







The treatment for celiac disease is a gluten-free diet that should be strictly and permanently carried out. Our aims were to determine adherence to the gluten-free diet and the risk factors for non-adherence.
Materials and methodsAn observational, cross-sectional, comparative study was conducted. It included individuals of both sexes and of any age that presented with celiac disease, lived in Paraguay from January to April 2021, and agreed to participate in the survey. Incomplete questionnaires were excluded. Non-probabilistic convenience sampling was utilized. Adherence was measured using the Leffler questionnaire. The study was approved by the Ethics Committee of the Universidad Privada del Este.
ResultsThe sample consisted of 371 respondents, 322 (87%) of whom were adults, with a mean age of 38 ± 12 years, and 49 (13%) of whom were children and adolescents, with a mean age of 10 ± 5 years. Female sex was predominant (85%). Adherence to the gluten-free diet was detected in 59% of the adults and 73% of the children and adolescents. The factors significantly associated with adherence included belonging to the child and adolescent age group and having had the diagnosis for a longer time: 9 ± 8 years for the adherence group and 7 ± 8 years for the non-adherence group.
ConclusionsThe present study demonstrated the frequency of adherence to the gluten-free diet in celiac patients in Paraguay. Psychologic and nutritional support is recommended for individuals with celiac disease that do not adhere to their treatment.
El tratamiento de la enfermedad celiaca es la dieta sin gluten que debe realizarse en forma estricta y permanente. Los objetivos fueron determinar la adherencia a la dieta sin gluten y los factores de riesgo de no adherencia.
Material y métodosEstudio observacional, transversal, comparativo. Se incluyó a varones y mujeres, de cualquier edad, portadores de enfermedad celiaca, que viven en el Paraguay en el periodo enero-abril 2021 y aceptaron completar una encuesta. Se excluyeron los cuestionarios incompletos. Se utilizó un muestreo no probabilístico, por conveniencia. Se midieron variables demográficas y clínicas. La adherencia se midió con el cuestionario de Leffler. El estudio fue aprobado por el Comité de Ética de la Universidad Privada del Este.
ResultadosLa muestra se constituyó con 371 encuestados, siendo 322 adultos (87%) con edad media 38 ± 12 años y 49 niños y adolescentes (13%) con edad media 10 ± 5 años. Hubo un predominio del sexo femenino (85%). La adherencia a la dieta sin gluten se detectó en 59% de los adultos y en 73% de los niños y adolescentes. Los factores asociados significativamente a la adherencia fueron pertenecer al grupo etario de los niños y adolescentes, además de llevar más tiempo de diagnóstico: 9 ± 8 años para los adherentes y 7 ± 8 años para los no adherentes.
ConclusionesEste estudio permite conocer la frecuencia de la adherencia a la dieta sin gluten en celíacos del Paraguay. Se recomienda el apoyo psicológico y nutricional a los celíacos sin adherencia a su tratamiento.
Celiac disease (CD) is an autoimmune, chronic, multiorgan condition that affects genetically predisposed individuals and is precipitated by gluten ingestion1. Its treatment is based mainly on the strict and continuous following of a gluten-free diet (GDF), which requires education, motivation, and follow-up, on the part of the patient2. The continued ingestion of gluten causes chronic complications and the probability of developing digestive tract tumors3.
GFD adherence can be evaluated by quantifying levels of autoantibodies in blood, by duodenal biopsy findings, or in interviews with nutritionists and through self-reporting questionnaires4,5.
The celiac dietary adherence test developed by Leffler has shown elevated sensitivity and specificity for measuring compliance with the GFD5–7. It consists of few questions, is rapid and easy to apply, and has ideal psychometric characteristics because it also enables individuals with celiac disease that do not present with digestive manifestations to be evaluated. It measures symptomatology in celiac patients, their expectations of self-efficacy, their reasons for following a GFD, and their perceived dietary adherence. The questionnaire has already shown its effectiveness in different countries. It has also been translated into Spanish and can be applied through telematics8.
There are no current data on the prevalence of CD in Paraguay, nor on celiac dietary adherence in Paraguay or Latin America. The day-to-day problems related to a GFD and lifestyle experienced by Paraguayan individuals with celiac disease cannot be extrapolated from other studies, and so national data are required. A questionnaire that can be applied online is a useful tool for obtaining such information9.
