
In 1942 Stout and Murray first described hemangiopericytoma (HPC) as a vascular tumor composed of Zimmerman's pericytes.1 In 1980 Wagner made the first histologic description of a solitary fibrous tumor (SFT) in the pleura,2 and in 1931 Klemperer and Rabin recognized it as a distinctive entity.3 Ultra-structurally, both the HPC and the SFT show variable characteristics of pericytic, fibroblast, and/or myofibroblast differentiation.4
Thanks to the exponential increase in the reports on SFT, the conclusion was reached that it did not only present in serous membranes.5 Currently, due to the superposition of the main histologic characteristics and the lack of specific criteria for determining whether a lesion is SFT or HPC, pathologists have decided to abandon the term HPC in favor of SFT.6
Localized SFT in the small bowel mesentery is an extremely rare tumor, with only 3 cases reported on in PubMed.7–9 The aim of presenting this case was to provide current knowledge about SFT classification and to report the 4th case of SFT in the small bowel mesentery.
An 82-year-old man was brought to the emergency room of the Hospital Nacional Guillermo Almenara Irigoyen (HNGAI) by his relatives for medical attention due to 10 days of colicky abdominal pain that increased in intensity as the days went by; he also presented with nausea, vomiting, fever of 40°C, and sensory disorder. During a thorough anamnesis, the patient stated he had experienced similar symptoms 4 months earlier, associated with dyspepsia and involuntary weight loss of 3kg at that time. Physical examination showed mild paleness, moderate pain upon palpation of the right hypochondrium, mesogastrium, and hypogastrium. In addition, a 15 x 15cm painful mass was palpated in the hypogastrium, while the rest of the physical examination was unremarkable.
A bowel transit time test indicated delayed transit, discreet dilation of the jejunoileal segments, and signs of flocculation with no intramural images. A contrast-enhanced abdominal tomography scan revealed an expansive lesion with hypervascularity that was in contact with the distal ileum, associated with an alteration in the surrounding adipose tissues, and signs of hemoperitoneum predominating in the pelvic cavity recesses. The efferent venous drainage that was dependent on the mesenteric veins, whose diameters were enlarged, was striking, and the diagnostic imaging service recommended considering hemangioma, hemangiosarcoma, carcinoid tumor, hemangiopericytoma, and stromal tumor in the differential diagnoses.
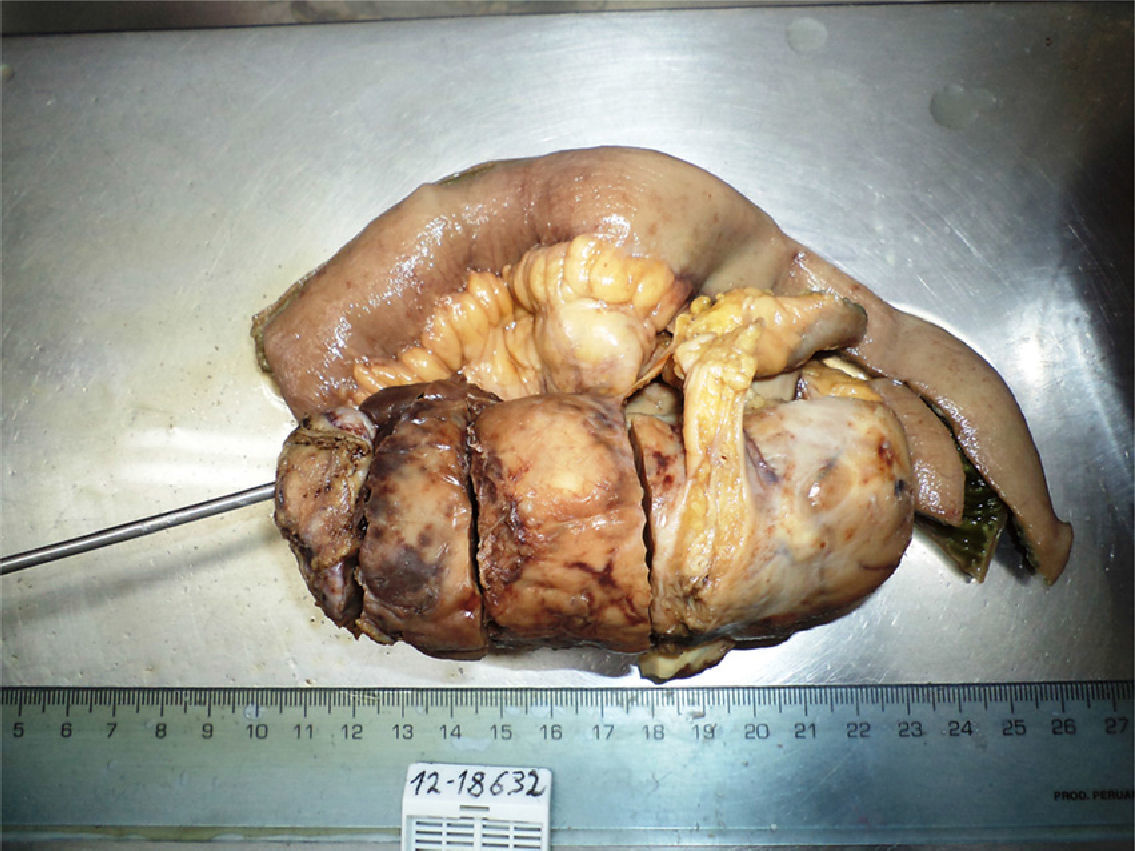
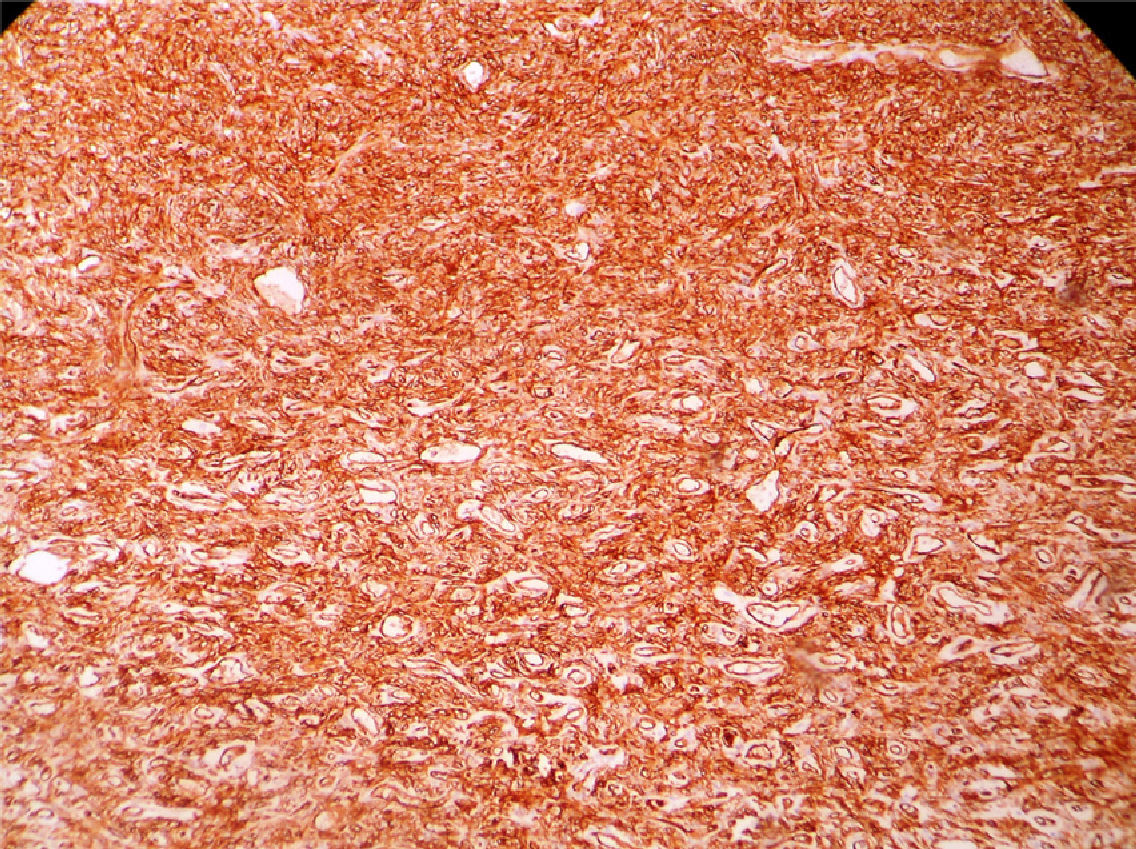
