







Irritable bowel syndrome (IBS) is a functional gastrointestinal disorder characterized by abdominal pain or discomfort that is associated with altered bowel habit. Both its prevalence and clinical characteristics vary throughout Latin America. A percentage of patients does not seek medical attention, therefore a reliable prevalence figure can only be established by interviewing non-selected populations.
AimsTo study the prevalence and clinical characteristics of IBS symptoms in non-selected subjects in Santiago, Chile.
MethodsA total of 437 shopping mall visitors above the age of 15 years (246 women) participated in the study by answering the Rome II validated questionnaire for IBS. The demographic and socioeconomic backgrounds, comorbidities, and a family history of IBS were registered.
ResultsA total of 64.1% subjects reported having gastrointestinal symptoms and 28.6% had symptoms suggestive of IBS. When the subjects with IBS symptoms were compared with the asymptomatic individuals, a predominance of women (65.6 vs 42.9, p<0.001) and a greater cholecystectomy frequency (33.6 vs 12.9% p<0.05) were observed in the former. The age of symptom onset was 30.4 years. An equal percentage of subjects (42.4%) presented with diarrhea and constipation and 15.2% presented with alternating IBS. Participants with a higher educational level reported a lower percentage of IBS (p<0.05). A family history of the disease was present in 40% of the subjects with IBS, compared with 14.9% in the asymptomatic individuals (p<0.05). Only 39.2% of the subjects had seen a physician for their symptoms and the treatment and tests ordered were inappropriate.
ConclusionsThe prevalence of IBS symptoms in the population studied is one of the highest described. Therefore, health teams should have the necessary knowledge and skill required for its management.
El síndrome de intestino irritable (SII) es un trastorno funcional digestivo caracterizado por dolor o malestar abdominal, asociado a alteraciones del hábito intestinal. Tanto prevalencia como características clínicas son variables en Latinoamerica. Un porcentaje de pacientes no consulta, la real prevalencia sólo puede establecerse encuestando población no seleccionada.
ObjetivosEstudiar la prevalencia y características clínicas de síntomas de SII en sujetos no seleccionados de Santiago, Chile.
MétodosParticiparon 437 mayores de 15 años (246 mujeres), asistentes a centros comerciales, quienes respondieron el cuestionario validado de Roma II para SII. Se registraron, antecedentes demográficos, socioeconómicos, comorbilidades y antecedentes familiares de SII.
ResultadosUn 64,1% relató síntomas digestivos, 28,6% síntomas sugerentes de SII. Comparando sujetos con síntomas de SII con asintomáticos se observó en los primeros: predominio del sexo femenino (65,6 vs. 42,9. p<0.001) y mayor frecuencia de colecistectomía (33,6 vs. 12,9% p<0,05). La edad de inicio de los síntomas fue 30,4 años. Se observó igual porcentaje (42,4%) entre pacientes con diarrea y con estreñimiento, y 15,2% alternante. Sujetos con mayor nivel educacional reportaron menor porcentaje de SII (p<0,05). El antecedente familiar de SII estuvo presente en 40% de sujetos con SII, comparado con sujetos asintomáticos 14,9% (p<0,05). Solo 39,2% consultaron al médico. El tratamiento y exámenes solicitados no estuvieron acorde con los síntomas.
ConclusiónLa prevalencia de síntomas de SII en la población estudiada es una de las más altas descritas, por lo cual los equipos de salud debieran tener los conocimientos y destrezas adecuados para su manejo.
