











The incidence of esophageal cancer is steadily increasing worldwide. Outcome is poor, given that the majority of cases are diagnosed at advanced disease stages. However, when detected at early stages, esophageal tumors can be curatively treated through less invasive methods, resulting in a 5-year survival rate above 90%. Therefore, it is essential to identify the high-risk population and recommend those patients undergo screening using high-resolution endoscopy, adding the resources of chromoendoscopy with Lugol solution (or digital chromoendoscopy) and magnification. Such systematized examination makes it possible to recognize early-stage esophageal neoplasia and propose endoscopic submucosal dissection as treatment. In that procedure, the tumor is resected en bloc, resulting in lower morbidity and mortality, compared with previous standard treatment, including early-stage esophagectomy. The present article is a review of the latest advances in the management of superficial esophageal tumors through endoscopic submucosal dissection.
La incidencia del cáncer de esófago viene aumentando progresivamente a nivel mundial. Su pronóstico es pobre ya que en su mayoría el diagnóstico se realiza en estadios avanzados. Sin embargo, cuando es detectado en estadio precoz, las neoplasias esofágicas pueden ser tratadas de forma curativa y por métodos menos invasivos, resultando en una sobrevida de más del 90% en 5 años. Por lo tanto, es clave identificar la población de alto riesgo del cáncer esofágico y recomendarles endoscopia de alta resolución de cribado, agregando recursos de cromoendoscopia con lugol (o digital) y magnificación. Este examen sistematizado permite reconocer la neoplasia esofágica en estadio temprano, donde se puede proponer tratamiento endoscópico mediante la disección endoscópica submucosa (DES) realizándose la resección en bloque de la lesión tumoral con disminución de la morbimortalidad en comparación con el tratamiento estándar previo, incluso en estadios tempranos como lo era la esofagectomía. El objetivo de este artículo es revisar los últimos avances en el manejo de las neoplasias esofágicas superficiales a través de la DES.
Malignant tumor of the esophagus is the eighth most frequent cancer and the sixth cause of death worldwide. An estimated 450,000 new cases were diagnosed in 2012, along with close to 400,000 deaths attributed to that condition. Those figures are related to the presentation of symptoms at advanced stages of the disease and the consequent poor prognosis. Definitive cure is no longer an option at the advanced disease stage, underlining the necessity of early stage diagnosis.1–4 The incidence of esophageal cancer has increased worldwide. In the United States, there has been a 7-fold increase in incidence over the last 30 years, especially in white males. Mean 5-year survival for esophageal cancer has not improved and remains below 15%.1,3
There are 2 primary neoplasias in the esophagus: squamous cell carcinoma (SCC) and adenocarcinoma. SCC is the most frequent type in Asia and the rest of the world and is associated with tobacco, alcohol abuse, nitrosamine use, caustic agent ingestion, achalasia, thermal injury due to hot drinks, tylosis, micronutrient deficiency (riboflavin, retinol, ascorbic acid, alpha-tocopherol, selenium, magnesium, and zinc). In turn, adenocarcinoma is frequent in Europe and North America and its risk factors are gastroesophageal reflux (Barrett's esophagus) and elevated body mass index.1,2,5–7 SCC of the esophagus is more frequent in men (3.6:1) between the fifth and seventh decades of life. In Brazil, the mortality rate is 14.3 men and 4.2 women for every 100,000 persons.8 Those two types of cancer differ in the metastatic lymphadenopathy rate, with a greater risk in patients with SCC, compared with patients with adenocarcinoma.7
The development of new endoscopic techniques that include chromoendoscopy with Lugol's solution, narrow-band imaging (NBI), flexible spectral imaging color enhancement (FICE), magnification endoscopy, confocal microscopy, high-resolution endoscopy, and spectroscopy have augmented sensitivity and specificity in the early-stage detection of those types of neoplasias. That is important, because early diagnosis of SCC improves its outcome, with 5-year survival rates of up to 95%.3,4,8–11
The treatment of choice for esophageal cancer has traditionally been surgical, even in early-stage disease. However, esophagectomy is associated with high morbidity and mortality rates.6 In the last two decades, endoscopic treatment that includes endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) has advanced, becoming a viable curative alternative to surgery in selected cases of early esophageal cancer. The advantages of endoscopic treatment are organ preservation, a practically null mortality rate, and low complication rates between 1-8% that include bleeding, perforation, and stricture. 2,6,9,11
EMR was the first endoscopic therapy to be developed and has been used as treatment for superficial SCC. It is an effective therapy and less invasive than esophagectomy. However, that technique only removes small lesions en bloc (<10mm). Larger lesions require piecemeal resection, which predisposes to imprecise histopathologic evaluation and is associated with increased rates of local recurrence.2,4,10 The ESD technique was developed in Japan and proposes en bloc resection of lesions larger than 20mm, reducing the need for piecemeal resection and enabling a precise evaluation of the resection margins (vertical and lateral), resulting in much lower local recurrence rates than with EMR and an excellent long-term cancer-free survival rate.4,6,12–14
The aim of the present article was to contribute to the understanding of recent advances in esophageal cancer management with a detailed review of the ESD technique in patients with SCC, diffusing information of that procedure so it can be incorporated into Western endoscopy centers, especially in Latin America. Because there are certain differences in the management of endoscopic treatment of SCC of the esophagus from that of adenocarcinoma and high-grade Barrett's esophagus, our review focused on the technical aspects related to the diagnosis and treatment of SCC of the esophagus.
