


Cirrhosis of the liver is known for its high risk of mortality associated with episodes of acute decompensation. There is an even greater risk in patients that present with acute-on-chronic liver failure. The identification of patients at higher risk for adverse outcomes can aid in making the clinical decisions that will improve the prognosis for these patients.
AimsTo determine in-hospital mortality and evaluate the epidemiologic and clinical characteristics of patients with cirrhosis of the liver seen at a tertiary referral hospital.
MethodologyA descriptive, observational, cohort study was conducted on adult patients with cirrhosis of the liver, admitted to a tertiary care center in Bucaramanga, Colombia, within the time frame of March 1, 2015 and February 29, 2016.
ResultsEighty-one patients with a mean age of 62 years were included in the study. The main etiology of the cirrhosis was alcoholic (59.3%). In-hospital mortality was 23.5% and the most frequent cause of death was septic shock (68.4%), followed by hypovolemic shock (10.5%). A MELD score≥18, a leukocyte count>12,000/ul, and albumin levels below<2.5g/dl were independent factors related to hospital mortality.
ConclusionsIn-hospital mortality in cirrhotic patients is high. Sepsis and bleeding are the 2 events leading to acute-on-chronic liver failure and death. A high MELD score, elevated leukocyte count, and low level of albumin are related to poor outcome during hospitalization. Adjusted prevention-centered public health measures and early and opportune diagnosis of this disease are needed to prevent the development of complications and to improve outcome in cirrhotic patients.
La cirrosis hepática es reconocida por el alto riesgo de mortalidad asociada a los episodios de descompensación aguda; este riesgo se incrementa aun más en el caso de pacientes que desarrollan insuficiencia hepática crónica agudizada. Identificar a aquellos pacientes con mayor riesgo de desenlaces adversos puede ayudar en la toma de decisiones clínicas encaminadas a mejorar su pronóstico.
ObjetivoDeterminar la mortalidad hospitalaria y evaluar las características epidemiológicas y clínicas de pacientes con cirrosis hepática atendidos en un hospital de tercer nivel.
MetodologíaSe realizó un estudio descriptivo observacional de cohorte, de pacientes adultos con cirrosis hepática admitidos en un hospital de tercer nivel en Bucaramanga, Colombia, entre el 1 de marzo de 2015 y el 29 de febrero de 2016.
ResultadosSe incluyeron 81 pacientes con edad promedio de 62 años. La principal etiología de cirrosis fue alcohólica (59.3%); la mortalidad hospitalaria fue del 23.5% siendo la causa más frecuente de muerte el choque séptico (68.4%), seguido del choque hipovolémico (10.5%). Fueron factores independientes relacionados con mortalidad hospitalaria un puntaje MELD≥18, leucocitos>12.000/ul y albúmina<2.5g/dl.
ConclusionesLa mortalidad hospitalaria en pacientes cirróticos es elevada, siendo la sepsis y el sangrado los 2 eventos precipitantes de insuficiencia hepática crónica agudizada y muerte. Un puntaje MELD alto, leucocitos elevados y albúmina baja están relacionados con un pobre desenlace durante la hospitalización. Es necesaria la adecuación de medidas de salud pública encaminadas a la prevención, diagnóstico temprano y oportuno de esta enfermedad, para evitar el desarrollo de complicaciones y mejorar el pronóstico en pacientes cirróticos.
Cirrhosis of the liver is currently one of the main public health problems worldwide,1 and is consolidated among the 10 first causes of general mortality in lower middle income countries.2
The development of complications secondary to portal hypertension and liver failure, which are outcome markers, occurs in up to 15% of cirrhotic patients each year.3 These complications include ascites, variceal gastrointestinal bleeding, infection, and hepatic encephalopathy. Compensated cirrhosis with no esophageal varices has a low annual mortality rate, close to 1%, whereas the development of esophageal varices increases the risk for death up to 3.4% per year. Mortality drastically increases, once there is some kind of decompensation, and the development of ascites increases the mortality rate to 20% per year. The presence of severe hepatic encephalopathy supposes an annual mortality rate of 54%, and after the first episode of variceal gastrointestinal bleeding, it can reach 57% in the first year of the event.4 The development of acute decompensation in cirrhosis usually is associated with a precipitating event, such as bacterial or viral infections, surgery, trauma, and active alcoholism, among others. Even though many patients respond to standard treatment and return to a compensated state, one third of patients develop hepatic or extrahepatic organ failure, worsening their prognoses. This condition has been named acute-on-chronic liver failure. It is a recently recognized syndrome, characterized by acute decompensation of cirrhosis associated with hepatic and extrahepatic organ failure that conditions a high short-term mortality rate (30-40% at 28 days). This entity presents mainly in patients with cirrhosis of alcoholic etiology and the most frequent triggering factor is infection.3,5 The development of acute-on-chronic liver failure occurs in the context of systemic inflammation, whose severity is correlated with the degree of organ failure and mortality.
