
We studied the epidemiology of functional gastrointestinal disorders (FGIDs) in school-aged Salvadoran children using standardized diagnostic criteria.
AimsTo determine the prevalence of FGIDs in school-aged children in El Salvador.
Material and methodsA total of 395 children participated in the study (one public school and one private school). School children completed the Spanish version of the Questionnaire on Pediatric Gastrointestinal Symptoms–Rome III (QPGS-III), an age-appropriate and previously validated instrument for diagnosing FGIDs according to the Rome III criteria. Sociodemographic (age, sex, type of school) and familial (family structure and size, family history of gastrointestinal disorders) data were obtained.
ResultsThe mean age of the sample was 11.8 years±1.6 SD (median 10, range 8-15) and 59% of the participants were female. Eighty-one children met the diagnostic criteria for a FGID (20%). Defecation disorders were the most common group of FGIDs. Functional constipation was diagnosed in 10% of the children and 9.25% were diagnosed with abdominal pain-related FGIDs (most commonly IBS, 3.75%). IBS overlapped with functional dyspepsia in 11% of the cases. Children with FGIDs frequently reported nausea. Children attending private school and older children had significantly more FGIDs than children in public school and younger children.
ConclusionsFGIDs are common in school-aged Salvadoran children.
La epidemiología de los trastornos funcionales gastrointestinales en niños salvadoreños en edad escolar usando criterios diagnósticos estandarizados no se ha estudiado.
ObjetivosDeterminar la prevalencia de trastornos funcionales gastrointestinales en niños salvadoreños en edad escolar.
Materiales y métodosTrescientos noventa y cinco niños participaron en el estudio (una escuela pública y una privada). Se utilizó el Questionnaire on Pediatric Gastrointestinal Symptoms-Rome III (QPGS-III) traducido al español, que es un instrumento apropiado para el uso en este grupo de edad y que ha sido validado. Se recolectó información acerca de variables socio-demográficas (edad, sexo, tipo de escuela) y familiares (tamaño y estructura familiar, historia familiar de trastornos funcionales gastrointestinales).
ResultadosLa edad promedio fue 11.8 años±1.6 SD (media 10, rango 8-15), y el 59% fueron mujeres. Ochenta y un niños cumplieron criterios diagnósticos de trastorno gastrointestinales funcionales (20%). El estreñimiento fue el diagnóstico más frecuente y fue diagnosticado en 10% de niños. El 9.25% de los niños fueron diagnosticados con trastornos funcionales gastrointestinales asociados a dolor abdominal (el más común fue síndrome de intestino irritable, 3.75%). Hubo sobreposición de diagnóstico entre síndrome de intestino irritable y dispepsia funcional en 11% de los casos. Los niños con trastornos funcionales gastrointestinales reportaron mayor porcentaje de nausea. Los niños en escuelas privadas y niños mayores de 12 años demostraron mayor porcentaje de trastornos funcionales gastrointestinales que niños en escuelas públicas y niños menores de 12 años.
ConclusionesLos trastornos funcionales gastrointestinales son comunes en niños salvadoreños en edad escolar.
Functional gastrointestinal disorders (FGIDs) are among the most common problems in children and adults. FGIDs are a worldwide problem. Studies from the US,1–4 Germany,5 China,6 and Colombia7 have found a high prevalence of FGIDs in school-aged children. Children with FGIDs have a poor quality of life and higher levels of anxiety and depression.8 FGIDs in children have long-lasting effects with a high proportion of children continuing to complain of gastrointestinal and psychological disturbances as adults.9,10
The pathogenesis of FGIDs is not yet fully understood. It has been proposed that FGIDs are a result of the interplay of multiple factors including genetics, the microbiome, and environmental and psychosocial elements. Irritable Bowel Syndrome (IBS) is one of the common FGIDs, and its definition includes changes in stool consistency, as well as the symptoms of chronic intermittent abdominal pain. A meta-analysis has shown an increased risk of IBS in Asian patients thought to be associated with the presence of specific genetic mutations.11 Recent studies have measured cytokines in adults and children with IBS in Mexico.12 It is still unclear whether cytokines and genetic variations could explain the differences in prevalence of FGIDs among regions. Identifying the relative influence of each of these factors would help advance the understanding of the pathogenesis and pathophysiology of FGIDs.
