





Gastroesophageal reflux disease (GERD) is highly prevalent in patients with idiopathic pulmonary fibrosis (IPF), even in the absence of symptoms. Information on this disease in Latin America is limited. The aim of our study was to determine the prevalence of dysmotility and GERD through high-resolution esophageal manometry (HREM) and 24 h multichannel intraluminal impedance-pH (MII-pH) monitoring in IPF patients, candidates for lung transplantation.
Material and methodsA retrospective, descriptive, observational study was conducted at a tertiary care hospital center. HREM and 24 h MII-pH studies were carried out as part of the protocol for lung transplantation candidates. The manometric and impedance data, including the thoracoabdominal pressure gradient (TAPG), were analyzed.
ResultsThe study included 37 patients. The mean distal contractile integral was 1530.47 mmHg-s-cm (SD ± 1210.03). Fourteen patients (37.8%) presented with ineffective esophageal motility (IEM). The median percentage of acid exposure time (AET) was 3.20% (range: 1.42-4.90) in the patients with IEM versus 0.50% (range: 0.2-2.90) in the patients with normal esophageal motility (p = 0.022). The mean AET percentage was 3.02% (SD ± 4.17) and the mean number of proximal reflux episodes was 25.88 (SD ± 19.37). Five patients (13.5%) had abnormal AET and a mean TAPG of 14.66 mmHg (SD ± 4.89) versus 17.09 mmHg (SD ± 6.92) in patients with AET < 6% (p = 0.457).
ConclusionsAlmost 40% of the patients with IPF, who were candidates for lung transplantation, had IEM. However, the prevalence of GERD was low and not associated with changes in the TAPG.
La enfermedad por reflujo gastroesofágico (ERGE) es altamente prevalente en pacientes con fibrosis pulmonar idiopática (FPI), incluso en ausencia de síntomas. La información al respecto en Latinoamérica es limitada. El objetivo de este trabajo fue determinar la prevalencia de dismotilidad y ERGE con manometría esofágica de alta resolución (HRM) e impedanciometría multicanal con phmetría (IMM-pH) de 24 horas en pacientes con FPI candidatos a trasplante pulmonar.
Material y métodosEstudio retrospectivo, descriptivo y observacional realizado en un centro de tercer nivel. Se realizaron estudios de HRM e MII-pH de 24 horas como parte del protocolo de candidatos a trasplante pulmonar. Se analizaron los datos manométricos y de impedanciometria incluyendo el gradiente de presión toracoabdominal (GPTA).
ResultadosSe incluyeron 37 pacientes. La media de DCI fue de 1530.47 mmHg.cm.s (DE ± 1210.03). Catorce (37.8%) presentaron motilidad esofágica ineficaz (MEI). Los pacientes con MEI tenían una mediana de porcentaje de tiempo de exposición al ácido (TEA) de 3.20% (rango: 1.42-4.90) vs. 0.50% (rango: 0.2-2.90) en pacientes con motilidad esofágica normal, (p = 0.022). La media del porcentaje de TEA fue 3.02% (DE ± 4.17). La media de episodios proximales de reflujo fue 25.88 (DE ± 19.37). Cinco (13.5 %) pacientes tuvieron un TEA anormal y éstos presentaron una media de GPTA de 14.66 mmHg (DE ± 4.89) vs. 17.09 mmHg (DE ± 6.92) en aquellos con un TEA < 6%, (p = 0.457).
ConclusionesCasi el 40% de los pacientes con FPI candidatos a trasplante tienen MEI. Sin embargo, la prevalencia de ERGE es baja y no se asocia a cambios en el GPTA.

