care (decannulation process, nasogastric tube passage process, gastrostomy, or the oral route) Decreased autonomy • Incorporate and train the family member or main caregiver on how to maintain routine care Poor support network *In all procedures, healthcare professionals (HCPs) must use Level 3 personal protective equipment (PPE).
In patients with confirmed COVID-19, postponing the clinical evaluation of swallowing in patients with dysphagia is recommended. Patients are predisposed to coughing during the procedure, and it is even more frequent in the context of their concomitant respiratory conditions7.
However, there are situations in which the procedures cannot be deferred because of patient needs and health center requirements, particularly those with great demand for high-complexity care beds in areas with an elevated prevalence of COVID-19 in the population. Thus, direct care should be reduced to cases in which the swallowing specialist, together with the team, estimates the predominance of benefits over risks25. In such cases, the clinical evaluation of swallowing can be carried out, in compliance with strict standards that enable the protection of the HCP and reduce the spread of the virus, using screening tests as an initial option.
Dysphagia screeningIn the context of the pandemic, swallowing clinicians should share tasks related to swallowing management with the health team. Training other professionals (nurses, respiratory therapists, or non-specialist physicians) in the use of those tools, receiving additional instructions from the outside26, reduces the number of HCPs that are exposed to SARS-CoV-2 and enables rational PPE use. It is always important to remember that the results obtained through the screening tests are useful for providing general recommendations to the health team, but not for planning the rehabilitation of dysphagia or its pathophysiology.
Using the following detection instruments, which are commonly described in the literature and easily applicable in the Latin American context, is suggested: the Volume-Viscosity Swallow Test (V-VST)27, the Yale Swallow Protocol28, the Repetitive Saliva Swallowing Test (RSST)29,30, and the Gugging Swallowing Screen (GUSS)31.
Clinical assessmentThe clinical assessment of swallowing must include the examination of the cognitive and communicative states, posture, and the oropharyngolaryngeal and respiratory systems. It is important to collect as much information as possible about the patient’s respiratory status, the use of supports to improve ventilation (oxygen and mechanical ventilation, among others), and the support of the multidisciplinary team, so that the patient’s tolerance to weaning, oxygen saturation stability, and respiratory rate can be checked26. There must be special considerations for patients with tracheostomy9,26.
Therefore, the following suggestions are recommended:
- a)
Check the availability of the PPE to be used. If PPE is limited, consider deferring the assessment.
- b)
If it does not interfere with the procedure, the patients should continue to wear PPE (goggles, masks). If that is not possible, make the necessary adjustments to the evaluation protocol.
- c)
If the same HCP provides services to patients that are negative for SARS-CoV-2, as well as to patients that are positive, the negative patients should be treated first.
- d)
Minimize exposure time, limiting the evaluation sessions to the bare essentials, ideally 15 min or less.
- e)
Keep a physical distance of at least 1.5 m between the HCP and the patient, when feasible, during the interview and cognitive-communication assessment.
- f)
A distance of 1.5 m should be kept during the orofacial motor exam, moving closer only for evaluating the intraoral structures and making the strength assessment.
- g)
Do not evaluate voluntary cough, unless absolutely necessary.
- h)
If the patient can ingest liquids and/or food independently, allow him/her to do so, if the patient’s cognitive and communicative performance allows him/her to adequately follow the instructions.
- i)
If the patient cannot ingest liquids and/or food independently, stay at the patient’s side.
- j)
Always choose the foods and/or liquids that are the most appropriate for the estimated condition of the patient, avoiding the generation of reflex cough or the need for aspirating the oral cavity (or the tracheostomy tube, if present).
- k)
Individually analyze the relevance and benefits of performing procedures with a high risk of aerosolization in patients with tracheostomy, such as deflation of the cuff, the use of a speaking valve, or subglottic air flow.
The acoustic analysis of swallowing, or cervical auscultation (CA)32, is an important procedure, in the context of the pandemic, that can be performed rapidly, minimizing the risk of contagion2,6,23. In practice, the sequential relation of swallowing physiology should be kept in mind33, as well as interference in the uptake of sounds that may occur due to the respiratory repercussion of COVID-19 and the presence of continuous or discontinuous transmission noise and aggregates, which can make analysis difficult34,35.