DiagnosisEsophageal neoplasia classically presents with progressive dysphagia and weight loss. When there is chest pain, invasion into the mediastinum should be suspected, and if there is associated ulceration or proximal esophagitis, the patient can manifest odynophagia.1 Tumors tend to be advanced in those cases, with no possibility of endoscopic curative treatment. Therefore, the first challenge is to establish diagnosis of esophageal cancer in its early stage, in other words, when the patient is asymptomatic and has subtle endoscopic changes that are difficult to recognize. Among such changes are a mucosa with pale or red epithelium and altered microvascular pattern with slight elevation or depression of its surface (fig. 1).1,8

The best diagnostic method is endoscopy, and even better, when it is combined with chromoendoscopy. That technique improves detection, given that squamous dysplasia can be difficult to recognize through standard endoscopy.2,8 Nevertheless, performing endoscopy on the general population as screening for SCC is not justifiable, due to the cost of the procedure, but it is cost-effective in the high-risk population, such as patients with squamous cell cancer of the head and neck.8
Chromoendoscopy utilizing Lugol's solution is considered the method of choice for the diagnosis of SCC and has 96% sensitivity and 63% specificity, compared with conventional white light endoscopy, which has 62% sensitivity and 79% specificity (fig. 2)2,8 Lugol's solution is a dye that reacts with squamous cells of the esophagus that have a high glycogen content. Thus, neoplastic or dysplastic cells do not have that reaction because of their poor glycogen storage. However, the “pink sign” should be evaluated. It consists of a change in the color of the neoplastic lesion from yellow to pink, 2 to 5min after Lugol's solution application (fig. 3). The pink sign is highly specific for dysplasia or SCC.4,8


Nevertheless, Lugol's solution application involves greater time and costs and also has the adverse effects and complications of allergic reaction, chest pain, or solution aspiration. Currently, the new digital chromoendoscopy methods of FICE and NBI can reduce those adverse situations15,16 (fig. 4). Arantes et al.15 conducted a study that utilized transnasal endoscopy as the esophageal SCC detection method in patients with squamous cell cancer of the head and neck, applying the diagnostic techniques of white light endoscopy and FICE and comparing them with the gold standard of Lugol's solution. They found that the first two methods were similar in SCC detection and had high sensitivity and specificity values. A systematic review and meta-analysis by Morita et al.16 was recently published on the diagnosis of high-grade dysplasia and SCC in the esophagus, comparing NBI and Lugol's solution. They found that both methods had the same detection rate. Thus, the new digital methods of chromoendoscopy are useful for adequate screening.
Endoscopic staging of early esophageal cancer
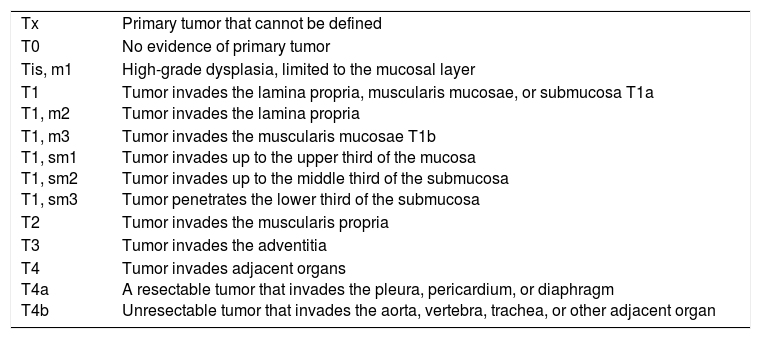
Outcome and adequate selection of treatment for esophageal cancer is closely related to disease staging.7 Early esophageal cancer is defined as lesions whose morphologic aspect compromise the mucosal and submucosal layers, without infiltrating the muscularis propria.7,9,17 Flat superficial neoplasias predominate in the esophagus and are subdivided in relation to the adjacent mucosa as superficially raised (IIA), flat (IIB), and depressed (IIC). Protruded and excavated forms, based on the Paris classification, are rare.17 Superficial neoplasias are subdivided according to the degree of transmural penetration as follows: m1: corresponds to the epithelium and basal layer; m2: lamina propria; and m3: muscularis mucosae. If there is invasion into the submucosa, it is classified as sm1: upper third; sm2: middle third; and sm3: lower third. In the absence of invasion into the lamina propria, the lesion is denominated intraepithelial neoplasia with high-grade dysplasia and the term carcinoma in situ can be used, as described in Table 1. 2,7,17
Definitions of category T for esophageal cancer.