Different Latin American studies have shown high in-hospital mortality rates in cirrhotic patients, reaching 24.2% in the general ward,6 but increasing up to 86% in patients requiring management in intensive care units,7 demonstrating the poor outcome associated with cirrhosis. Epidemiologic data on cirrhosis of the liver are limited in the regional literature. There are few studies that provide demographic, clinical, or prognostic information on these patients, and the literature that offers data on factors associated with cirrhosis-related mortality is also limited. It is necessary to study this disease, so that more can be learned about its epidemiology, which will, in turn, lend support to clinical and healthcare decision-making, as well as to the creation and adaptation of policies based on facts. Therefore, the aim of the present study was to determine in-hospital mortality and evaluate the clinical and epidemiologic characteristics of patients with cirrhosis of the liver seen at a tertiary care hospital.
Materials and methodsStudy design and populationA descriptive, observational, cohort study was conducted within the time frame of March 1, 2015 and February 29, 2016. The data collection center was the Hospital Universitario de Santander, a tertiary care referral center serving the Northeast region of Colombia. Patients that were above 18 years of age, seen at the emergency department and hospitalized, with histopathologic diagnosis of cirrhosis of the liver, or that fulfilled a compatible combination of clinical, biochemical, and imaging study findings8 were enrolled in the study. Patients with a past history of liver transplantation were excluded. Non-probabilistic consecutive sampling was carried out and a total of 81 patients were included in the study during the collection period.
Data collectionThe good clinical practice and human experimentation norms were met during the development of the study. All patients gave their authorization to participate in the study through written statements of informed consent. The demographic and clinical variables of the participants were collected through a survey applied either to the patient or to an accompanying guardian upon hospital admission. The referred data were corroborated through a review of the previous medical histories, when available. Clinical, paraclinical, and imaging study data were taken from the medical history of the hospitalization. Intrahospital complications, hospital stay, the patient's condition upon release, and cause of death in the event a patient died, were registered. The Model for End-stage Liver Disease (MELD) and Child-Pugh scores were calculated, which are predictive mortality models in cirrhotic patients.9,10
Potential memory bias was considered and dealt with through corroborating the referred data with the former medical record of each patient. Standard norms were established for maintaining homogeneity in the radiology reports and the Doppler ultrasound findings.
Statistical analysisThe statistical analysis was carried out using the STATA® 11 program. Measures of central tendency were employed for the quantitative variables and measures of frequency for the qualitative variables, with their respective dispersion measures. The Student's t test was used for comparing the parametric variables and the chi-square test or the Fisher's test was used for the nonparametric variables. Variables that could be related to hospital mortality were evaluated through a multivariate logistic regression analysis.
Ethical considerationsThe study was designed in accordance with the national and international ethical guidelines for biomedical research on humans (the Helsinki Declaration, the Belmont Report, and the international guidelines prepared by the International Organizations of the Medical Sciences Council) and was approved by the institutional scientific research ethics committee.
ResultsOf the 121 potentially eligible patients, 97 met the eligibility criteria. Sixteen of those patients were not included due to the inability to obtain their informed consent or because they refused to participate in the study. This left a total of 81 study participants and none of them dropped out.
The mean age was 62 years, 64.2% of the participants were men, and 73% came from urban areas. The most frequent etiology of cirrhosis of the liver was alcoholic (59.3%), followed by autoimmune causes (6.2%). Table 1 summarizes the general characteristics of the participants.