Irritable bowel syndrome (IBS) is part of a subgroup of the so-called functional gastrointestinal disorders, characterized by abdominal pain and discomfort associated with changes in the bowel habit and bowel movement disorders. The Rome criteria have established definitions relative to both the characteristics and duration of these alterations.1–3
Studies conducted on this group of patients have revealed different pathophysiologic disorders such as: visceral hyperalgesia,4,5 altered motility and bowel transit,2,6,7 changes in the microbiota,8 and others associated with disorders related to the psychosocial sphere.9
Its impact on the health of the population is important, given that it constitutes a high percentage of the gastroenterologic consultations in the United States and is a significant cause of absenteeism in the workplace.2,10 Its economic impact is great due to the requirements of a larger number of medical consultations, tests, and medicines, compared with the population that does not present with IBS.11–13
This pathology has a precocious onset and it is estimated to affect from 10 to 15% of schoolchildren, half of whom continue to present with symptoms into adulthood.14
Its prevalence is variable depending on the communities studied and in several Latin American countries it varies between 9 and 18%;15 whether these variations are real, or are the result of studies on different population groups, or depend on surveys using different instruments, or on the existence or not of confirmation after diagnosis, is the subject of debate. Today well-structured surveys are available that make an important approach to diagnosis possible, while at the same time reducing the presence of organic pathology.
It is believed that the majority of patients with IBS do not seek medical attention for their symptoms,13 and therefore the only way to establish the true prevalence in a population is to survey an important number of individuals from a non-selected population. In this regard, no previous studies with these characteristics have been carried out.
Our aim was to study the prevalence of symptoms consistent with IBS in a non-selected population in Santiago de Chile, using the Rome II questionnaire for IBS to conduct the survey.
MethodsA cross-sectional study was conducted through surveys carried out on weekends by medical interns from the Universidad de Chile that were previously instructed in the application of the survey.
This analysis was carried out within the time frame of June to July of 2005 in 5 large shopping centers located in the eastern (n=88), central (n=88), northern (n=87), western (n=85), and southern (n=89) areas of the city of Santiago.
The interns applying the surveys set up at the entrances to the shopping malls and personally invited men and women above the age of 15 years to directly and voluntarily answer a questionnaire, without receiving any type of compensation or additional benefit.