| Tx | Primary tumor that cannot be defined |
| T0 | No evidence of primary tumor |
| Tis, m1 | High-grade dysplasia, limited to the mucosal layer |
| T1 T1, m2 | Tumor invades the lamina propria, muscularis mucosae, or submucosa T1a Tumor invades the lamina propria |
| T1, m3 T1, sm1 T1, sm2 T1, sm3 | Tumor invades the muscularis mucosae T1b Tumor invades up to the upper third of the mucosa Tumor invades up to the middle third of the submucosa Tumor penetrates the lower third of the submucosa |
| T2 | Tumor invades the muscularis propria |
| T3 | Tumor invades the adventitia |
| T4 T4a T4b | Tumor invades adjacent organs A resectable tumor that invades the pleura, pericardium, or diaphragm Unresectable tumor that invades the aorta, vertebra, trachea, or other adjacent organ |
Tis: Carcinoma in situ.
The classification described above aids in defining the risk for presenting with metastatic lymphadenopathy, given that they are closely related to the vertical depth or level of the lesion in the wall of the affected organ, which is a key factor in the selection of patients for successful curative endoscopic treatment. Thus, when tumor involvement is limited to the superficial epithelium (m1 and m2), the risk for metastatic lymphatic involvement is almost null and endoscopic treatment is sufficient for cure. But if the tumor invades the muscularis mucosae (m3) and the proximal portion of the submucosa at a depth less than 200μm under the muscularis mucosae (sm1), the risk can reach 9 and 19%, respectively, especially if there is lymphatic or vascular invasion. Those cases are on the borderline of curative endoscopic treatment and therefore an integrated evaluation is essential for defining the following parameters: tumor size, lymphovascular invasion, and horizontal extension of the invasion into the muscularis mucosae, given that there is a high risk for metastatic lymphadenopathies in tumors that deeply invade the submucosa.4,6,9,12,17,18
Staging of esophageal cancer should begin with a thoracoabdominal computed tomography scan to evaluate distant metastasis. However, tomography has poor sensitivity for detecting celiac lymphadenopathies and small metastases (particularly peritoneal ones) and lesion depth cannot be defined. Endoscopic ultrasound enables a more accurate definition of the depth of invasion of the lesion and the presence of metastatic lymphadenopathies in the mediastinum or the celiac trunk, thus determining stages T1a and T1b with a sensitivity and specificity above 80%.7,9,19 Patients with complete invasion of the submucosa or with regional or distant metastases determined through tomography or endoscopic ultrasound, should not undergo ESD.19
Endoscopic treatment indications for early esophageal cancerThe following are the criteria for curative endoscopic resection of early esophageal cancer:17
- 1.
Lesion depth restricted to stages m1 and m2 (basal layer and lamina propria).
- 2.
Maximum length of 3cm and lateral extension less than 3/4 of the circumference.
- 3.
Maximum of 4 lesions.