Therefore, the following considerations are suggested for CA use:
- a)
Use CA when it is strictly necessary.
- b)
Whenever possible, each patient should be designated his/her own equipment and it should not be shared. Otherwise, isolate the equipment with an examination glove and disinfect it immediately, according to the local protocol.
- c)
The HCP must stand to the side of or behind the patient. Do not stand facing the patient at the time of the test.
- d)
If the CA is carried out digitally, generate the graphic-acoustic analysis outside of the consultation room, to minimize contact with the patient.
Dysphagia severity scales are instruments used within the diagnostic process, to help identify risk, as an instrument to maintain a common language between HCPs, and a parameter to control the effectiveness of rehabilitation. Said scales have been proposed in several studies, but consensus criteria are not always used36, and so the selection of a particular scale should be made, according to the characteristics and resources of each hospital, clinic, or healthcare center. It is important for the health team to be familiar with those scales, facilitating clinical decision-making and their subsequent implementation.
Considerations for instrumental assessment of swallowingAll instrumental assessments of swallowing are considered AGPs and should be elective procedures. However, the patient’s condition sometimes makes it impossible to defer the study. For example, COVID-19 patients, especially those that underwent endotracheal intubation after extubation in the intensive care unit (ICU), may need those procedures the most37,38.
General suggestions for instrumental assessment are:
- a)
The decision to indicate instrumental assessment procedures should be based on the risk-benefit analysis for each patient.
- b)
Perform COVID-19 testing (polymerase chain reaction [PCR]) prior to the procedure, whenever possible.
- c)
Wear full PPE, regarding all patients that have a positive test or are untested, prioritizing patients with nutritional deterioration due to dysphagia and in whom the result is relevant for making decisions about their management.
- d)
Strict use of PPE (masks [FFP2, N95, or higher], eye protection, a long-sleeved apron, and gloves).
- e)
Carry out the procedures with the minimum number of HCPs. Only the personnel that is essential for carrying out the evaluation should be present.
- f)
Allow sufficient time between patients, for disinfecting and sterilizing the equipment.
High levels of viral load have been identified in the oral and nasal cavities. Therefore, oropharyngeal manipulation represents a high risk of infection, by activating the cough or vomiting reflexes. In that context, the following specific recommendations are suggested37,39:
- a)
Postpone follow-up endoscopic exams and screenings, if possible.
- b)
Use the video recording system whenever possible, because adequate physical distance from the patient can be maintained and the study can be reviewed several times, to better understand the swallowing disorder.
- c)
Perform the FEES in an airborne infection isolation room (AIIR), or a room with adequate ventilation, according to the AGP regulations at each health service. Use a negative pressure room, if available.
Before conducting the examination, a clinical reevaluation is proposed. Videofluoroscopy should be ordered, only if the oral route remains unsafe. Videofluoroscopy is preferred over FEES, in COVID-19-positive patients or COVID-19-suspected cases40. Nevertheless, when oral feeding is possible, videofluoroscopy should only be performed in patients at high risk of aspiration/malnutrition. Specific recommendations for the procedure are:
- a)
Prior instructions must be given to the patient and the multidisciplinary support team, for carrying out an examination in the shortest time possible.
- b)
Allow self-administered food/liquids during the test, whenever possible41.
- c)
The use of scales, such as the Rosenbek Penetration-Aspiration Scale (PAS)42,43 and the Dysphagia Outcome and Severity Scale (DOSS), are recommended for analyzing the videofluoroscopy findings44.
- d)
The exam should be carried out in large rooms, with remote access to screens, whenever possible.
- e)
Use an IQAir HealthPro (Incen AG) with a HEPA class H13 filtration system, if possible, for the configuration of the radiology room, to evacuate particles in the air and prevent viral transmission through droplets and aerosols generated by episodes of coughing, during videofluoroscopy25,39.
Motility tests and functional disorders are generally not urgent and can be scheduled and planned well. Like FEES and videofluoroscopy, esophageal manometry is considered a high exposure risk for HCPs because it is an AGP. There are few reports in the literature on this procedure, in the context of the COVID-19 pandemic45, but based on the information available, we propose the following suggestions:
- a)
When placing the probe, cover the patient’s mouth with a modified surgical mask.
