
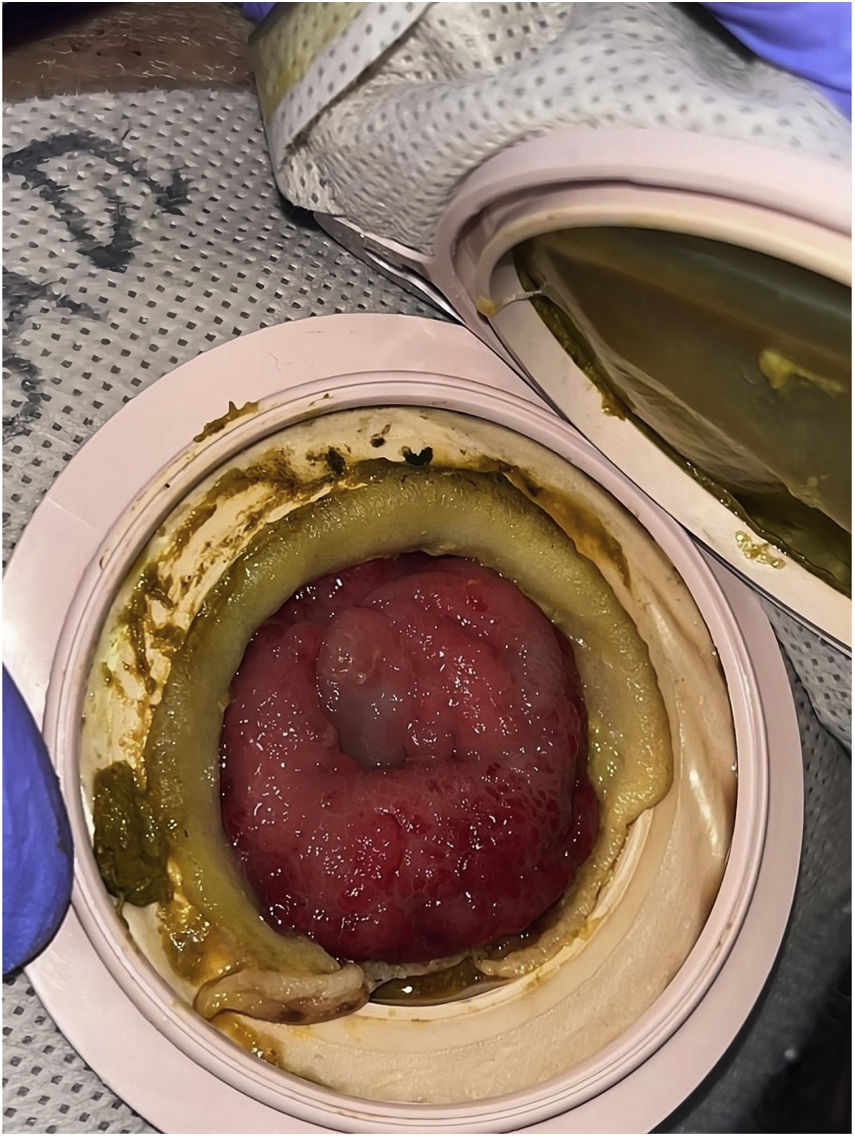

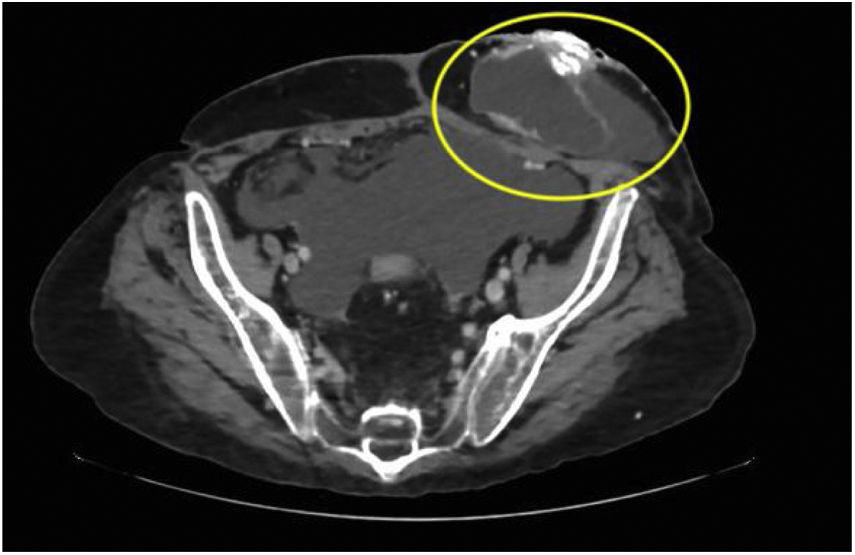
A 64-year-old man underwent a colectomy in 2018 secondary to intestinal occlusion due to colon cancer. In addition, he presented with a history of cirrhosis of the liver secondary to metabolic dysfunction-associated steatotic liver disease. He came to the emergency department due to acute bleeding at the stoma site. Physical examination was unremarkable and laboratory tests reported anemia. Vascular tracts with evidence of recent bleeding through the edges of the stoma, which bled easily, were observed (Fig. 1). Cyanoacrylate was directly injected into the stoma, achieving hemostasis with no complications (Fig. 2). A control computed tomography scan showed the cyanoacrylate in the stoma (Fig. 3).



Bleeding due to peristomal varices is a rare complication in patients with a stoma (3-5%). It generally presents in cases with cirrhosis of the liver but, as with other ectopic varices, it is more common in patients with prehepatic portal hypertension. Treatment includes endoscopic sclerotherapy, variceal banding, transjugular intrahepatic portosystemic shunt placement, and retrograde transvenous obliteration. The choice of treatment strategy is dependent on bleeding severity. Endoscopic treatment is generally preferred for patients with mild-to-moderate bleeding, whereas transjugular intrahepatic portosystemic shunt placement is reserved for patients with severe bleeding, and retrograde transvenous obliteration is performed, when a transjugular intrahepatic portosystemic shunt is contraindicated.