With the incorporation of ESD, lesions can be larger than 3cm, even if they occupy the totality of the circumference, in addition to there being no limit as to the number lesions, as long as they are early neoplasias.17 The Japan Esophageal Society defines the absolute indications for ESD in early SCC of the esophagus as: esophageal lesion limited to the epithelium (m1) or lamina propria (m2), but involving less than 2/3 of the circumference. Among the relative indications that should be considered for adding chemotherapy and radiotherapy are: lesion that invades the muscularis mucosae (m3) or submucosa (sm1), but with no lymphadenopathies or metastases prior to the ESD, and lesion limited to the epithelium (m1) or lamina propria (m2), involving more than 2/3 of the circumference of the esophagus.4,6,17
Endoscopic submucosal dissection of early esophageal cancerEndoscopic resection of the mucosa was developed at the end of the 1980s and was rapidly accepted as an alternative to surgery in the treatment of superficial esophageal neoplasia.20,21 However, complete extraction was not possible in larger lesions (15mm), and so piecemeal resection was developed for those types of tumor. There was a high rate of local recurrence with that technique, which was resolved with the development of the new endoscopic therapy of ESD.2,6,19,20
ESD is an advanced endoscopic technique whose aim is to allow en bloc resection in lesions larger than 2cm. It also covers the detection, diagnosis, treatment, and prevention and management of complications (bleeding, perforation, stricture) with long-term follow-up, and therefore requires adequate training. Despite the fact that the minimum number of cases needed to perform ESD of the esophagus is not defined, Japanese experts recommend carrying out at least 50 ESD procedures in the distal stomach or rectum, before performing it in the esophagus.4,17,22,23
ESD was originally designed for application in the stomach, but was later applied in the esophagus, colon, and rectum. The wall of the esophagus measures 3.5-4mm, increasing its technical difficulty, due to the reduced luminal space, compared with the stomach. However, despite that greater technical difficulty, ESD has been shown to be an effective and safe treatment for SCC of the esophagus, increasing patient survival rates.7,17,19,22,24
The wall of the digestive tract is made up of two main components: the mucosa and the muscularis mucosae. They both are separated by the submucosa (connective tissue), signifying that en bloc resection involves a risk for involuntary injury of the muscular layer, resulting in perforation of the viscera. To reduce that risk, the injection of a viscous solution of sodium hyaluronate, hydroxypropyl methylcellulose, sodium carboxymethylcellulose, hypertonic dextrose, hypertonic saline, fibrinogen, or glycerol is required to separate the early neoplasia from the muscularis propria.7,12,17
Esophageal endoscopic submucosal dissection techniqueThe procedure is performed with the patient under deep sedation, generally with endotracheal intubation that facilitates better sedation and prevents the risk for aspiration. Prophylactic antibiotic use is controversial and not well-defined, even though different endoscopy centers in Japan use second-generation cephalosporins IV for 3 days.4,17,20
After complete lesion evaluation utilizing magnification endoscopy and digital chromoendoscopy, chromoendoscopy with Lugol's solution at 0.8% should be carried out to adequately define the limits of the lesion (fig. 2).4,17,19,24,25 The most widely recommended electrosurgical equipment is VIO 200D or 300D (Erbe Elektromedizin GmbH, Tu¿bingen, Germany). ESD can be performed using different types of endoknives: the Hook Knife (KD- 620LR, Olympus, Tokyo, Japan); the Dual Knife (KD- 650, Olympus, Tokyo, Japan); and the IT Knife (KD-612, Olympus, Tokyo, Japan), which is the most widely used in gastric ESD. However, it has a high perforation rate in ESD of the esophagus, leading to the recent development of the IT Knife nano (KD- 612, Olympus) for ESD of the colon and esophagus.20 There is also the 1.5 mm-long short stylet needle: the Flush Knife (FK) (Fujifilm, Tokyo, Japan), which not only enables marking, incision, submucosal dissection, and hemostasis, but also makes the simultaneous injection of saline solution possible.9,12,17,20,23 CO2 insufflation is indicated because it is absorbed more quickly than air and excreted during respiration, which is useful for preventing severe mediastinal emphysema, and in the case of perforation, it provides enough time for endoscopic closure with endoclip.4,12,20 In the present review, we describe esophageal ESD utilizing the FK.