- b)
Do not perform the procedure on a patient that has tested positive for COVID-19. The procedure can be postponed until a negative test is obtained. In the interim, the patient can be referred for an esophagogram, if pending.
- c)
The catheter or probe is regularly cleaned, according to the material and protocol of each laboratory, but it is specifically recommended to add cleaning with a cloth, using disinfectants, such as 70% alcohol or a sodium hypochlorite solution.
As is the case with the previously described exams, esophagogastroduodenoscopy is a procedure with a high risk for contagion of COVID-19, for both HCPs and patients, due to exposure to respiratory or gastrointestinal secretions46,47. In times of COVID-19, and according to the clinical and epidemiological risks, all the protection recommendations mentioned above, for patients and HCPs during the performance of endoscopy, should be followed.
Swallow therapySwallowing specialists must participate in the clinical decision-making process of the health team, even in patients that are medically unstable. That includes providing information to the healthcare team, indirect management of dysphagia, through instructing team members, and direct treatment.
The characteristics of each healthcare center must always be considered. Indeed, in most Latin American health centers there are few swallowing specialists, if any at all. Therefore, implementing a triage to organize the provision of services, according to existing resources and the needs of each patient, is suggested. Said planning must take into account the incidence of consciousness and cognition, determining treatment candidates on a daily basis, as well as the types of patients and the frequency of the intervention, according to the expected recovery of the patients.
Patients in intensive care unitsPatients with COVID-19 that have been admitted to an ICU, especially those of advanced age with underlying diseases, such as hypertension, chronic heart and lung diseases, diabetes, and obesity, have more complications and require long periods of orotracheal intubation48–50. Orotracheal intubation can cause dysphagia due to a decrease in oropharyngeal and laryngeal sensation, lesions and edema in the swallowing structures, atrophy of the oropharyngeal muscles, cognitive disturbances, and respiratory-swallowing incoordination51. In addition, various neurological manifestations associated with COVID-19 disease have been described, including alterations in dependent functions of the central and/or peripheral nervous system52. This is seen in a clinical context, when cognitive, motor, and respiratory fluctuations are frequent, and such changes should be monitored by the swallowing specialist and healthcare team26.
The achievement of re-functionalization of the sphincters and aerodigestive tract pressures, in patients that have undergone prolonged intubation or long periods of tracheostomy, requires a treatment process9. For this to occur, an early approach to the swallowing function is essential; the tone and motility of the oropharyngolaryngeal structures and the swallowing respiratory synchrony tend to recover through such an approach53. Early approach aims to transfer the patient to a lower-complexity room, as soon as possible, in preparation for discharge.
The following suggestions are made for managing ICU patients:
- a)
The patient’s condition must be stable (with or without external support), allowing interventions with a low generation of respiratory and/or hemodynamic changes.
- b)
Adapt the different rehabilitation techniques to minimize complications, such as aspiration pneumonia9.
- c)
Prepare and implement an oral hygiene plan that reduces the risk of aspiration pneumonia9,54.
- d)
Defer any procedure that requires deflation of the tracheostomy cuff. Postpone it until the patient is considered negative or when the benefits to the individual outweigh the risks of the intervention50.
- e)
Implement an augmentative alternative communication system (AACS), to favor patient communication, facilitating the patient’s ability to deliver information about his/her swallowing condition.
In this context, the aim of dysphagia treatment should be to safely achieve oral feeding in the shortest time possible, preparing the conditions for discharge, and collaborating with the bed cycle. Preparation for discharge should take telemedicine monitoring into account, to assess the performance of the patient’s feeding at home. As mentioned above, instrumental assessments should be performed to determine swallowing functionality and structural compensation, only when the benefits outweigh the risks.
In-office swallowing therapyIn Latin America, most of the public health agencies have suggested the suspension of elective outpatient care, limiting patient interactions to emergency cases only, as a preventive or mitigating measure against the advance of the SARS-CoV-2 virus. Outpatient clinic staff must consider every patient as a suspected COVID-19 patient and manage the correct use of PPE. That precaution is particularly essential, when planning actions that generate aerosols55.