Idiopathic pulmonary fibrosis (IPF) is the most common interstitial lung disease.1 It is a chronic, progressive disease that mainly affects older adults.2 In the United States, its prevalence is 10 to 60 cases per 100,000 persons, but that figure can be as high as 494 cases per 100,000 persons above 65 years of age.3,4 Prevalence of the disease in Mexico is not known, but on average, each pneumologist in Mexico diagnoses IPF in 8 patients/year.5 IPF has unfavorable clinical progression, with a current median survival of 3.8 years,4 an elevated hospitalization rate, and a high economic burden on the healthcare system.6
At present, IPF etiology is unclear but risk factors contributing to its development (smoking, drugs, workplace and environmental exposure) have been proposed. Gastroesophageal reflux disease (GERD) is also a widely recognized risk factor.7 Gastric content microaspiration is the mechanism through which GERD increases the risk of IPF, by causing chronic pulmonary epithelial insult that leads to the development of fibrosis.8 On the other hand, IPF has been proposed as a cause of GERD9 due to the fact that the decrease in pulmonary compliance in IPF causes an increase in the negative intrathoracic pressure and the thoracoabdominal pressure gradient (TAPG).10 Given the nature of positive abdominal pressure and the environment of negative thoracic pressure, there is a tendency for gastric fluid to flow from the stomach into the esophagus, with the TAPG determining the magnitude of said flow. Lung transplantation candidates with advanced IPF present with a more negative thoracic pressure, and consequently a higher TAPG, and so are expected to have a higher prevalence of GERD.11,12 In addition, data support an association between GERD and allograft injury in patients that undergo lung transplantation. Therefore, a strategy of early diagnosis and aggressive treatment of GERD is promoted in lung transplant recipients for improving their outcomes.13
The aim of the present study was to document the results of high-resolution esophageal manometry (HREM) and 24 h multichannel intraluminal impedance-pH (MII-pH) monitoring in patients diagnosed with IPF, who were candidates for lung transplantation, and evaluate the association between the TAPG and the prevalence of GERD in our patient cohort.
Patients and methodsA retrospective, descriptive, analytic study was conducted, encompassing a study period of March 2021 to March 2024. HREM and 24 h MII-pH were consecutively performed on 37 patients diagnosed with IPF, as part of the protocol for lung transplantation candidates. The patients were diagnosed at the Pneumology Service of the Hospital Universitario “Dr. José Eleuterio González”, based on the clinical and imaging criteria established for making the IPF diagnosis.
Definitive IPF diagnosis was considered in patients: a) in whom other defined clinical entities or diffuse parenchymatous lung diseases of known cause (environmental or workplace exposure, connective tissue diseases, drug toxicity) were excluded and b) in whom there was a histologic pattern of usual interstitial pneumonia in the examination of lung tissue obtained through surgical lung biopsy and/or radiologic evidence of a pattern of usual interstitial pneumonia in high-resolution computed tomography.14
Adult patients diagnosed with IPF taking part in the lung transplant protocol, referred to the Gastroenterology Service of the Hospital “José Eleuterio González”, and who completed the Chicago 4.0 protocol during HREM and underwent 24 h MII-pH monitoring were included.
Patients with a confirmed diagnosis of GERD prior to their lung disease or patients in whom it was not possible to carry out the complete HREM or 24 h MII-pH protocol were excluded from the study. Likewise, patients with typical GERD symptoms, patients who presented with a type III esophagogastric junction (EGJ) on the HREM, and patients with class 3 obesity at the time of the study were also excluded. If a patient was being treated with an acid suppressant (proton pump inhibitor, H2 receptor agonist, or potassium-competitive acid blocker), the drug was suspended at least 7 days before the HREM and 24 h MII-pH monitoring.
High-resolution esophageal manometry protocolAll patients underwent HREM at the Gastroenterology Service of the Hospital Universitario “Dr. José Eleuterio González”, after fasting for 8 h. Medications that could alter esophageal motility and lower esophageal sphincter (LES) relaxation were suspended at least 7 days before the study. All studies were performed by a neurogastroenterology specialist (GTB), utilizing a solid-state manometry catheter with 36 circumferential pressure transducers (ManoScan™; Sierra Scientific Instruments, Los Angeles, CA, USA) spaced at 1 cm intervals. The catheter was calibrated from 0 to 300 mmHg through externally applied pressure prior to use. The transnasal catheter was then placed to register the pressure from the pharynx to the stomach, enabling the simultaneous recording of the pressure of the upper esophageal sphincter (UES), body of the stomach, intrathoracic pressure, LES, the crural diaphragm (CD), and gastric pressure.