The aims of the present study were to describe the demographic characteristics (age, sex, city of residence, economic independence) and clinical features (weight, height, age at CD diagnosis, initial clinical symptoms, diagnostic confirmation method, symptoms due to dietary gluten transgressions, comorbidities) in a group of individuals with celiac disease, as well as to determine dietary adherence to a GFD, utilizing the Leffler test for individuals with the condition.
Materials and methodsDesignAn observational, cross-sectional, comparative study was conducted.
Study populationThe population wasmade up of individuals of both sexes and of any age that presented with celiac disease, lived in Paraguay from January to April 2021, and agreed to participate in the survey. Incomplete questionnaires were excluded. Non-probabilistic convenience sampling was utilized.
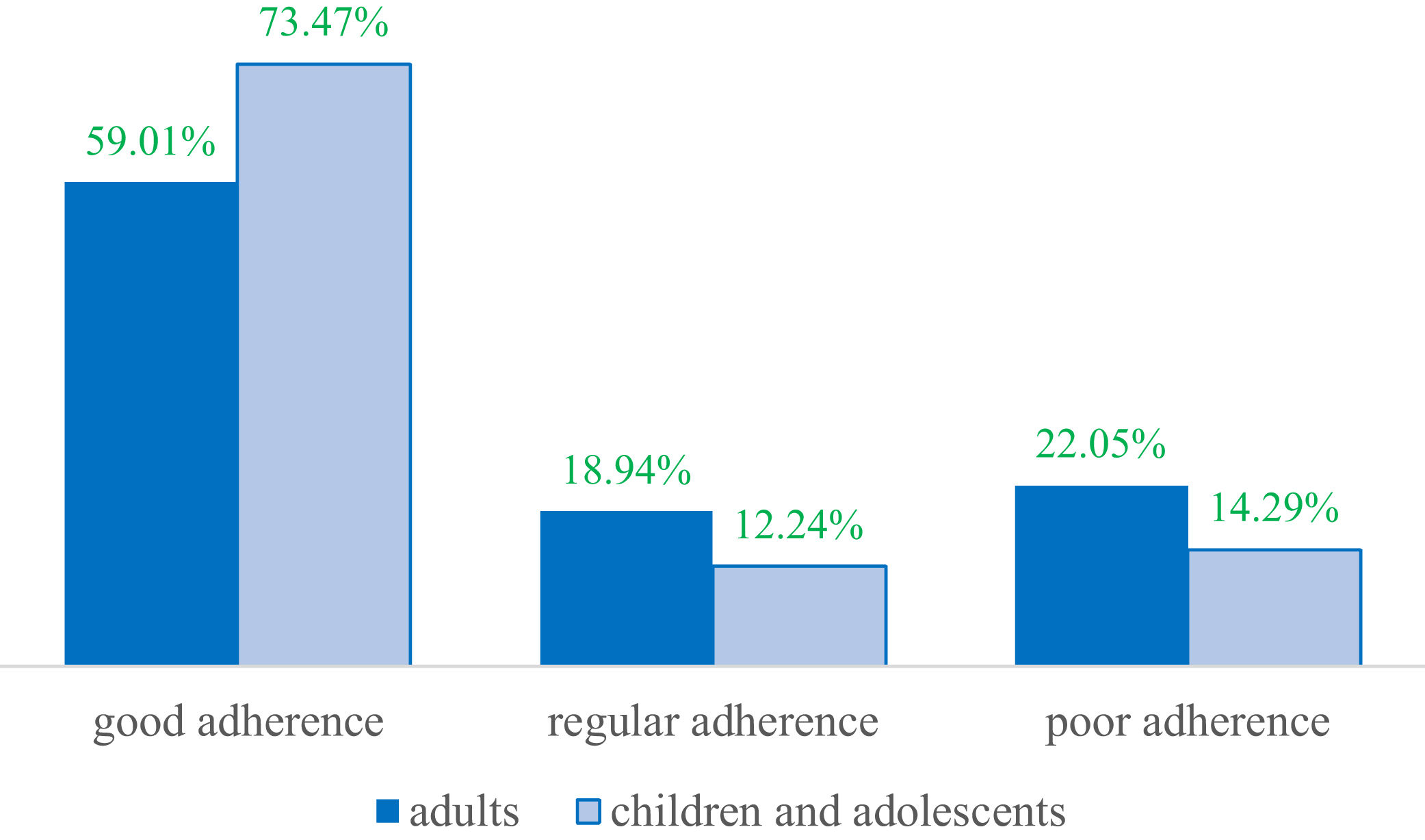
VariablesThe demographic (age, sex, city of residence, economic independence, educational level) and clinical (weight, height, age at CD diagnosis, diagnostic confirmation method, symptoms due to dietary gluten transgression, comorbidities, a family history of celiac disease) variables were evaluated, along with the results of the Leffler celiac dietary adherence test6. Each of the 7 questions in the Leffler instrument were measured as an ordinal variable, with a value of one point for the lowest option and 5 points for the highest. The questions were written, utilizing colloquial expressions, including one with a synonym in the Guarani language (Appendix A). The total number of test points ranged from 7 to 35 points. Good adherence to a GFD was considered for all scores ≤ 13 points, moderate adherence was a score of 14-16 points, and poor adherence was a score ≥ 17 points10. For statistical purposes, cases were considered those with poor adherence to a GFD and controls were those with good and moderate adherence.