As a result of the discussion of the clinical cases of the coloproctology service of the HNGAI, an exploratory laparotomy+resection of the tumor of the distal ileum and mesentery+ileoileal anastomosis was performed. The macroscopic anatomopathologic study reported a 21cm small bowel segment, a mildly congestive serosa with a 13 x 5 x 4.5cm tumor formation at the level of the mesentery (fig. 1). The conclusion was aggressive HPC of high intermediate risk. The tumor measured 13cm at its largest diameter and presented with zones of necrosis and hemorrhage. The mitotic index was less than 1 in 10 per high power field (HPF), and there was no pleomorphism or atypia. The tumor was confined to the mesentery of the small bowel-ileum and there was no intestinal involvement. The small bowel and its section edges showed no evidence of malignancy. The edge of the mesenteric section corresponded to the tumor's cleavage plane. CD 34 (+), CD 99 (+), CD 31 (−), CD 117 (−), S-100 (−), Actin (−) (fig. 2).

.")
If the SFT appears in the small bowel mesentery it is called extrapleural SFT or peritoneal SFT. The mean presentation age is 54 years, with a slight predominance in men. The 3 reported cases were 26, 53, and 71-year-old patients.7–9 Its clinical manifestation spectrum depends on the size and location of the tumor. The definitive diagnosis is made through immunohistochemistry, in which SFT displays a strong and diffuse stain for CD 34, vimentin, and bcl-2. It is rarely positive for actin, desmin, protein S-100, and cytokeratins.4
There is no clear connection between this tumor's morphology and result, given that SFT behavior is unpredictable. Twenty percent of SFTs possess a malignant variant characterized by large tumor size (more than 5cm in diameter), by being hypercellular and invasive, with nuclear pleomorphism, tissue necrosis, and having a high mitotic index greater than 4 mitoses per 10 HPF. All SFTs have the potential to become malignant, and so a systematic mitosis count is recommeded.6
In our case the SFT presented with malignant characteristics such as large size (a diameter larger than 13cm) associated with necrotic zones, as well as good outcome particularities, such as an absence of pleomorphism and invasion and a mitotic index of 1 per 10 HPF. The patient was released on the 12th postoperative day with a favorable recovery.
In conclusion, the majority of SFTs present with CD 34 (+), CD 99 (+), and CD 117 (−), as in our case. However, 66% of gastrointestinal stromal tumors (GIST) also express CD 34 (+), with the characteristic that 95% of the cases are CD 117 (+). Knowing that a CD 117 (−) stain is the best marker for distinguishing between SFT and GIST provides the ideal manner for differentiating them.10
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Chiroque L, Arenas J, Luyo-Rivas A. Tumor fibroso solitario confinado en el mesenterio del intestino delgado (íleon). 2013;78:259–260.