The patients were placed in the decubitus position (at 30º), followed by a 60 s stabilization period. They were told to take 3 deep breaths, followed by a baseline period in which they did not swallow for a period of 30 s. That period was utilized to measure the pressure of the EGJ structures. Following that, 5 ml of water at room temperature were administered, with the patient taking a single swallow, 10 times. The multiple rapid swallow test (5 consecutive swallows of 2 ml of water) was the provocative maneuver. After the multiple rapid swallow maneuver, the patients were told to sit up, followed by a 60 s adaptation period, 3 deep breaths, and a 30 s baseline period. Water was then administered in 5 single swallows of 5 ml of water each. To finish, the 200 ml rapid drink challenge was carried out. All tests were analyzed by the attending specialist (GTB), following the analysis norms and classification of esophageal motor function and the EGJ, suggested by the Chicago 4.0 classification.15 The diagnosis of ineffective esophageal motility (IEM) was defined as > 70% of ineffective swallows or ≥ 50% of failed swallows.15
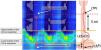
Thoracoabdominal pressure gradient analysisUtilizing the resting phase in the supine decubitus position of the HREM tests, abdominal pressure, thoracic pressure, and the TAPG were evaluated (Fig. 1). Abdominal pressure was defined as pressure 1 cm below the lower edge of the CD during inspiration (referred to as atmospheric pressure) and thoracic pressure was defined as pressure 5 cm above the upper edge of the LES during inspiration (referred to as atmospheric pressure). The TAPG was defined as the difference in pressure between the gastric/abdominal pressure and the negative esophageal/thoracic pressure.16
24 h multichannel intraluminal impedance-pH monitoring
After the HREM study, the upper edge of the LES was located with the patient in the seated position. ZepHr® Impedance/pH Reflux Monitoring System (Diversatek Healthcare) equipment was employed. A ZAN-BG-44 Diversatek Healthcare transnasal MII-pH catheter was placed in each patient. The channel for measuring the esophageal pH was placed 5 cm above the edge of the LES. The minimum study duration was 16 h and the maximum was 24 h. The 24 h MII-pH traces of each patient were analyzed by the specialist (GTB), taking into account the following variables:
- •
Total number of gastroesophageal reflux episodes through impedance. More than 80 reflux episodes was considered abnormal.
- •
DeMeester score (abnormal value > 14.72).
- •
Quantity of reflux episodes that reached the proximal channels.
- •
Acid exposure time (AET) percentage.
The diagnosis of GERD was defined as an AET > 6% of the total MII-pH study duration.17
Statistical analysisA descriptive analysis was carried out. The categorical variables were presented as frequencies (%) and the quantitative variables as medians (q25-q75) or means (± SD). The quantitative variables were compared using the Student’s t test and Mann-Whitney U test, as corresponded. The categorical variables were compared using the Pearson’s chi-square test. The Spearman’s correlation was utilized to test the association between two numerical variables. The statistical analysis was carried out using the SPSS version 22.0 program (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY), and statistical significance was set at a p value < 0.05.
ResultsThirty-seven patients diagnosed with IPF and considered candidates for lung transplant were included. The median patient age was 62 years (range: 52-65). Twenty (54.1%) patients were men and 17 (45.9%) were women. The mean body mass index (BMI) was 25.74 (SD ± 3.96). Sixteen (43.3%) patients were normal weight, 14 (37.8%) were overweight, and 7 (18.9%) had class 1 obesity.
High-resolution esophageal manometryIn our entire cohort, the average of the mean LES pressure was 27 mmHg (SD ± 14.53). Mean LES length was 2.52 cm (SD ± 0.61). Type I EGJ was present in 26 (70.3%) patients and type II EGJ in the rest of the patients. The mean intrathoracic pressure was –4.98 (SD ± 3.88) and the mean intra-abdominal pressure was 11.78 (SD ± 6.94). The mean TAPG was 16.76 mmHg (SD ± 6.68), the mean integrated relaxation pressure (IRP) was 7.77 mmHg (SD ± 4.61), and the mean distal contractile integral (DCI) was 1,530.47 mmHg-cm-s (SD ± 1,210.03). The mean abdominal pressure in the normal weight patients was 11.30 (SD ± 7.69), 11.92 (SD ± 4.40) in the overweight patients, and 11.88 (SD ± 6.31) in the obese patients (p = 0.965). The mean TAPG in normal weight patients was 17.64 (SD ± 6.94), 18.12 (SD ± 4.55) in the overweight patients, and 13.54 (SD ± 6.25) in the obese patients (p = 0.253).
Fourteen (37.8%) patients met the IEM criteria, according to the Chicago 4.0 classification. The rest of the patients were diagnosed with normal esophageal motility. The patients with IEM had a mean TAPG of 15.23 (SD ± 6.52) versus 17.69 (SD ± 6.74) in the patients with normal esophageal motility (p = 0.284). Likewise, the patients with IEM had a median AET of 3.20 (range: 1.42-4.90) versus 0.50 (range: 0.2-2.90) in the patients with normal esophageal motility (p = 0.022). Table 1 describes the remaining manometric findings in the patients with IEM.