Specific recommendations for in-office treatment are listed below:
- a)
Upon discharge, recovered patients should be encouraged to continue with care, preferably by telemedicine.
- b)
Carry out a telephone survey, prior to admission of the patient/caregiver, to verify the presence of signs or symptoms of COVID-19.
- c)
Teams that treat dysphagia in COVID-19-positive patients should not be the same teams that treat elective outpatients.
- d)
In outpatient care, the intervals between consultations should be optimally programmed, with respect to the time needed to disinfect the environment, between each appointment.
In home care settings, the HCP must take the standard precautions, regarding his/her transportation to the patient’s home. For their part, the patient and his/her family should take the same precautions, as well as create a sanitizing room in the house for the HCP. The World Health Organization has created guidelines for the HCP in the home care scenario. Those recommendations were adapted to the dysphagia intervention, as follows56:
- a)
Be informed about the onset of symptoms or signs that could indicate suspected or positive COVID-19 cases, with respect to the patient or family members in a home care setting.
- b)
Avoid attending to a home care patient after a hospital shift.
- c)
Comply with the local transport regulations for going to the patient’s house.
- d)
Promote telehealth to minimize the risk of SARS-CoV-2 transmission.
- e)
Assess and consult the clinical threshold for home care (decannulation process, nasogastric tube passage process, gastrostomy, or oral route).
- f)
Incorporate and train the family member or principal caregiver, so that he/she can maintain routine care.
- g)
Reduce the number of face-to-face visits, to limit the risk of contagion, without making the patient feel emotionally isolated or abandoned.
Medical centers have chosen to close clinics and outpatient procedures to mitigate the impact of the disease for the following reasons: precaution, protection of patients and HCPs from exposure to disease, and limited resources. Elective procedures and surgeries have been postponed, to preserve existing supplies and allocate them to the care of patients infected with COVID-1957,58. Within that framework, the LADS has established a series of suggestions for the more frequent medical procedures in dysphagia.
As general recommendations, all patients, even asymptomatic ones, should have a PCR test for SARS-CoV-2, one or two days before the procedure. Procedures should be postponed in positive patients until their performance is deemed safe. Unfortunately, due to the low sensitivity of PCR for diagnosing COVID-19 in pre-symptomatic patients, a negative result does not mean that preventive measures against infection can be suspended, even in asymptomatic patients, and so adequate PPE use must be strictly adhered to. In addition, closed-circuit suction systems with an anti-viral filter and negative pressure operating rooms should be used, whenever possible.
Specific recommendations for each procedure are outlined below:
Botulinum toxinAs a non-emergency medical procedure, the application of botulinum toxin to the salivary glands has been postponed in several countries. As a result, controlling hypersalivation in patients that need said applications, to contain recurrent aspiration pneumonia, has become particularly difficult59. Therefore, the LADS suggests the following recommendations for the treatment of hypersalivation:
- a)
Patients that are stable, with the use of anticholinergic drugs, may continue clinical treatment.
- b)
Intraglandular botulinum toxin application in patients with hypersalivation should only be prescribed in cases that present with side effects or no response to anticholinergic drugs.
The following recommendations are suggested for surgical procedures:
- a)
When deciding to intervene surgically in a dysphagic patient, in times of COVID-19, the possible benefits and risks of the surgery must be weighed, including the risk of transmission to the patient, as well as to the HCP, during both the procedure and the postoperative period.
- b)
The surgical staff should be as small as possible60.
- c)
The use of an electric or ultrasonic scalpel can promote aerosol formation, and therefore, should be avoided. When necessary, they should be simultaneously used with a vacuum coupled to a HEPA filter system61.
- d)
Local-regional anesthesia should be preferred whenever possible, as it reduces the number of AGPs (i.e., intubation and extubation of the patient)62.
The recommendations for esophageal dilations are the same as those described for endoscopic procedures.
Cricopharyngeal myotomyDespite being a simple procedure, patients that undergo cricopharyngeal myotomy generally require postoperative rehabilitation for a relatively long period of time. Thus, the procedure should be avoided, if possible, due to the potential risk of SARS-CoV-2 spread during rehabilitation6. On the other hand, in the dysphagic patient with a clear indication for such a procedure, myotomy may be a better alternative than tracheostomy, which has a higher risk of aerosolization60.