Epidemiological studies using validated diagnostic instruments and common methods make comparisons among regions possible. The comparative analysis of regional differences in prevalence and the infectious, social, environmental, dietary, and cultural characteristics of each region provides a unique opportunity to study the relative influence of each of the factors involved in the biopsychosocial model. Epidemiological studies are of utmost importance for public healthcare planning. Regional prevalence studies are an aid to efficient healthcare planning by allowing a targeted use of scarce healthcare resources. A better understanding of the various factors that predispose children to develop FGIDs could also lead to a novel approach to this public health problem in the form of primary and secondary prevention. Establishing early preventive measures could result in a shift in the current paradigm of FGID care with potential implications for children and adults.
In the past, we have translated and validated the Questionnaire of Pediatric Gastrointestinal Symptoms (QPGS) into Spanish13 and conducted epidemiological studies on school children in the US3 and South America,7 using a common methodology. To the best of our knowledge, this is the first study to be published on the epidemiology of FGIDs in school children in Central America.
The main aim of this study was to determine the prevalence of FGIDs in school-aged children in El Salvador.
MethodsThe study was conducted in June and July 2014 in the city of San Salvador, the capital of El Salvador, and included children from a public school and a private school. El Salvador is the most densely populated country of Central America with an extension of 21,000km2. San Salvador is the largest city in El Salvador with a population of 567,698 inhabitants (approximately 10% of the country's population).14,15 Racial makeup is largely mestizo (86%) with a smaller percentage of white/creole individuals.16 San Salvador has a tropical wet and dry climate and is warm all year round.17 The latter is important since the prevalence of FGIDs may be influenced by seasonal changes.18,19
The study followed the methodology used in previous and ongoing studies by our group, Functional International Digestive Epidemiological Research Survey (FINDERS), an international collaborative group established for the purpose of conducting epidemiologic studies in children from Latin America.7,20 FINDERS is led by some of the authors of this study (CAV, MS), who collaborate on the conceptualization, design, planning, and execution of the studies. The design of the investigations conducted by FINDERS is based on previous school studies in the US.1,3 The methods were adapted and then tested on Latin American children. A detailed description of the methods of the study is available elsewhere.7 In short, an invitation package including a consent form to participate in an epidemiological study was mailed to the families of all the children in grades four through six. Children that were included in the study had no history of organic medical conditions and agreed to participate. Spanish is the official language and the language spoken by virtually all residents in San Salvador, therefore a Spanish version of the QPGS–Rome III Version (QPGS-III) was utilized.13,21,22 The same version of the instrument was used in studies conducted in Colombia7 and Ecuador20 by FINDERS. To ensure their comprehension, the investigators reviewed the questionnaire with the children through an audiovisual presentation before its completion. Investigators were also available to answer questions while the participants completed the questionnaire. Parents provided information regarding the past medical history and the sociodemographic (age, sex, type of school) and familial (family structure and size, family history of gastrointestinal disorders) variables of the participants. Ten percent of the records were reviewed and compared with the original forms to detect any possible transcriptional errors. The National Ethics Committee of Clinical Research of El Salvador approved the study.
Statistical AnalysisPrevalence data were pooled from the 2 schools for the initial analysis. Data were analyzed using the 2-sided Student's t test, chi-square test, and Fisher exact test, where appropriate (Stata 10 software; StataCorp, College Station, Texas). To evaluate possible risk factors for FGIDs, the univariate analysis with OR calculation and the logistic regression analysis were performed between each of the exposure variables of interest: the sociodemographic variables (age, sex, type of school), the familial variables (family structure and size, family history of gastrointestinal disorders), and the effect variable (presence or absence of FGIDs). P values of less than 0.05 were considered statistically significant.