Clinical and manometric characteristics of patients with idiopathic pulmonary fibrosis (comparison between patients with IEM and normal esophageal motility).
| Variable | IEM | Normal peristalsis | p value |
|---|---|---|---|
| n = 14 | n = 23 | ||
| Body mass index | 24.27 (±3.28) | 26.50 (±4.14) | 0.132 |
| Mean LES pressure (mmHg) | 19.60 (±16.07) | 29.64 (±13.01) | 0.045 |
| Minimal respiratory LES pressure (mmHg) | 5.31 (±4.66) | 17.82 (±12.13) | 0.002 |
| LES length (cm) | 2.41 (±0.58) | 2.55 (±0.61) | 0.490 |
| Intrathoracic pressure (mmHg) | -7.45 (±6.99) | -3.47 (±2.91) | 0.139 |
| Intra-abdominal pressure (mmHg) | 7.77 (±5.87) | 14.21 (±6.48) | 0.005 |
| Thoracoabdominal pressure gradient (mmHg) | 15.23 (±6.52) | 17.69 (±6.74) | 0.284 |
IEM: ineffective esophageal motility; LES: lower esophageal sphincter.
In our patient cohort, the mean percentage of exposure time to a pH < 4 was 3.02% (SD ± 4.17). The mean of the total number of reflux episodes detected by impedance was 44.51 (SD ± 22.75). The mean of proximal reflux episodes by impedance was 25.88 (SD ± 19.37). Only three (8.1%) patients presented with more than 80 reflux episodes during the study. The mean DeMeester score was 11.21 (SD ± 15.28). Eight (21.6%) patients presented with an abnormal DeMeester score. Four (10.8%) patients had acid exposure between 4 and 6% and 5 (13.5 %) patients had abnormal acid exposure (pH < 4, at least 6% of the total time of the study). Of the 5 patients with abnormal acid exposure, 2 (14.3%) had IEM (p = 0.915). The mean LES pressure in patients with an AET > 6% was 20.62 (SD ± 9.79) versus 26.66 (SD ± 15.47) in patients with an AET ≤ 6% (p = 0.406).
Thoracoabdominal pressure gradient and gastroesophageal reflux diseaseThe patients with abnormal AET had a mean TAPG of 14.66 (SD ± 4.89) versus 17.09 (SD ± 6.92) in patients with an AET < 6% (p = 0.457). The patients with more than 80 reflux episodes detected by impedance had a mean TAPG of 12.73 (SD ± 5.26) versus 17.12 (SD ± 6.73) in patients with fewer reflux episodes (p = 0.282). The patients with an abnormal DeMeester score had a mean TAPG of 6.86 (SD ± 5.30) versus 16.73 (SD ± 7.09) in the patients with a normal DeMeester score (p = 0.964). There was a negative correlation between the number of proximal reflux episodes and the TAPG (rs = –0.235, p = 0.248).
Table 2 describes the rest of the manometric findings in the patients with normal and abnormal acid exposure.
Clinical and manometric characteristics of patients with idiopathic pulmonary fibrosis (comparison between patients with normal and abnormal AET).
| Variable | AET > 6% n = 5 | AET ≤ 6% n = 32 | p value |
|---|---|---|---|
| Body mass index | 25.04 (±3.73) | 25.87 (±4.05) | 0.674 |
| Mean LES pressure (mmHg) | 20.62 (±9.79) | 26.66 (±15.47) | 0.406 |
| Minimal respiratory LES pressure (mmHg) | 10.94 (±10.91) | 13.42 (±12.79) | 0.684 |
| LES length (cm) | 2.46 (±0.70) | 2.50 (±0.59) | 0.866 |
| Intrathoracic pressure (mmHg) | -5.84 (±4.26) | -4.85 (±4.08) | 0.798 |
| Intra-abdominal pressure (mmHg) | 8.82 (±5.40) | 12.24 (±7.11) | 0.312 |
| Transdiaphragmatic gradient (mmHg) | 14.66 (±4.89) | 17.09 (±6.92) | 0.457 |
AET: acid exposure time; LES: lower esophageal sphincter.