Epidemiologic characteristics: information on demographic characteristics were collected that included sex, age, the area of residence in Santiago (residents of other cities were not included), educational level, and current occupation. The areas of residence were arranged into 5 geographic zones that resulted in general groupings of populations of different socioeconomic levels; zone 1 represented the highest level and zone 5 the lowest level. The educational level and occupation were grouped into 5 categories: 1) a completed university education and/or university degree, 2) a completed high school education or incomplete university studies, 3) housewives and domestic workers, 4) employed with completed technical studies, and 5) non-specialized workers (with partial or completed studies).
For the purpose of determining the prevalence of IBS symptoms, a Spanish language version of the Rome II modular questionnaire for functional gastrointestinal disorders was used (Fig. 116).
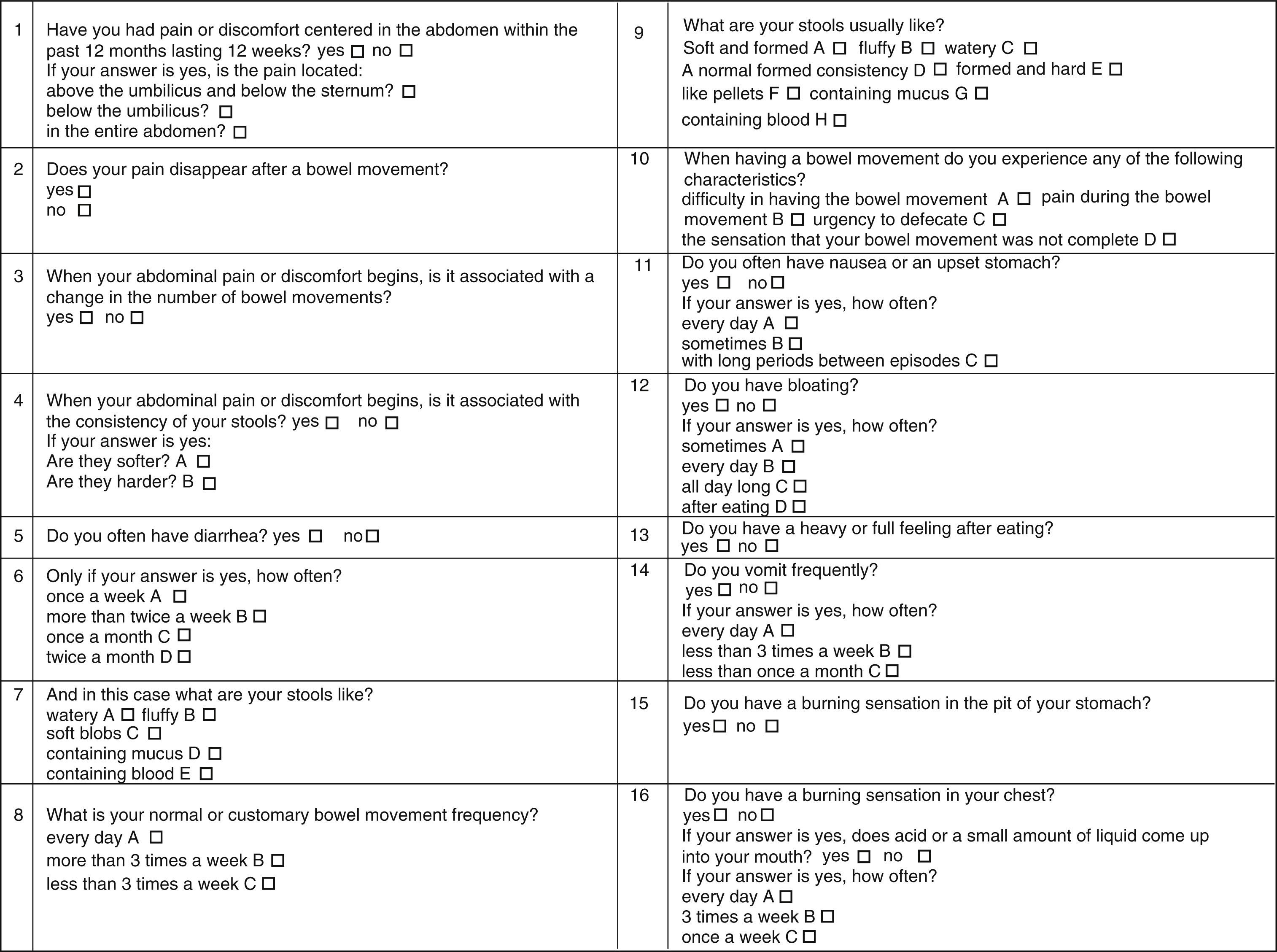
An affirmative answer to the question (Q) associated with 2 or more affirmative answers to Q2, Q3, or Q4 and a negative answer to Q 11, Q 13, Q 14, Q 15, and Q 16 were used as the criteria for diagnosing IBS. Diarrhea-predominant IBS (IBS-D) diagnosis: IBS criteria and 2 or more affirmative answers to Q 4A, Q 5, Q 6B, Q 7A-D, Q 9-C, and Q 10C.
Constipation-predominant IBS (IBS-C) diagnosis: IBS criteria and 2 or more affirmative answers to Q 4B, Q 8C, Q 9 D-F, Q 10 A-D.
For the diagnosis of alternating IBS (IBS-A), the criteria for IBS and an affirmative answer to Q 4A and B and Q 9A and F were used.
The questions referred to the presence of comorbidity (high blood pressure, diabetes mellitus, chronic liver damage, nephropathy), past surgical history, use of medication at the time of the survey, a family history of IBS diagnosis (parents, brothers or sisters, grandparents, aunts or uncles), tests done because of symptoms, and age at onset of gastrointestinal symptoms.
Sample sizeBecause there were no previous studies reporting IBS prevalence in Chile, the estimate presented at the Latin American Consensus on Irritable Bowel Syndrome, corresponding to a maximum prevalence of 18%, was used to calculate sample size.15 According to the formula used for this calculation, we established a minimum sample size of 391 surveys to reach 80% power and an alpha level of 0.05.
Statistical analysisAll the eligible surveys were given a correlated code number, keeping the identity of the subjects confidential. The STATA 9.0 software was used for the data analysis. Age and IBS presence (with and without the variable of sex) were compared using the Student's t test. The Pearson chi-square test or the Fisher exact test were used to compare the categorical variables. Possible risk factors, such as female sex, a family history of IBS, and occupational level were determined through the logistic regression analysis. Odds ratio was calculated with a 95% confidence interval.