ResultsA total of 434 children were invited to participate. Thirty-five children were excluded from the study due to the presence of organic disease (gastritis, Hirschsprung's disease, gastroesophageal reflux disease, among others). There was no significant difference in age or sex between the children that participated in the study (n = 399) and those that were excluded from the study.
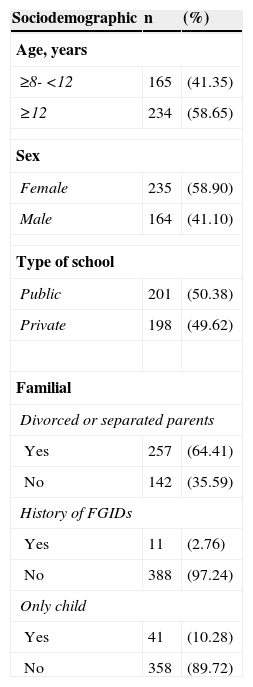
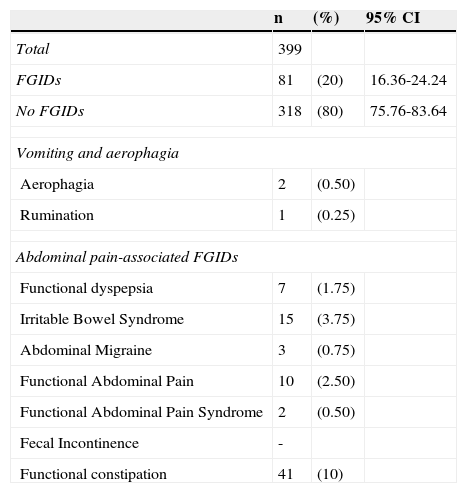
Participants had a mean age of 11.8 years ± 1.6 SD (median 10, range 8-15); 58.6% were 12 years old or older and 59% were female. Parents of participants were divorced or separated in 64% of cases (Table 1). Eighty-one children (20%) met the Rome III diagnostic criteria for a FGID. Mean age for this subgroup was 11.7 ± 1.7 years (range 8-14 years) and 46 were female (56.8%). Defecation disorders were the most common group of FGIDs (functional constipation, 10%), followed by abdominal pain-related FGIDs (9.25%) (Table 2). The most common abdominal pain-related FGID was IBS (3.75%). Disorders of vomiting and aerophagia were the least common group of FGIDs (0.75%). Only 0.75% of children were diagnosed with abdominal migraine.
Sociodemographic and familial variables in the study population.
| Sociodemographic | n | (%) |
|---|---|---|
| Age, years | ||
| ≥8- <12 | 165 | (41.35) |
| ≥12 | 234 | (58.65) |
| Sex | ||
| Female | 235 | (58.90) |
| Male | 164 | (41.10) |
| Type of school | ||
| Public | 201 | (50.38) |
| Private | 198 | (49.62) |
| Familial | ||
| Divorced or separated parents | ||
| Yes | 257 | (64.41) |
| No | 142 | (35.59) |
| History of FGIDs | ||
| Yes | 11 | (2.76) |
| No | 388 | (97.24) |
| Only child | ||
| Yes | 41 | (10.28) |
| No | 358 | (89.72) |
Prevalence of FGIDs in school-aged children in San Salvador, El Salvador.