For Zenker’s diverticulum, open surgery should be preferred in patients known to be positive for COVID-19, whereas endoscopic approaches may be considered for patients with a negative PCR test. The latter approach should be considered for elderly patients or those with comorbidities, as it requires less surgical time and shorter hospital stay63–65. Some surgeons use an intraesophageal balloon as an aid, during the anatomical location of muscle fibers of the upper esophageal sphincter66,67. That maneuver should be avoided in patients with COVID-19, to minimize the risk of exposure to potentially infected mucosa.
Gastroesophageal refluxThe risk of developing gastroesophageal reflux disease (GERD) is increased in critically ill patients, by the presence of nasogastric tubes, the dorsal decubitus position, and high dose sedation, among others. GERD affects laryngeal sphincter function and increases the risk of aspiration. Chronic GERD can contribute to the development of postintubation dysphagia41.
Proton pump inhibitors (PPIs) remain the first-line drugs in the pharmacological treatment of GERD. Prokinetic agents can accelerate gastric emptying, increase resting pressure of the lower esophageal sphincter, or increase esophageal clearance of refluxed contents. Combination therapy of a PPI plus a prokinetic agent should be considered in patients with GERD and delayed gastric emptying.
Artificial nutritionNutritional treatment is key in critical patients with COVID-19, to avoid malnutrition, with the aim of reducing mortality and exacerbation of the clinical condition. The LADS has established the following suggestions for its use:
Enteral tubesEnteral nutrition is recommended in patients with COVID-19 that do not meet their requirements through oral intake and/or cannot utilize the oral route68 due to dysphagia, neurological/respiratory status, or to other associated comorbidities.
There is no evidence demonstrating that the direct placement of nasoenteral tubes is a risky procedure for HCPs. However, the risk is inferred because tube placement stimulates the patient’s oropharynx and pharynx, causing coughing and a possible increase in secretions and aerosols69. Consequently, nasojejunal, nasogastric, and nasoduodenal tube placement should be performed by non-endoscopic methods due to the increased risk of COVID-19 transmission (unless the nasojejunal or nasoduodenal position is strictly required).
There is no evidence that a patient receiving enteral nutrition at home during the COVID-19 pandemic should modify his/her treatment.
GastrostomyPercutaneous endoscopic gastrostomy (PEG) has been established as a treatment option for patients with transient or permanent dysphagia due to neurological disorders. It may be required in cases of COVID-19, in which patients cannot meet their nutritional requirements over long periods of time.
The placement of a percutaneous gastrostomy tube, guided by endoscopy, is generally an elective procedure. The recommendations are the same as those previously described for endoscopy.
Telemedicine in swallowing rehabilitationAs noted throughout the present document, the use of telemedicine should be promoted as a safe way to provide care for patients with dysphagia. To reduce bias, the telemedicine clinical assessment of swallowing should be combined with quantitative measures, such as self-perception questionnaires and the use of clinical scales, which, in combination with the medical history and clinical observation, can provide the necessary information for better dysphagia management. Procedures must be adapted, heeding the following suggestions:
- a)
Prior to the telemedicine clinical evaluation of swallowing, the HCP must make sure that food and fluids are available to the patient, provide the patient with standardized food consistencies, use food coloring to improve visibility, and utilize a colored tape placed at the thyroid level, to visualize laryngeal elevation during swallowing.
- b)
The active participation of caregivers is mandatory, especially in patients with cognitive difficulties or motor interference. Good communication between the clinician and the caregiver facilitates treatment adherence70.
- c)
In-person patient assessment should only be carried out in emergency situations that cannot be postponed. The decision to have face-to-face treatment should be made after a team discussion or when the use of telemedicine prevents the patient from achieving an adequate condition of health.
- d)
Inadequate selection of the type of technology to be used, insufficiently trained HCPs, and patients with digital illiteracy can be limitations of telemedicine. All those variables must be considered and compensated for creatively.
Finally, to support clinicians during the evaluation, diagnosis, and treatment processes, we have proposed an algorithm that includes the general considerations regarding the management of swallowing disorders (Fig. 1). To correctly apply the algorithm, in the context of the COVID-19 pandemic, the HCP must be familiar with all the suggestions proposed in the present article.