Data were presented as mean ± standard deviation. All the calculations were two-tailed p values and statistical significance was considered with a p<0.05.
Ethics committeeThis study was approved by the Scientific Ethics Committee of the Hospital Clínico Universidad de Chile.
ResultsA total of 437 surveys were taken, corresponding to 191 men and 246 women, with a mean age of 42.8±14.9 and 42.9±14.4 years, respectively, and a range of 15-82 years. One hundred fifty-four subjects (35.2%) stated they had no gastrointestinal symptoms during the time period managed in the survey (Table 1).
Epidemiologic background of the surveyed subjects.
| Total | Asymptomatic | IBS | Other symptoms | p | |
| No. (%) | 437 100 | 154 35.2 | 125 28.6 | 158 36.15 | NS |
| Years: mean±SD | 42.7±14.6 | 41.1±15.5 | 45.2±15.2 | 42.5±13.0 | NS |
| Age range | 15-82 | 15-71 | 17-82 | 18-81 | NS |
| Sex M/W(%) | 191/246 43.7 56.3 | 88/6657.1 42.9 | 43/8234.4 65.6a | 60/9838 62.0b | 0.001a0.001b |
| No. (%) | No. (%) | No. (%) | No. (%) | p | |
| Area of residence | |||||
| 1 | 122 (100) | 60 (49.2) | 35 (28.6) | 27 (22.1) | NS |
| 2 | 48 (100) | 12 (25.0) | 9 (18.7) | 27 (56.3) | NS |
| 2 | 53 (100) | 10 (18.9) | 14 (26.4) | 29 (54.7) | NS |
| 4 | 87 (100) | 34 (39.0) | 23 (26.5) | 30 (34.5) | NS |
| 5 | 127 (100) | 38 (30.0) | 44 (34.6) | 45 (35.4) | NS |
| Educational level | |||||
| 1 | 98 (100) | 47 (48.0) | 15 (15.3)c | 36 (36.3) | <0.01c |
| 2 | 58 (100) | 26 (44.1) | 19 (32.2) | 14 (23.7) | NS |
| 3 | 78 (100) | 19 (24.4) | 26 (33.3) | 33 (42.3) | NS |
| 4 | 174 (100) | 54 (31.0) | 54 (31.0) | 66 (38.0) | NS |
| 5 | 28 (100) | 8 (28.6) | 11 (39.3) | 9 (32.1) | NS |
| Family history of IBS | 121 (27.6) | 23 (14.9) | 50 (40)d | 48 (30.3) | <0.001d |
Two hundred eighty-three subjects (64.8%) said they had gastrointestinal symptoms. One hundred twenty-five subjects (28.6%) reported symptoms consistent with IBS according to the Rome II criteria. Fifty-three subjects (42.4%) were observed in both the IBS-D and the IBS-C subgroups, and only 19 (15.2%) presented with IBS-A. There were no differences in relation to sex.
The remaining subjects corresponded to a group of patients with heterogeneous symptoms, among which reflux, epigastric pain, and dyspepsia were predominant. Other existing symptoms were not tabulated.
Demographic backgroundUpon comparing the demographic data of the subjects with IBS symptoms and the asymptomatic ones, a greater proportion of women was observed in the IBS group (65.6%), whereas the percentage of women was 42.9% in the asymptomatic subjects. On the other hand, there were no differences in the ages of the patients in the two groups (45.2 years vs-. 41.1 years).