| n | (%) | 95% CI | |
|---|---|---|---|
| Total | 399 | ||
| FGIDs | 81 | (20) | 16.36-24.24 |
| No FGIDs | 318 | (80) | 75.76-83.64 |
| Vomiting and aerophagia | |||
| Aerophagia | 2 | (0.50) | |
| Rumination | 1 | (0.25) | |
| Abdominal pain-associated FGIDs | |||
| Functional dyspepsia | 7 | (1.75) | |
| Irritable Bowel Syndrome | 15 | (3.75) | |
| Abdominal Migraine | 3 | (0.75) | |
| Functional Abdominal Pain | 10 | (2.50) | |
| Functional Abdominal Pain Syndrome | 2 | (0.50) | |
| Fecal Incontinence | - | ||
| Functional constipation | 41 | (10) | |
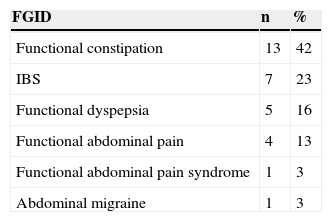
There was frequent overlap among the different FGIDs. Children with IBS had functional dyspepsia in 11% of cases. Based on recent studies that showed a high prevalence of nausea in children with FGIDs,23,24 we investigated the frequency of nausea in this group of school children and found that 79 out of 399 children reported nausea. Nausea was reported by 38% of children diagnosed with FGIDs vs 15% of children not diagnosed with a FGID (p = 0.0075). Almost half of all children with functional constipation had nausea and almost one in 4 children with IBS also presented with nausea (Table 3).
Prevalence of nausea per FGID diagnosisa
| FGID | n | % |
|---|---|---|
| Functional constipation | 13 | 42 |
| IBS | 7 | 23 |
| Functional dyspepsia | 5 | 16 |
| Functional abdominal pain | 4 | 13 |
| Functional abdominal pain syndrome | 1 | 3 |
| Abdominal migraine | 1 | 3 |
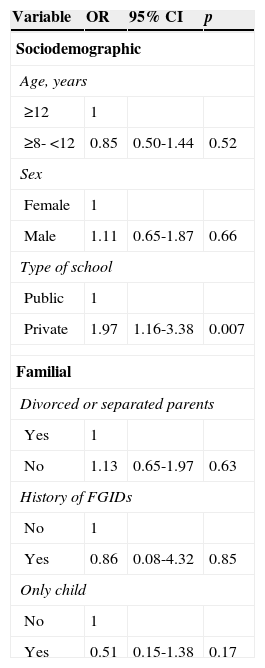
The sociodemographic, familial, clinical, and environmental variables of children with and without FGIDs were compared (Table 4). Multiple regression analysis revealed that age (younger than 12 years) (p = 0.04) and type of school (private) (p = 0.001) significantly contributed to FGID prevalence. Being an only child appeared to have a protective effect, but did not achieve significance.
Relationship between the presence of FGIDs and sociodemographic and familial variables in school-aged children in San Salvador, El Salvador.
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Sociodemographic | |||
| Age, years | |||
| ≥12 | 1 | ||
| ≥8- <12 | 0.85 | 0.50-1.44 | 0.52 |
| Sex | |||
| Female | 1 | ||
| Male | 1.11 | 0.65-1.87 | 0.66 |
| Type of school | |||
| Public | 1 | ||
| Private | 1.97 | 1.16-3.38 | 0.007 |
| Familial | |||
| Divorced or separated parents | |||
| Yes | 1 | ||
| No | 1.13 | 0.65-1.97 | 0.63 |
| History of FGIDs | |||
| No | 1 | ||
| Yes | 0.86 | 0.08-4.32 | 0.85 |
| Only child | |||
| No | 1 | ||
| Yes | 0.51 | 0.15-1.38 | 0.17 |
This is the first study to provide comprehensive data on the prevalence of FGIDs in children in Central America. We surveyed children from 2 schools in San Salvador, the largest city in El Salvador. We included a large number of children from both a private and a public school, which made our sample more diverse and socioeconomically representative of the larger population of El Salvador and enabled group comparison.
