
A strong genetic association between celiac disease (CD) and the human leukocyte antigen (HLA) has been widely demonstrated. In Europe, the HLA-DQ2 allele is predominant. However, studies in Latin America indicate that HLA-DQ8 could be more frequent. In Mexico, the frequency of those alleles has not been reported in subjects with CD. Therefore, the aim of the present study was to evaluate the distribution of HLA-DQ2 and HLA-DQ8 in Mexican individuals with CD.
Material and methodsAn exploratory study was conducted on a cohort of 49 subjects with chronic diarrhea. Autoantibodies for CD, duodenal atrophy, and HLA haplotypes were determined.
ResultsThirty individuals had CD (23 women, mean age 54.2 ± 15.5 years), 24 (80%) of whom expressed HLA-DQ8, 15 (50%) expressed HLA-DQ2, and 11 (37%) presented with both alleles. However, neither the HLA-DQ2 nor the HLA-DQ8 allele was found in 5 (10%) individuals. In subjects with chronic diarrhea that did not have CD, 12 (63%) presented with HLA-DQ2, and 7 (37%) with HLA-DQ8. Individuals with CD expressed the combinations of the HLA-DQ8/DQ2 alleles (37 vs. 5%) and the HLA-DR4/DQ8 alleles (60 vs. 26%) more frequently than the subjects without CD.
ConclusionsIn Mexican subjects with CD, HLA-DQ8 distribution was more frequent than that of HLA-DQ2, indicating a possible similarity to the frequency reported in other Latin American countries. However, given the nature of the present study and its sample size, further conclusions could not be reached.
Existe una fuerte asociación entre la enfermedad celiaca (EC) y el antígeno leucocitario humano (HLA). En Europa predomina el alelo HLA-DQ2; sin embargo, estudios en América Latina indican que el HLA-DQ8 podría ser más frecuente. En México no se ha reportado la frecuencia de estos alelos en sujetos con EC. Por lo tanto, el objetivo de nuestro estudio fue determinar la distribución de HLA-DQ2 y HLA-DQ8 en sujetos mexicanos con EC.
Material y métodosSe llevó a cabo un estudio exploratorio con una cohorte de 49 individuos, en quienes se buscó la presencia de marcadores serológicos, histológicos y genéticos de la EC.
ResultadosTreinta sujetos (23 mujeres) con una edad promedio de 54.2 ± 15.5 años presentaron EC; 24 (80%) de ellos expresaron HLA-DQ8 y 15 (50%) HLA-DQ2; 11 (37%) presentaron ambos alelos; sin embargo, en 5 (10%) individuos no se encontró HLA-DQ2 ni HLA-DQ8. Entre los sujetos con diarrea crónica que no tuvieron EC, 12 (63%) presentaron HLA-DQ2 y 7 (37%) HLA-DQ8. Los sujetos con EC expresaron más frecuentemente la combinación de HLA-DQ8/DQ2 (37% vs. 5%) y los alelos HLA-DR4/DQ8 (60% vs. 26%).
ConclusionesEn sujetos mexicanos con EC la expresión de HLA-DQ8 fue más frecuente que la de HLA-DQ2, lo cual indica que la distribución de HLA podría ser similar a las descritas en otros países de América Latina. Sin embargo, la naturaleza y el tamaño de la muestra de este estudio no permiten hacer más conclusiones.
Celiac disease (CD) is one of the most common food-related intestinal disorders. This condition is characterized by an abnormal immune response to the ingestion of gluten and related proteins in genetically susceptible individuals that have a polygenic disorder, with the participation of both human leukocyte antigen (HLA) genes and non-HLA genes.1 HLA-DQ2 and HLA-DQ8 are the most frequent, and the DQA1*05/DQB1*02 heterodimer is observed in 90-95% of the cases.2
In most European subjects with CD, HLA-DQ2 is more prevalent,3,4 but that same assumption remains controversial for Latin American populations. For instance, in a study conducted on pediatric and adult Amerindian subjects with CD, there was a higher frequency of HLA-DQ8.5–7 In addition, the authors of a population-based study carried out in different regions of Mexico found a distribution of 16% for HLA-DQ2 and 24% for HLA-DQ8,8 suggesting that the Mexican population could share some of the characteristics found in other Latin American countries.
The diagnostic criteria for CD include the combination of positive serologic auto-antibodies, such as anti-endomysium (EmA IgA), anti-transglutaminase (anti-tTG IgA/IgG), and anti-deamidated gliadin peptide (AGA-DGP IgA/IgG), together with the histologic demonstration of villous atrophy of the second part of the duodenum.9,10 However, in certain clinical situations, it is recommended to investigate the presence of HLA-DQ2/DQ8 to rule out the disease.9
In Mexico, the frequency of CD is similar to that described worldwide,11 but the distribution of HLA-DQ8/DQ2 in subjects with CD has not been reported. Therefore, the aim of the present study was to determine the distribution of the HLA-DQ2 and HLA-DQ8 alleles in Mexican subjects with CD.
Materials and methodsAn exploratory study was conducted on 49 consecutive Mexican patients (38 women) with a mean age of 53 ± 14.5 years with chronic diarrhea (watery or loose stools for more than four weeks) and symptoms consistent with CD that were seen at the outpatient unit of a tertiary care referral center in Mexico City.