Limitations
The suggestions proposed herein are based on the international literature available on the subject and no system for assessing the evidence was employed. Said recommendations are based on clinical experience, given that the ever-increasing knowledge produced during the pandemic will provide more robust information on the subject. Not all the Latin American countries are represented by the authors, but it is our hope that more countries join the society in the coming years, enriching all future updates of the position statements of the LADS.
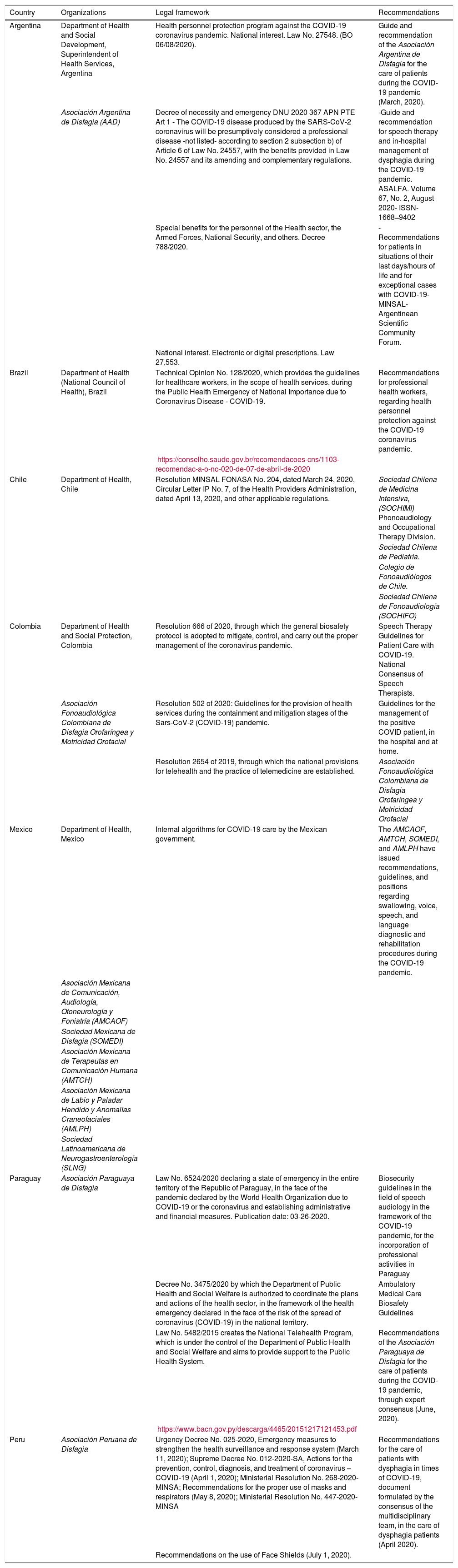
Legal framework and ethical challengesIt is important to be familiar with the guidelines for providing care to patients with COVID-19 in the different countries of Latin America, as developed by their respective departments of health, and with those contained in the position statements of local health organizations (Table 3).
Legal considerations for the protection of healthcare professionals, in the context of COVID-19, are available in some Latin American countries.