The aim of the present study was to describe the manometric and impedance-pH monitoring findings in IPF patients who were candidates for lung transplantation and to evaluate the association between the TAPG and GERD. Our research was motivated by the recently reported high incidence of GERD in patients with IPF, ranging from 60 to 90% in developed countries,18–22 due mainly to changes in thoracic pressure, causing a higher TAPG and subsequent greater acid reflux exposure.23–25 However, the prevalence in our study cohort was significantly lower than that previously reported in the literature (13.8%). A possible explanation could be that we excluded patients with independent risk factors for GERD (hiatal hernia,26 smoking,27,28 elevated BMI29) from our study. We also studied highly selected patients with IPF (for example, ruling out patients with a prior reflux diagnosis) to evaluate whether altered TAPG values could be a determining factor in abnormal AET in that patient population. Few studies evaluate the influence of the TAPG on the development of abnormal AET in patients with IPF, who are candidates for lung transplantation, and according to the low prevalence, it is likely that the alterations in the thoracoabdominal pressure dynamics are simply an epiphenomenon.
An elevated TAPG has been proposed to facilitate gastroesophageal reflux by overcoming EGJ pressure. The TAPG tends to be elevated in obese patients as a consequence of an increase in intra-abdominal pressure,30,31 as well as in patients with severe lung diseases, due to the increase in intrathoracic pressure.11,24 Importantly, unlike the findings of other studies,30,31 BMI had no significant influence on the intra-abdominal pressure or TAPG of our patients. The TAPG also had no significant influence on AET, the number of reflux episodes, or the DeMeester score of our patients, concurring with information from previous reports.16,30–32
The EGJ is known to function as an anatomic and physiologic barrier against gastroesophageal reflux. The evaluation of its components through HREM has gained relevance in recent years, given that a competent EGJ has been posited to act as an adjuvant against gastroesophageal reflux. According to the Lyon 2.0 consensus,17 the manometric findings of hiatal hernia, a weak EGJ (DCI below 25 mmHg-cm),15 and IEM/absent contractility are supporting evidence for the diagnosis of GERD.
Esophageal motor alterations are frequent in IPF. IEM is the commonly associated finding in those patients, with a prevalence ranging from 17 to 45% in recent studies.33,34 IEM was present in 38% of our patients. Said disorder has been associated with worsening of GERD severity and a higher number of proximal reflux episodes,33 due to the inadequate esophageal elimination of gastric reflux. The AET in our patients with IEM was significantly higher than that in the patients with normal esophageal motility, but the prevalence of esophageal AET and the mean proximal reflux events were not.
Despite not reaching statistical significance, intrathoracic pressure negativity was double in the patients with IEM, compared with the patients with normal motility, but the TAPG was similar in the two groups. This was because the intra-abdominal pressure was significantly higher in the patients with normal esophageal motility, possibly due to their higher BMI.
Lung transplantation is crucial in the treatment of IPF and provides an approximate 5-year survival rate of 55%, post-transplant.35 Chronic graft dysfunction is the main cause of death in those patients and predominantly manifests as obliterating bronchiolitis.36,37 The diagnosis of IEM in lung transplant candidates has recently been associated with an increase in acute graft rejection.34 Given its frequent diagnosis in our cohort, IEM should be taken into consideration, given that it is possible that said patient subgroup would benefit from a stricter follow-up, thus avoiding early postoperative graft rejection.
Our study results were limited by the relatively small size of the sample and the fact that the findings corresponded to a highly selected population from a single center. In addition, there was no available information for evaluating the usefulness of mean nocturnal baseline impedance or symptomatic association in our patients. Even though we described alterations prior to lung transplantation, it would be interesting to know the prevalence of said alterations and whether they are permanent or reversible. Despite those limitations, the detailed description of the manometric and 24 h MII-pH monitoring findings in our patients provides valuable information on their influence on the development of GERD in patients with IPF.
In conclusion, our findings suggest greater attention should be paid to esophageal motility in patients with IPF, given that nearly 40% of our patients with IPF, who were candidates for lung transplantation, had IEM. Nevertheless, the prevalence of GERD was low and not associated with changes in the TAPG. Prospective, post-transplantation studies with larger samples are needed to corroborate our findings.
Financial disclosureNo financial support was received in relation to this study/article.
Ethical considerationsPatients underwent the study protocol prior to lung transplantation. The present study describes the clinical findings in that group of patients who were collected anonymously and retrospectively; therefore, neither informed consent nor ethics committee authorization were required.
This manuscript contains no individual names or results.
The authors declare that there is no conflict of interest.