Data managementThe questionnaire was applied online, utilizing the Google Meet™ Internet platform. The authors promoted it through social media and the affiliates of the Fundación Paraguaya de Celiacos. If the individuals with celiac disease were minors, their parents or guardians were asked to complete the questionnaire. The answers were registered on an electronic spreadsheet and underwent a descriptive statistical analysis, using the Epi Info 7™ program. The qualitative variables were expressed as frequencies and percentages, and the quantitative variables as measures of central tendency and dispersion. The chi-square test and Student’s t test were employed to evaluate the association between variables. Statistical significance was set at a p < 0.05.
Sample sizeSample size was calculated using the Epi Dat 3.1™ program. According to previous studies, the expected GFD adherence was 33%11. Utilizing a 95% confidence level and 5% accuracy, at least 340 subjects were calculated to be included in the analysis.
Ethical considerationsBioethics principles were respected, as was data confidentiality, given that the questionnaire was anonymous. Study motives and the person responsible for data management were explained, before the questionnaire was answered. The study protocol was approved by the Ethics Committee of the School of Medicine of the Universidad Privada del Este (Paraguay). There were no commercial conflicts of interest.
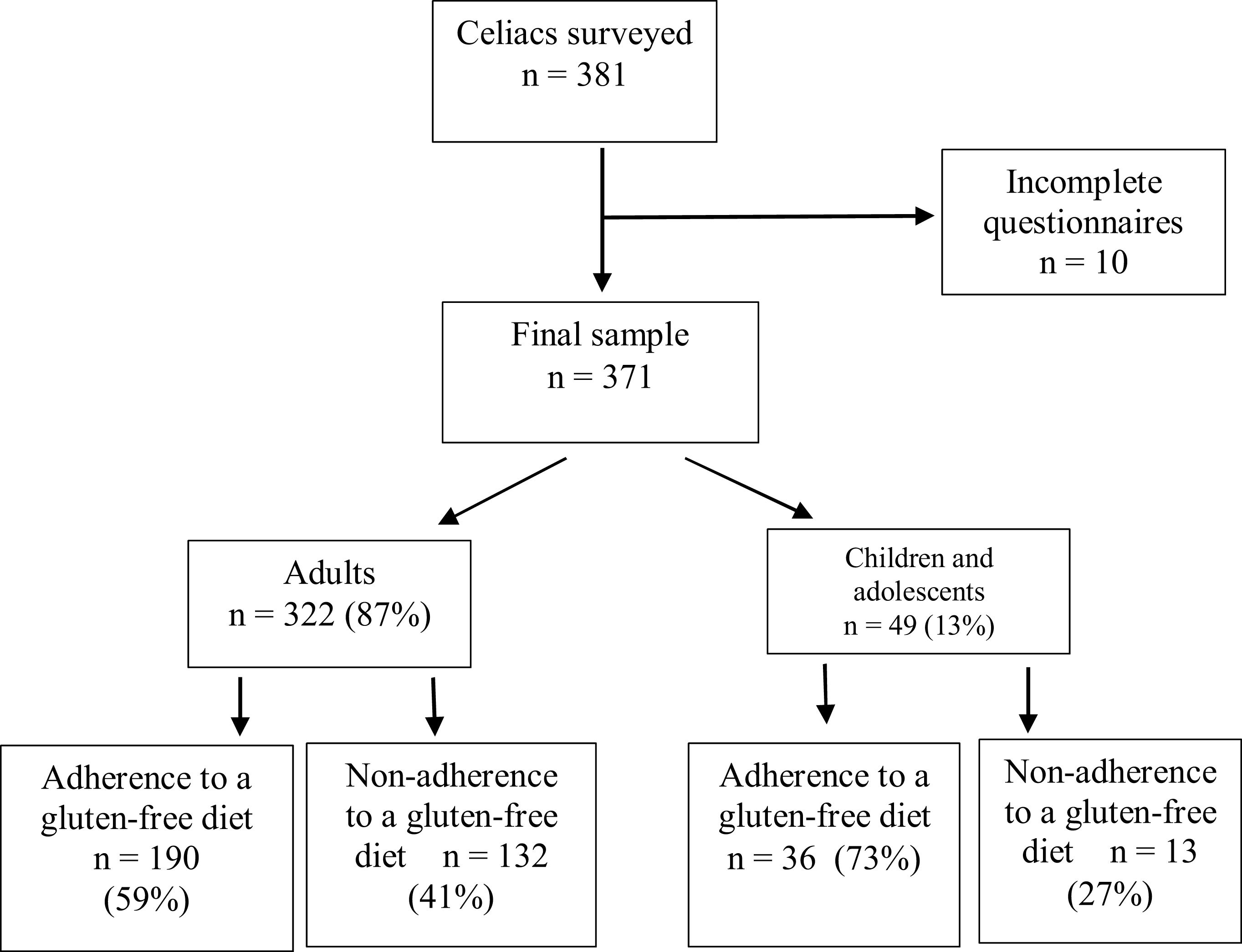
ResultsThe sample was made up of 371 surveyed individuals (Fig. 1).
Female sex was predominant (85%). Table 1 describes the rest of the demographic characteristics.
Demographic characteristics of the celiac patients surveyed (n = 371).
| Demographic characteristics | Frequency (%) | |
|---|---|---|
| Sex | Female | 316 (85%) |
| Male | 55 (15%) | |
| Mean age ± SD | Adults (n = 322) | 38 ± 12 years |
| Children and adolescents (n = 49) | 10 ± 5 years | |
| Place of residence | Asunción | 109 (29%) |
| Central department | 176 (47%) | |