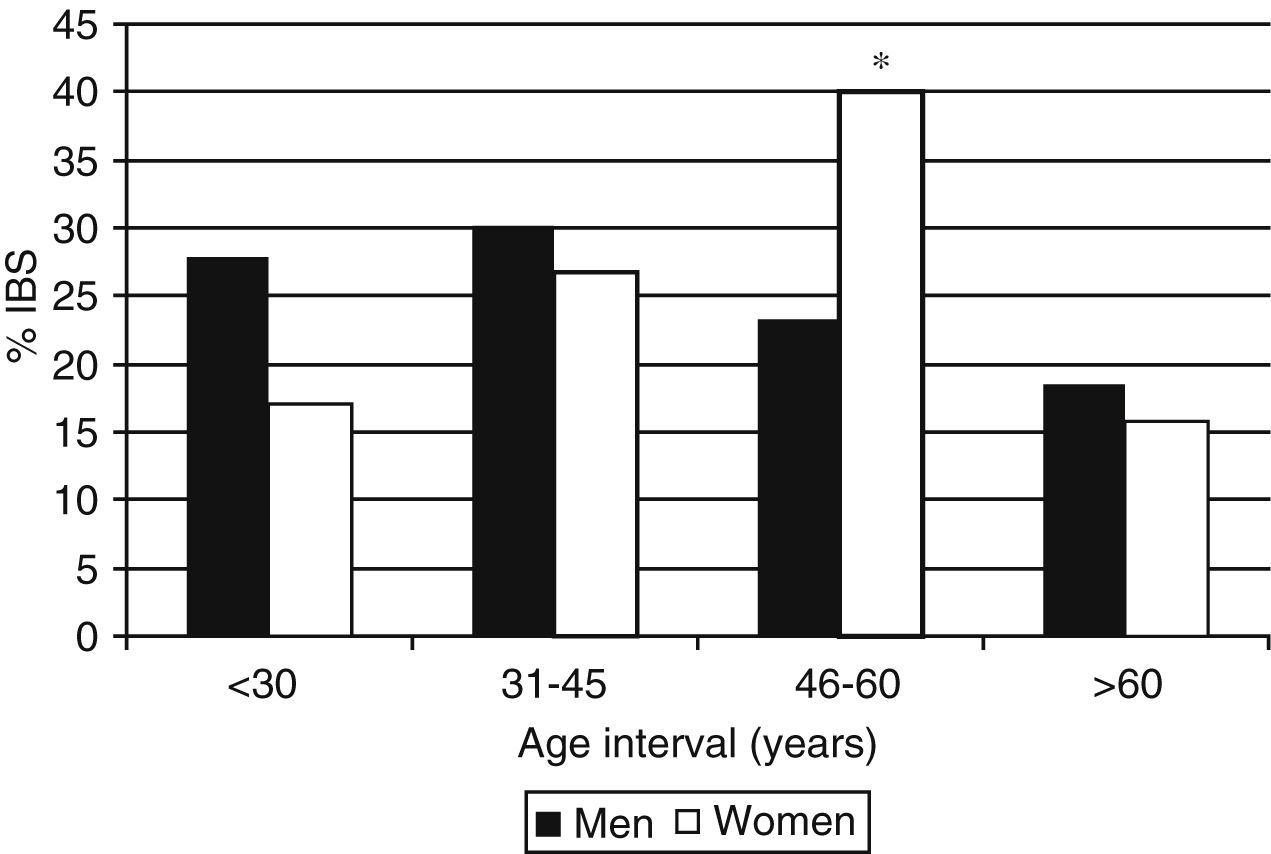
The sex distribution percentage of the different patient ages in the IBS group is shown in Figure 2: the percentage of women patients with IBS symptoms progressively increased with age, reaching a maximum 46-60 years; there were significant differences with men from the same age group and with older or younger women (p<0.05). In contrast, there were no age-related variations in men.
Regarding the educational level (Table 1), the majority of the surveyed subjects, whether presenting IBS symptoms or asymptomatic, were in level 4 (technical studies). When comparing the percentage distribution of the subjects with IBS symptoms and the asymptomatic ones, a lower IBS percentage was seen in the group with a higher level of education; there were no differences in the other groups. In relation to the area of residence, the majority of the subjects lived in areas 1 and 5; there were no differences in the distribution percentage between the subjects with and without IBS symptoms in the different areas of residence (Table 1).
Risk factors for irritable bowel syndromeA family history of IBS was present in 40% of the IBS subjects, whereas only 14.9% of the asymptomatic subjects stated having such a history (p<0.001) (Table 1).