The study subjects underwent blood chemistry screening tests, serum levels of anti-tTG IgA/IgG and EmA IgA (INOVA Diagnostics, Inc., San Diego, CA, USA), stool analysis for parasites, and stool cultures. The individuals were also studied under the institutional protocol for chronic diarrhea, in which malabsorption is a serum beta-carotene level lower than 60μg/dl in females, and 50μg/dl in males, values consistently related to significant steatorrhea (stool fat 10g/d). In individuals with steatorrhea, a D-xylose absorption test in urine was performed (normal > 5g/vol).12
All the individuals had upper gastrointestinal endoscopies and duodenal aspirates, and at least four fragments of the second part of the duodenum were taken for analysis. Histologic findings were classified according to the Marsh-Oberhuber criteria,13 and CD was diagnosed through compatible intestinal biopsy histology (Marsh II-IV), and positive antibody tests (tTg-IgA/IgG/ EmA IgA). Small intestinal bacterial overgrowth (SIBO) was defined when bacterial populations in the small intestine exceeded 105-106 organisms/ml.14
Class II antigens (HLA-DRB1, HLA-DQB1) were typed by the PCR-SSP procedure (Pel-Freez HLAA/B/DR/DQ SSP Unity, Brown Deer, Wisconsin, USA), and the HLA-DQ8 allele was determined as a generic category (broad antigen).
A Mexican mestizo was defined as a person born in Mexico, whose last two ascending generations were also born in Mexico. Demographic data were collected, and the patients were classified into two groups: group A, patients with celiac disease and group B, patients with chronic diarrhea from other causes. The physicians that classified the patients were blinded to the results of the HLA analysis.
All participants signed written statements of informed consent and the study was approved by the Institutional Review Board for Biomedical Studies on Humans Beings (ref. 1719).
Statistical analysisThe distribution of the HLA-DQ2 and HLA-DQ8 alleles was reported. The frequencies were compared between patients with CD and those with chronic diarrhea from other causes, but no statistical comparisons were performed between the 2 groups.
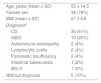
ResultsThe demographic characteristics are shown in Table 1. The diagnosis of CD was established in 30 subjects (23 women) with a mean age of 54.2 ± 15.5 years. In the rest of the individuals, SIBO was the most common diagnosis (15 women), mean age 50.7 ± 12.5 years).
Characteristics of the study subjects.
| Age, years (mean ± SD) | 53 ± 14.5 |
| Female sex | 38 (78%) |
| BMI (mean ± SD) | 21 ± 4.6 |
| Diagnosisa | |
| CD | 30 (61%) |
| SIBO | 10 (20%) |
| Autoimmune enteropathy | 2 (4%) |
| Lymphocytic colitis | 2 (4%) |
| Pancreatic insufficiency | 2 (4%) |
| Intestinal tuberculosis | 1 (2%) |
| IBS-D | 1 (2%) |
| Without diagnosis | 5 (10%) |
CD: Celiac disease; IBS-D: Irritable bowel syndrome-diarrhea; SIBO: Small intestinal bacterial overgrowth.
The expression of HLA-DQ2 was similar between the 2 study groups (50% vs. 63%), but HLA-DQ8 was more frequent in patients with CD (80% vs. 37%). The frequency of HLA-DQ8 persisted after including the prevalence of HLA-DR4/DQ8 haplotype, and the combination of both HLA-DQ2 and HLA-DQ8 was more frequent in subjects with CD (37% vs. 5%).
Discussion and conclusionsThe present study is the first to measure the frequency and distribution of the HLA-DQ2 and HLA-DQ8 alleles in a Mexican population with CD. Our results are similar to observations made worldwide, regarding the high frequency of the HLA-DQ2 and HLA-DQ8 haplotypes in subjects with CD. However, unlike most of the European populations, the subjects with CD from our study expressed the HLA-DQ8 haplotype more frequently. That same association was previously described in other South American individuals with CD,6,15 coinciding with the high prevalence of HLA-DQ8 previously reported in Mexican mestizo subjects.16 On the other hand, the frequency of the HLA-DQ8 haplotype was interestingly low in individuals with chronic diarrhea without CD, which was also the case when the DR4/DQ8 haplotype presented. In general, an unexpectedly high prevalence of HLA-DQ2 was found, being even higher than the frequency of HLA-DQ2 reported by Barquera et al.8 in the general Mexican population.
The most frequent diagnosis in the group of chronic diarrhea from other causes was SIBO, and subjects became asymptomatic after receiving specific treatment.14–17 In 5 (10%) cases no diagnosis was established, and seronegative CD was ruled out because its presence was not supported by histologic findings or response to a gluten-free diet.
Regarding the limitations of the present study, the small sample size did not allow stronger assumptions to be made. However, ours is the first exploratory research analyzing the distribution of the HLA-DQ2 and HLA-DQ8 alleles in Mexican individuals with CD. It is also the first report to suggest that the HLA-DQ8 allele and DR4/DQ8 haplotype could be more prevalent than HLA-DQ2 in Mexican individuals with CD, supporting the findings of other Latin American populations. Finally, it is important to emphasize that, given the nature of the present study and its small sample size, the results obtained must be further evaluated.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Cerda-Contreras E, Ramírez-Cervantes KL, Granados J, Mena L, Núñez-Álvarez C, Uscanga L. ¿Es posible una mejor identificación de la enfermedad celiaca en sujetos mexicanos por medio de HLA-DQ8 que de HLA-DQ2? Revista de Gastroenterología de México. 2018;83:410–413.