Few studies have been published on the prevalence of FGIDs utilizing the latest version of the Rome criteria in children.5,25–28 We have previously described the prevalence of FGIDs in South American children using the Rome III criteria.7,29 In the present study, we found a prevalence of 20%, which is lower than the 29% prevalence found by our group (FINDERS) in school children in Colombia and the 22.8% in Ecuadorian children. Possible explanations for the variation in prevalence include differences in genetic background, diet, microbiome, environment, infectious profiles and psychosocial, cultural, and socioeconomic factors. Although our study was not designed to determine the causes of these epidemiological differences, large prospective studies may help explain our findings. In agreement with our previous study from Colombia, we found that constipation was the most common FGID, IBS was the most common abdominal pain-associated FGID, and that non-retentive fecal incontinence, cyclic vomiting syndrome, rumination, abdominal migraine, and aerophagia occurred in less than 1% of the children. The latter findings contrast with those of 2 epidemiological studies showing a prevalence of abdominal migraine of 23%29 and a prevalence of aerophagia of 7.5%, using the Rome III criteria.30 However, both of these figures are thought to be unexpectedly high and differ from what is commonly seen in our practice and by other members of the FGID community who find those disorders to be rare.
The 10% prevalence of functional constipation found in this study and the 14% prevalence of functional constipation found in 2 previous school studies using self-report questionnaires and the Rome III criteria7,26 are much lower than the 21% prevalence found in children using an older version of the criteria (Rome II).31 These differences in prevalence may be at least partially explained by the use of a different set of diagnostic criteria.32 This assumption is in line with the findings of a retrospective review of charts that applied the Rome II and Rome III criteria to the same cohort of children; it showed significantly more children qualifying for the diagnosis of functional constipation with the Rome II criteria than with the Rome III criteria.32 Considerable changes in the prevalence of FGIDs resulting from the use of different versions of the Rome criteria have also been shown in another study that found a 4-fold increase in abdominal migraine prevalence by applying the Rome III criteria in lieu of the Rome II criteria to the same group of children.29 This underscores the importance of using a common methodology and precise and up-to-date criteria to establish diagnosis.
Children with various FGIDs reported nausea more frequently than their non-FIGD counterparts. Studies have shown that there is a more severe impact on quality of life and a worse prognosis in children that have an abdominal pain-FGID and nausea.23,24 Nausea was also reported in half of the patients with functional constipation. In a group of children with nausea, 13% met the adult Rome III criteria for IBS-C,23 but the association with functional constipation has not previously been reported. To the best of our knowledge, no prior studies have measured the presence of nausea in children with FGIDs in Latin America or in children of Hispanic background in general. Similarly, for the first time, this study investigated the presence of overlap of different FGIDs in Latin-American children and we found that overlap was common. Whether children with overlap of FGIDs have a different prognosis from children that meet criteria for a single FGID is not yet known.
Age and the type of school influenced the prevalence of FGIDs. Older children had a significantly higher prevalence of FGIDs. Children attending a private school were also more likely to report symptoms than children from a lower socioeconomic background. Different psychosocial and behavioral mechanisms may explain this association.
Limitations of our study include the selected population of school children, which may not be representative of the entire pediatric community in El Salvador. Our data were obtained exclusively from the children. Although obtaining additional data from parents would have provided an interesting supplementary perspective to the child's symptoms, we believe that the self-report of symptoms by children mature enough to provide accurate information should be the gold standard, as parents may not be aware of all the child's symptoms33 or may subjectively report them depending on their own personal history or opinion of the importance of the symptoms.
In conclusion, we have found that FGIDs are common in children in El Salvador. Older children and children with a higher socioeconomic status have a greater prevalence of FGIDs. This and other comparative studies expand our knowledge on the epidemiology of FGIDs in children. The epidemiological comparison of the prevalence of FGIDs in children of different ethnicity and race from various countries and migrant communities in their native and adoptive countries may be helpful for understanding the role of genetic, environmental, and cultural factors in the pathogenesis of FGIDs in children.
Ethical responsibilitiesProtection of persons and animalsThe authors declare that no experiments were performed on humans or animals for this study.
Data confidentialityThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.
Doctors Zablah and Velasco-Benítez contributed equally to this work.
Please cite this article as: Zablah R, Velasco-Benítez CA, Merlos I, Bonilla S, Saps M. Prevalencia de trastornos funcionales gastrointestinales en niños en edad escolar en El Salvador. Revista de Gastroenterología de México. 2015;80:186–191.


www.publicationethics.org.