| Country | Organizations | Legal framework | Recommendations |
|---|---|---|---|
| Argentina | Department of Health and Social Development, Superintendent of Health Services, Argentina | Health personnel protection program against the COVID-19 coronavirus pandemic. National interest. Law No. 27548. (BO 06/08/2020). | Guide and recommendation of the Asociación Argentina de Disfagia for the care of patients during the COVID-19 pandemic (March, 2020). |
| Asociación Argentina de Disfagia (AAD) | Decree of necessity and emergency DNU 2020 367 APN PTE Art 1 - The COVID-19 disease produced by the SARS-CoV-2 coronavirus will be presumptively considered a professional disease -not listed- according to section 2 subsection b) of Article 6 of Law No. 24557, with the benefits provided in Law No. 24557 and its amending and complementary regulations. | -Guide and recommendation for speech therapy and in-hospital management of dysphagia during the COVID-19 pandemic. ASALFA. Volume 67, No. 2, August 2020- ISSN-1668−9402 | |
| Special benefits for the personnel of the Health sector, the Armed Forces, National Security, and others. Decree 788/2020. | -Recommendations for patients in situations of their last days/hours of life and for exceptional cases with COVID-19- MINSAL- Argentinean Scientific Community Forum. | ||
| National interest. Electronic or digital prescriptions. Law 27,553. | |||
| Brazil | Department of Health (National Council of Health), Brazil | Technical Opinion No. 128/2020, which provides the guidelines for healthcare workers, in the scope of health services, during the Public Health Emergency of National Importance due to Coronavirus Disease - COVID-19. | Recommendations for professional health workers, regarding health personnel protection against the COVID-19 coronavirus pandemic. |
| https://conselho.saude.gov.br/recomendacoes-cns/1103-recomendac-a-o-no-020-de-07-de-abril-de-2020 | |||
| Chile | Department of Health, Chile | Resolution MINSAL FONASA No. 204, dated March 24, 2020, Circular Letter IP No. 7, of the Health Providers Administration, dated April 13, 2020, and other applicable regulations. | Sociedad Chilena de Medicina Intensiva, (SOCHIMI) Phonoaudiology and Occupational Therapy Division. |
| Sociedad Chilena de Pediatría. | |||
| Colegio de Fonoaudiólogos de Chile. | |||
| Sociedad Chilena de Fonoaudiología (SOCHIFO) | |||
| Colombia | Department of Health and Social Protection, Colombia | Resolution 666 of 2020, through which the general biosafety protocol is adopted to mitigate, control, and carry out the proper management of the coronavirus pandemic. | Speech Therapy Guidelines for Patient Care with COVID-19. National Consensus of Speech Therapists. |
| Asociación Fonoaudiológica Colombiana de Disfagia Orofaríngea y Motricidad Orofacial | Resolution 502 of 2020: Guidelines for the provision of health services during the containment and mitigation stages of the Sars-CoV-2 (COVID-19) pandemic. | Guidelines for the management of the positive COVID patient, in the hospital and at home. | |
| Resolution 2654 of 2019, through which the national provisions for telehealth and the practice of telemedicine are established. | Asociación Fonoaudiológica Colombiana de Disfagia Orofaríngea y Motricidad Orofacial | ||
| Mexico | Department of Health, Mexico | Internal algorithms for COVID-19 care by the Mexican government. | The AMCAOF, AMTCH, SOMEDI, and AMLPH have issued recommendations, guidelines, and positions regarding swallowing, voice, speech, and language diagnostic and rehabilitation procedures during the COVID-19 pandemic. |
| Asociación Mexicana de Comunicación, Audiología, Otoneurología y Foniatría (AMCAOF) | |||
| Sociedad Mexicana de Disfagia (SOMEDI) | |||
| Asociación Mexicana de Terapeutas en Comunicación Humana (AMTCH) | |||
| Asociación Mexicana de Labio y Paladar Hendido y Anomalías Craneofaciales (AMLPH) | |||
| Sociedad Latinoamericana de Neurogastroenterología (SLNG) | |||
| Paraguay | Asociación Paraguaya de Disfagia | Law No. 6524/2020 declaring a state of emergency in the entire territory of the Republic of Paraguay, in the face of the pandemic declared by the World Health Organization due to COVID-19 or the coronavirus and establishing administrative and financial measures. Publication date: 03-26-2020. | Biosecurity guidelines in the field of speech audiology in the framework of the COVID-19 pandemic, for the incorporation of professional activities in Paraguay |
| Decree No. 3475/2020 by which the Department of Public Health and Social Welfare is authorized to coordinate the plans and actions of the health sector, in the framework of the health emergency declared in the face of the risk of the spread of coronavirus (COVID-19) in the national territory. | Ambulatory Medical Care Biosafety Guidelines | ||
| Law No. 5482/2015 creates the National Telehealth Program, which is under the control of the Department of Public Health and Social Welfare and aims to provide support to the Public Health System. | Recommendations of the Asociación Paraguaya de Disfagia for the care of patients during the COVID-19 pandemic, through expert consensus (June, 2020). | ||
| https://www.bacn.gov.py/descarga/4465/20151217121453.pdf | |||
| Peru | Asociación Peruana de Disfagia | Urgency Decree No. 025-2020, Emergency measures to strengthen the health surveillance and response system (March 11, 2020); Supreme Decree No. 012-2020-SA, Actions for the prevention, control, diagnosis, and treatment of coronavirus – COVID-19 (April 1, 2020); Ministerial Resolution No. 268-2020-MINSA; Recommendations for the proper use of masks and respirators (May 8, 2020); Ministerial Resolution No. 447-2020-MINSA | Recommendations for the care of patients with dysphagia in times of COVID-19, document formulated by the consensus of the multidisciplinary team, in the care of dysphagia patients (April 2020). |
| Recommendations on the use of Face Shields (July 1, 2020). |
The present position statement was developed to provide immediate guidance for the multidisciplinary dysphagia care team during the pandemic. The authors included recommendations related to the use of PPE, as well as to the diagnosis, treatment, and rehabilitation of oropharyngeal and esophageal dysphagia, to reduce the risk of contagion and spread of the virus in the environment. These recommendations are based on clinical experience, given that, at present, scientific evidence is still limited, and the development of knowledge about the pandemic will be a continuous learning experience.