After the chromoendoscopy, the limits of the lesion are marked with the FK with ERBE parameters: soft coagulation, effect 5, 100W, with a minimum distance from the lesion of 2mm from the lateral margins and 5mm from the proximal margins to reduce the risk of stricture caused by ESD (fig. 5).4,17,20 Injection of the submucosa with saline solution is then carried out, which should be done at the oral margin of the lesion from one end to the other. First saline solution is injected, followed by an injection of 0.4% sodium hyaluronate solution (Muco-Up®, Seikagaku, Japan), which keeps the lesion raised for a longer period of time.4,12,17,26

A transverse and lateral incision with the FK is then made, deep enough to reach the submucosal plane (parameters: Endocut I, effect 4, cut duration: 2, cut interval: 3) (fig. 6). In addition, the cap is used for presenting the submucosal tissue and the endoscopic submucosal dissection is carried out in the oral-anal direction, always parallel to the axis of the esophageal wall to prevent perforation risk (submucosal layer dissection parameters: forced coagulation, effect 2, 40W) (fig. 7).4,17,20 Every time electric dissection is performed, injection of saline solution at the level of the submucosa can be added.17


An important part of making the procedure safer is preventing bleeding during ESD and adequate hemostasis is essential. If a submucosal vessel is identified, or unexpected bleeding presents, hemostasis must be performed with the FK (parameters: soft coagulation, effect 5, 100W) for 3 to 5 s on each side of the vessel, followed by forced coagulation.12,17,20 If hemostasis cannot be controlled in 3 attempts, the COAG grasper (Olympus, Tokyo, Japan) hemostasis forceps should be used.20,25
Finally, the samples must be removed with a foreign body tweezer, trapped on the submucosal side to not damage the mucosal side of the lesion. The dissection site should be re-evaluated (fig. 8) if prominent vessels are observed and they should receive hemostasis. If there are muscular layer lacerations, therapy should be performed with an endoscopic clip. The sample is fixed with pins over a plate of expanded polystyrene (tecnopor) and placed in formalin (fig. 9). The pathologist should cut the sample into 2-cm-wide fragments that are parallel and perpendicular to the lesion and evaluate them according to the Vienna Classification, identifying: the size of the lesion, its differentiation grade, and its depth, along with the proximal, distal, lateral, and vertical margins.8,17,25 The depth of the invasion is measured in micrometers (μm) from the last layer of the muscularis mucosae, with a cutoff point of 200μm for sm1.25
Post-esophageal endoscopic submucosal dissection

The patient usually remains in a fasting state the first 24h after ESD therapy, with oral sucralfate and 40mg of a proton pump inhibitor (PPI) every 12h. A progressive liquid diet can be initiated the next day.4,19 Patients with gastroesophageal reflux should receive PPI therapy for 2 months after the procedure. Endoscopic control should be carried out 3 months after ESD, after which annual endoscopy that includes chromoendoscopy, should be performed to evaluate recurrence or metachronous lesions (fig. 10).4
Esophageal endoscopic submucosal dissection complications. Patient received prophylactic oral corticoid therapy for stricture for 4 weeks.")
Complication rates are low, at 0 to 4% for significant bleeding, defined as that above 500ml or a fall in hemoglobin > 2g/dl, and at 2.6-6.9% for perforation. The latter can cause mediastinal emphysema, which has been described as a complication in different published case series. Emphysema increases the mediastinal pressure, reducing the esophageal lumen, resulting in inadequate visualization of its mucosa. But severe mediastinal emphysema can also present, with the complication of developing pneumothorax, which can end in shock. Therefore, the patient should be monitored during the procedure through an electrocardiogram, oxygen saturation, capnography, blood pressure, and periodic cervical palpation to evaluate the presence of subcutaneous emphysema.14,20,24,25 If there is perforation after ESD, it can be treated conservatively with endoclip placement, NPO, adequate hydration, and antibiotic therapy.4
Stricture is the complication of greatest incidence, from 3 to 18%, after ESD of the esophagus. The extension of the resection is the most important predictor. If it is above 75% of its circumference, there is a higher probability of presenting with that event. Esophageal stricture is a factor that reduces patient quality of life and can require numerous balloon dilation sessions.4,17,20,27 The efficacy of oral prednisone has been described for stricture prevention (fig. 11). In the Japanese study conducted by Kataoka et al.,28 they compared 2 groups: one that received treatment with oral systemic steroids with an initial dose of 30mg of prednisone that was gradually decreased each week, and the other that received no preventive treatment. The authors found that the stricture rate and the number of balloon dilation sessions were considerably lower in the group that received the corticoids, versus the group that did not, and the differences were statistically significant. Another option is the injection of 4ml of triamcinolone acetate, 10mg/ml through an injection catheter, carrying out 20 punctures of solution of 0.2ml each, at the edge and the center of the resection.4,17,20 Other options for the prevention of esophageal stricture after circumferential ESD include hydrostatic balloon dilation, the use of polyglycolic acid membranes, autotransplantation of gastroesophageal tissue, and the use of metal stents.29
Conclusions
ESD is the treatment of choice for early-stage SCC. It has a low recurrence rate and reduced morbidity and mortality. The greatest challenge is to have early diagnosis of esophageal cancer, and so screening and surveillance programs for high-risk patients are a priority. ESD is technically more difficult in the esophagus than in the stomach, due to its narrow lumen, and its safe and efficient performance requires adequately trained endoscopists. It is essential to develop training centers in Latin America for the professionals interested in learning ESD, a procedure that would offer great quality of life benefits to the patients in our communities that are candidates for its performance.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Arantes V, Espinoza-Ríos J. Manejo del carcinoma de células escamosas de esófago precoces a través de la disección endoscópica submucosa. Revista de Gastroenterología de México. 2018;83:259–267.