The univariate analysis of the evaluated factors showed that women had a greater risk for IBS, but it was not statistically significant (p=0.057). The presence of family history was significant (p<0.01). Having a university education was associated with a lower presence of IBS symptoms and was statistically significant (p<0.02).
A past history of surgery was found in 107 subjects and the number of surgeries was 108 (38.7%). The most frequent procedures were cholecystectomy, appendectomy, and gynecologic interventions. Table 2 shows that more than twice the number of subjects with IBS underwent cholecystectomy compared with the asymptomatic subjects (p<0.05). This difference was maintained when only women were taken into account. In contrast, appendectomy presented with a similar frequency in both groups.
Clinical data of the subjects with symptoms of irritable bowel syndrome and the asymptomatic subjects.
| Irritable bowel syndrome | Asymptomatic | |
| Surgeries | ||
| Cholecystectomy | 42 (33. 6%)* | 20 (12.9%) |
| Appendectomy | 13 (10.4%) | 19 (12.3%) |
| Gynecologic surgery | 7 (5.6%) | 0 |
| Others | 4 (3.2%) | 3 (1.9%) |
| Total | 66 (52.8%)* | 42 (27.2%) |
| Concomitant Pathologies | ||
| High Blood Pressure | 28 (22.4%)* | 19 (1.3%) |
| Diabetes Mellitus | 14 (11.2%)* | 6 (3.8%) |
| Others | 20 (16%)* | 9 (5.8%) |
| Total | 62 (49.6%)* | 34 (22.07%) |
A very low proportion of other surgical procedures was observed in the two groups.
In the concomitant pathology analysis (Table 2), high blood pressure and diabetes mellitus stood out and their frequency was significantly greater in the patients with IBS symptoms (p<0.05).
The mean age for IBS symptom onset was 30.4 years, with a range of 11 to 69 years.
Forty-nine (39.2%) of the subjects with IBS had seen a physician. Of those subjects, tests were ordered for 28 of them; the most frequent was endoscopy, performed in 13 of the subjects, blood tests in 8, abdominal ultrasound in 4, and abdominal ultrasound plus endoscopy in 3 subjects.
Of the 49 subjects with IBS that had a medical consultation, 37 (75.5%) reported having received some kind of treatment for their symptoms (Table 3) and the most frequently used drug was a proton pump inhibitor in 35.1% of the cases.
DiscussionOur results showed a high frequency of gastrointestinal symptoms in a population visiting large shopping malls in different areas of Santiago (64.8%). Of those subjects, 28% presented with symptoms that were consistent with IBS according to the Rome II criteria. The remaining clinical manifestations could not be adequately evaluated due to the fact that the survey only included questions from the Rome II criteria for defining IBS.
General characteristicsIn Latin America, a prevalence of IBS between 9 and 18% has been described,15 which is similar to that reported for the Hispanic population in the United States.17
In Europe, a telephone survey encompassing a large number of participants, revealed an overall prevalence of 11.5%; it was higher in Italy and in the United Kingdom.18 A survey of 5,000 patients in the United States reported a 14.1% prevalence.19 Two recent studies in Mexico showed an IBS prevalence of close to 16%,20,21 in Colombia a somewhat higher figure of 19.9% was reported,22 and in Uruguay this prevalence was 10.9%.23
In Chile, a survey was applied to Chilean gastroenterologists in which they were asked if they thought they presented with IBS. There was an affirmative response in 22% of those surveyed.24
From the data obtained in the present study, we can say that the population visiting shopping malls in different areas of Santiago has a high prevalence of IBS symptoms at 28.6%, one of the highest in the world, similar to that observed in Nigeria.25
It is difficult to establish the factors that could be related to this greater IBS prevalence in Chile. Unlike other pathologies, such as cholelithiasis, the ethnic factor does not seem to be relevant, given that a recent communication26 reported a prevalence of 22% in a rural mapuche population, only slightly lower than the figure observed in the present study. Taking into account that there are no previous studies that would enable variability over periods of time to be established in relation to IBS prevalence, it can only be speculated that the very relevant socioeconomic changes have been the main variant in the last decades in the Chilean environment.