| Other departments | 86 (24%) | |
| Educational level | Primary | 32 (9%) |
| Secondary | 71 (19%) | |
| University | 268 (72%) | |
| Economic independence | With own income | 241 (65%) |
| Without own income | 130 (35%) | |
SD: standard deviation.
The clinical characteristics are detailed in Table 2.
Clinical characteristics of the celiac patients surveyed (n = 371).
| Clinical characteristics | Children and adolescents (n = 49) | Adults (n = 322) |
|---|---|---|
| Nutritional status | ||
| Malnutrition | 4 (8%) | 12 (4%) |
| Normal BMI | 40 (82%) | 153 (48%) |
| Overweight | 2 (4%) | 127 (39%) |
| Obesity | 3 (6%) | 30 (9%) |
| Progression time | ||
| Age at diagnosisa | 4 (2–9) years | 29 (21–38) years |
| Gluten-free diet durationa | 3 (2–7) years | 8 (3–50) years |
| Symptom onset | ||
| Chronic diarrhea, dyspepsia | 37 (75%) | 263 (82%) |
| Anemia | 9 (18%) | 132 (41%) |
| Herpetiform dermatitis | 7 (14%) | 86 (27%) |
| Casual finding | 7 (14%) | 34 (10%) |
| Diagnostic confirmation method | ||
| Upper gastrointestinal endoscopy | 30 (61%) | 265 (82%) |
| Autoantibodies, HLA gene | 18 (37%) | 45 (14%) |
| Never confirmed | 1 (2%) | 12 (4%) |
| Blood relatives with celiac disease | ||
| With celiac relatives | 25 (49%) | 155 (48%) |
| With no celiac relatives | 25 (51%) | 167 (52%) |
| Comorbidities | ||
| Primary hypothyroidism | 2 (4%) | 49 (15%) |
| High blood pressure | 0 | 34 (10%) |
| Diabetes mellitus | 2 (4%) | 11 (3%) |
BMI: body mass index.
Upon evaluating the answers to the Leffler questionnaire, 145 (39%) of the subjects were found to not adhere to a GFD, with a predominance of adults (Fig. 1). When discerning the level of adherence by age group, children and adolescents had the best adherence, whereas adults had the worst (p 0.1) (Fig. 2).
When analyzing the risk factors for poor GFD adherence, adult age was a significant factor (p 0.05) (Table 3). The mean number of years on a GFD was 9 ± 8 years for dietary adherence and 7 ± 8 years for dietary non-adherence (p 0.02).