The publishing of international clinical experience, utilizing the scientific method, will enable us to know more about the evolution of patients that present with sequelae after having had COVID-19 infection.
Note for special considerationsIn both oropharyngeal and esophageal dysphagia, if there are negative studies in the diagnostic algorithm, the possibility of gastroesophageal reflux disease should be ruled out as a condition, through either a therapeutic test and/or a pH monitoring study71,72, and biopsies of the esophageal mucosa should be performed in patients with dysphagia, to rule out eosinophilic esophagitis73,74. When complementary studies are normal or negative, consider the possibility of functional dysphagia (after exclusion of globus, xerostomia, odynophagia)75,76.
Financial disclosureNo financial support was received in relation to this work.
Conflict of interestCarlos Manzano, Rodrigo Tobar-Fredes, Deborah Salle Levy, Rui Imamura, Rodrigo Morales Fernández, Liz Ojeda Peña, David Parra Reyes, Patricia Santoro, Valeria Tona, Omar Edel Trujillo Benavides, Miguel Vargas García and Ana Maria Furkima declare that they have no conflict of interest. Monica Rocío Zavala Solares has given lectures at Medtronic.
Special thanks to Adrian Castillo-Allendes, Francisco Contreras-Ruston, Lady Cantor, Juliana Codino, Marco Guzman, Celina Malebrán, Axel Pavez, Thays Vaiano, Fabiana Wilder and Mara Behlau, authors of the article, “Voice therapy in the context of the COVID-19 pandemic”; recommendations for clinical practice that were the source of inspiration and motivation for this article by the Latin American Dysphagia Society (LADS). We also wish to thank the members of the scientific committee of the LADS from different countries. Special appreciation to Ioko Inamoto (Japan), Pere Clavé (Spain), and Luis F. Riquelme (the United States) for their expert feedback on this document. The present article is a posthumous tribute to all those who have passed away in the course of carrying out their professional duties, especially to the multidisciplinary HCPs of Latin America for their dedication, vocation, courage, and sacrifice.
Please cite this article as: Manzano-Aquiahuatl C, Tobar-Fredes R, Zavala-Solares MR, Salle-Levy D, Imamura R, Morales-Fernández R, et al. Posicionamiento de la Sociedad Latinoamericana de Disfagia para el manejo de la disfagia orofaríngea y esofágica durante la pandemia COVID-19. Rev Gastroenterol Méx. 2021. https://doi.org/10.1016/j.rgmx.2021.08.002
Not only patients infected with SARS-CoV-2 need care. As the pandemic continues, many institutions and medical societies have suggested postponing non-emergency medical care, which has led to a marked reduction in outpatient care10–16. As a result of this, the diagnosis and treatment of other progressive diseases related to COVID-19 have been delayed, which has had an impact on morbidity, mortality and treatment costs for these patients17–19. As the incidence curve improves, it will be necessary to consider resuming the care of elective patients considering the challenges related to the safety of patients and health care professionals (HCPs), as well as the availability of personal protective equipment (PPE).


www.publicationethics.org.