Age at the time of onset is within the ranges that have been established in other studies, even though this variable is not clearly defined in the main studies.27–29 A mean of 42 years has been estimated in Latin America.15
Regarding the IBS-D and IBS-C subgroups, the low prevalence in our study of the alternating group in which both symptoms are present is striking, compared with that observed in a European study in which this presentation form was observed in 63% of the cases.18 Nevertheless, the results observed in different reviews indicate much variability in this respect in the different populations studied, a fact that is partially dependent on the methodology employed for establishing the diagnosis.18,27,28
Risk factorsAs reported in other studies, a higher prevalence of IBS symptoms was associated with women30 and with the age group of 46-60 years in the present study; statistical significance was not reached in relation to the total group participating in the survey.
It was interesting that the group with the highest educational level presented with a significantly lower percentage of IBS symptoms; there are no articles in the literature that directly analyze this factor. One study suggests that a lower socioeconomic level and a higher level of anxiety are associated with a greater IBS prevalence.31 However, the socioeconomic factor did not seem to have a direct relation in our study, given that the distribution in relation to areas of residence that could have very different populations, was similar in this aspect. It is possible that the educational level per se could be conducive to a better adaptation to the symptoms.
A total of 40% of the subjects with IBS symptoms had a family history of the same pathology, compared with 14.9% of the asymptomatic subjects. This was an important distinctive factor between the two groups, and similar observations have been made in other studies.32,33
The interpretation of these data is complex. Some studies strongly suggest a familial influence; children whose parents present with IBS have been shown to have a higher number of medical consultations.34 Evidence supporting a genetic factor is based on studies that show a greater concordance in monozygotic twins, compared with dizygotic twins,35,36 but this finding has not been confirmed in all the studies.37
Different investigations have associated IBS with the polymorphism of the serotonin transporter, IL-10, the cholecystokinin receptor, and others.37,38
Medical impactWhen analyzing the characteristics of the group of patients with IBS, it should be taken into account that a percentage of them probably are organic pathology carriers, especially those of the IBS-D group. Their evaluation could lead to establishing other diagnoses such as: microscopic colitis, celiac disease, and inflammatory bowel disease. The percentage of organic pathology with these characteristics that could be present in this group of patients was not analyzed in the present study.
Some studies have reported a greater number of surgeries in IBS patients,27,39 especially cholecystectomy, but also appendectomy and gynecologic surgery, and this phenomenon was also observed in our survey.
It is interesting that 33.6% of the subjects with IBS had undergone cholecystectomy, compared with 13% of the asymptomatic subjects. This proportion was maintained only in the analysis of the female patients. It is possible that the presence of gastrointestinal symptoms in patients with IBS is a determining factor in a more frequent diagnosis of cholelithiasis that results in cholecystectomy, even as a prophylactic measure. This is a widely accepted criterion in the Chilean medical environment. The association with organic pathologies such as high blood pressure that do not compromise the gastrointestinal tract is not clear.
The percentage of patients that visited a physician was similar to that described in another study.28 It is conspicuous that the majority of the tests done (upper gastrointestinal endoscopy) and the therapy administered (proton pump inhibitors) had little relation to the symptoms the patients most likely described to their attending physicians; this can have an important economic impact on local health organizations.40
It is possible that, depending on the respective speciality of the attending physician, fewer diagnostic criteria of functional gastrointestinal disorders, in accordance with the symptoms reported by the patient, are employed. As a result, a greater difference between the question asked by the attending physician and the interpretation of the patient's response would be observed.
In conclusion, according to the results of our survey, the group being studied presented with one of the highest frequencies of IBS-type symptoms. Even if only some of these patients seek medical attention for their symptoms, the required information and orientation in relation to their adequate management should be reflected in the undergraduate study programs in general medicine and in the postgraduate courses for specialists.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there was no conflict of interest.
Please cite this article as: Madrid-Silva AM, et al. Prevalencia de síntomas de intestino irritable en población asistente a centros comerciales de Santiago de Chile. Revista de Gastroenterología de México. 2013;78:203–210.