Risk factors for non-adherence to the gluten-free diet in celiacs (n = 322).
| Risk factors | Adherence (n = 226) | Non-adherence (n = 145) | (95% CI) |
|---|---|---|---|
| Male sex | 37 (67%) | 18 (33%) | 1.1 (0.9-1.3) |
| Female sex | 189 (60%) | 127 (40%) | |
| Children and adolescents | 36 (73%) | 13 (27%) | 0.8 (0.6-0.9)* |
| Adults | 190 (59%) | 132 (41%) | |
| Primary and secondary school education | 67 (65%) | 36 (35%) | 0.9 (0.7-1.0) |
| University education | 159 (59%) | 109 (41%) | |
| Own income | 148 (61%) | 93 (39%) | 0.9 (0.8-1.1) |
| Dependent on another’s income | 78 (60%) | 52 (40%) | |
| Initial symptom presentation | 212 (60%) | 139 (40%) | 1.1 (0.8-1.5) |
| Casual finding | 14 (70%) | 6 (30%) | |
| Gluten intake discomfort | 180 (64%) | 102 (36%) | 0.8 (0.6-1.0) |
| No gluten intake discomfort | 46 (52%) | 43 (48%) |
In the present study, the frequency of GFD adherence in Paraguayan individuals with celiac disease, was 59% in adults and 73% in children and adolescents. A 2017 study conducted in Paraguay found that 33% of the celiac individuals maintained a strict GFD, 58% had occasional dietary transgressions, and 9% frequently consumed gluten11. In a similar study conducted in 2020, 15% of the general population followed a GFD, but the analysis included celiac and non-celiac individuals12.
In other countries, GFD adherence frequency, also determined through surveys, varied widely: 7% in El Salvador13, 7.48% in Brazil14, 6.37% in Argentina15, 5.9% in Colombia16, 47% in Australia17, 47% in Poland18, 53% in India19. 57% in Mexico20, 70% in Chile21, 61% in Australia22, 62% in Canada23, 65% in Italy24, 75% in the United States17, 80% in Brazil25, 83% in Norway26, and 90% in Spain9. The broad difference between countries can be explained by their demographic, sociocultural, and economic diversity, emphasizing the importance of having national data, as in our sample, to enable specific action to be taken to improve the frequency of GFD adherence19.
Interestingly, 13 of the individuals surveyed in our study had no histologic confirmation of CD. They were not excluded from the analysis because they had positive serology, herpetiform dermatitis, or blood relatives with celiac disease, and presented with digestive symptoms upon gluten ingestion. The confirmatory diagnosis of CD in adults continues to be duodenal biopsy and treatment response, but many patients are known to reject the endoscopic study, preferring to directly undertake a GFD, especially older adults1,27. Nevertheless, the need for diagnostic confirmation should be underlined, given that a GFD must be strict and life-long7,28.
Malnutrition was detected in 4% of the adults and 8% of the children and adolescents and was associated with GFD non-adherence in 50% of the cases. The persistence of alterations in the intestinal mucosa and poor food absorption are the likely explanation29. However, that phenomenon requires more detailed study with a nutritional approach30.
GFD adherence depends on numerous factors that involve the individual, as well as relatives and the community. Those factors can either promote the effect or act as a barrier31. We initially sought an age cutoff point for GFD adherence and non-adherence but decided to present the results based on demographically known age groups: children, adolescents, and adults. Because the first two groups are socially dependent on adults, we separated them from the adults to perform the analyses. Belonging to the children and adolescent age group was the only significant factor in the present study. Hypervigilance of the dietary restriction has been shown to be easier in children but decreases in adolescence and adulthood32,33. Strict parental control is easier at home than outside of it, but GFD adherence tends to decrease when adolescents feel the social pressure of their classmates and friends34. GFD adherence results in nutritional status improvement and symptom disappearance, but quality of life can deteriorate due to the social demands the diet imposes35,36. One study detected that quality of life in Paraguayan celiac individuals was good in 25%, regular in 49%, and poor in 26%, and that poor quality of life was not significantly associated with GFD adherence11.
Another significant factor was the mean number of years on a GFD: 9 ± 8 years for the individuals that adhered to a GFD and 7 ± 8 years for those that did not. That could be due to the fact that the more recently diagnosed individuals could make more mistakes and have more disinformation and inexperience, in relation to the complexity of strictly following a GFD, especially outside of the home37. Nevertheless, that hypothesis requires confirmation through another, possibly qualitative, study focused on said aspect.
Individuals with celiac disease that had a higher educational level and their own income had better GFD adherence. That could be explained by the fact that higher education improves the level of knowledge about the risks of voluntary gluten ingestion and enables the individuals to identify and interpret the nutritional information labels on food products38. In addition, the costs of processed foods for celiac patients are much higher and can be inaccessible to individuals economically dependent on a third party39. However, those factors need to be extensively evaluated in further studies.
Many of the individuals surveyed stated they had been casually diagnosed because they had blood relatives with CD. The families of new celiac patients are advised to undergo serologic testing for CD screening, even if they are asymptomatic, given that they are a risk group1,28. In our sample, the celiac individuals that had relatives with the disease had better GFD adherence, possibly because there was family support for carrying out the treatment. The containment of anxiety suffered by the recently diagnosed celiac patient that comes from staying at home, even if he/she is asymptomatic, is a recognized adherence facilitator31,40.
Another GFD adherence factor was the appearance of symptoms after voluntary or accidental gluten ingestion. Celiac patients that present with digestive symptoms recognize that any ingestion of gluten has a negative effect on their health, often explosively, leading them to restrain from voluntary gluten ingestion, thus contributing to GFD adherence31. Nevertheless, many celiac individuals tolerate small quantities of gluten, which can be harmful, because the intestinal mucosa remains inflamed and is associated with chronic complications: anemia, osteoporosis, and neoplasia1,3.
The limitations of the present study were its cross-sectional design and non-randomized sampling, as well as a lack of autoantibody level measurement or duodenal biopsy for confirming GFD adherence5. There could have been response bias, given that many celiac individuals do not have access to social media or the internet. Others may have had age or socioeconomic-related difficulties, such as the availability of electronic communication devices, for answering the questionnaire. Another limitation was the fact that many gluten-intolerant individuals could have participated in the survey, knowing that such individuals cannot be classified as having CD12. In contrast, our study’s strengths were its multicenter character and adequate sample size. Ongoing education of celiac patients, psychologic and nutritional support, and attending self-help groups, such as the Fundación Paraguaya de Celiacos, are recommended12.
In conclusion, GFD adherence was detected in 59% of the adults and 73% of the children and adolescents. The factors significantly associated with adherence were belonging to the age group of children and adolescents and having been diagnosed for a longer period of time: 9 ± 8 years for the individuals with dietary adherence and 7 ± 8 years for those with non-adherence.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were conducted on humans or animals for the present study.
Confidentiality of data. The authors declare that no patient data or images appear in this article that could identify patients. The study protocol was approved by the Bioethics Committee of the School of Medicine of the Universidad Privada del Este, Paraguay.
Right to privacy and informed consent. The authors declare that informed consent was requested, even though no patient data were published.
Author contributionsR. E. R-D and M. E. C-A contributed equally with respect to the study concept, data collection and analysis, discussion, and final approval of the manuscript.
Financial disclosureThe study was carried out with the participating institutions’ resources.
Conflict of interestThe authors declare that there is no conflict of interest.
| Gluten-free diet adherence questionnaire | |
|---|---|
| Has your energy level been low (caigüe) during the past four weeks? | None of the time |
| A little of the time | |
| Some of the time | |
| Most of the time | |
| All of the time | |
| Have you had headaches during the past 4 weeks? | None of the time |
| A little of the time | |
| Some of the time | |
| Most of the time | |
| All of the time | |
| Are you able to follow a gluten-free diet outside of your home? | Always |
| Almost always | |
| Many times | |
| Rarely | |
| Never | |
| Do you carefully consider the consequences before eating something? | Always |
| Almost always | |
| Many times | |
| Rarely | |
| Never | |
| Do you consider yourself a failure with respect to the gluten-free diet? | Never |
| Few times | |
| Sometimes | |
| Many times | |
| Always | |
| Is the accidental ingestion of a gluten-containing food consequential for your health? | Very important |
| Quite important | |
| I’m not sure | |
| Not very important | |
| Not at all important | |
| In the past 4 weeks, how often have you eaten gluten-containing food? | Never |
| 1 to 2 times | |
| 3 to 5 times | |
| 6 to 10 times | |
| More than 10 times | |
See related content in DOI:1016/j.rgmxen.2023.04.003, Uscanga Dominguez L.F. Editorial: Adherence to a gluten-free diet: how much is a little? Rev Gastroenterol Méx. 2023;88: 305–306.