General characteristics of the study participants.
| Characteristic | Survivors (n = 62) | Non-survivors (n = 19) | p value |
|---|---|---|---|
| Age (years), X | 62.2 | 61.5 | 0.841 |
| Male sex, n (%) | 36 (58) | 15 (79) | 0.11 |
| Residence in urban zone, n (%) | 44 (71) | 15 (79) | 0.57 |
| Educational level (years), Me | 3 | 4 | 0.59 |
| Illiteracy, n (%) | 13 (21) | 6 (31.5) | 0.33 |
| Comorbidities | |||
| High blood pressure, n (%) | 27 (43.5) | 5 (26.3) | 0.28 |
| Diabetes mellitus, n (%) | 16 (25.8) | 3 (15.8) | 0.54 |
| Obesity, n (%) | 10 (16.1) | 1 (5.2) | 0.44 |
| Alcohol consumption, n (%) | 39 (62.9) | 15 (79) | 0.055 |
| Quantity of consumption (g/day), Me | 23.8 | 22.5 | 0.89 |
| Cirrhosis etiology | |||
| Alcoholic, n (%) | 36 (58.1) | 12 (63.2) | 0.79 |
| Undetermined, n (%) | 12 (19.3) | 4 (21.1) | 0.96 |
| Autoimmune, n (%) | 5 (8.1) | 0 (0) | 0.58 |
| NASH, n (%) | 4 (6.4) | 0 (0) | 0.56 |
| Hepatitis B, n (%) | 1 (1.6) | 2 (10.5) | 0.13 |
| Hepatitis C, n (%) | 1 (1.6) | 1 (5.2) | 0.8 |
| Others, n (%) | 3 (4.8) | 0 (0) | 0.86 |
g: grams; Me: median; n: number; NASH: nonalcoholic steatohepatitis; X: mean.
The prevalence of complications identified during hospitalization was ascites in 56.8%, hepatic encephalopathy in 27.2%, variceal upper gastrointestinal bleeding in 17.3%, spontaneous bacterial peritonitis in 4.9%, hepatorenal syndrome in 1.2%, and hepatopulmonary syndrome in 1.2%. A total of 34.6% of the participants presented with some grade of kidney failure upon hospital admission.
The hospital mortality rate was 23.5% (19 participants). The most frequent cause of death was septic shock (68.4%), followed by hypovolemic shock (10.5%), liver carcinoma (10.5%), and acute renal failure (5.3%). The most frequent initial infection causing sepsis was urinary infection (30.1%), followed by soft tissue infection (23.1%), pulmonary infection (15.4%), and spontaneous bacterial peritonitis (7.7%). No significant differences were found in the distribution of age, sex, region of birth, educational level, or prevalence of comorbidities. There were also no significant differences in relation to alcohol consumption between survivors and non-survivors, and the etiology distribution was similar between those 2 groups. The most frequent etiology was alcoholic in both groups, followed by that of undetermined causes.
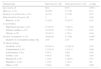
The MELD score (23 vs 13 points p = 0.001) and quantitative Child-Pugh score (10 vs 8.1 points p = 0.006) were significantly higher in the non-surviving patients, compared with the survivors. The median levels of leukocytes (12,680 vs 6,120/ul; p < 0.001), creatinine (1.16 vs 0.71mg/dl; p = 0.034), total bilirubin (2.99 vs 1.6mg/dl; p = 0.036), and the INR (1.67 vs 1.28; p = 0.003) were also significantly higher in the non-survivors and the mean albumin level (2.01 vs 2.67g/dl; p < 0,001) was significantly lower in the non-survivor group (Table 2).
Comparison of clinical data and laboratory variables upon admission.
| Findings | Survivors (n = 62) | Non-survivors (n = 19) | p value |
|---|---|---|---|
| Hospital stay (days), Me | 9 | 6 | 0.11 |
| MELD score, X | 13 | 23 | 0.001 |
| MELD ≥ 18, n (%) | 9 (15.5) | 12 (70.8) | <0.000 |
| Quantitative Child-Pugh score, X | 8.1 | 10 | 0.006 |
| Child-Pugh A, n (%) | 10 (17.2) | 0 (0) | 0.1 |
| Child-Pugh B, n (%) | 34 (58.6) | 7 (43.7) | 0.4 |
| Child-Pugh C, n (%) | 14 (24.2) | 9 (56.3) | 0.034 |
| Albumin (g/dl), X | 2.67 | 2.01 | <0.000 |
| Leukocytes (number/ul), Me | 6,120 | 12,680 | <0.000 |
| INR, Me | 1.28 | 1.67 | 0.003 |
| PT (seconds), Me | 15.9 | 19.5 | 0.013 |
| Creatinine (mg/dl), Me | 0.71 | 1.16 | 0.034 |
| Bilirubin (mg/dl), Me | 1.6 | 2.99 | 0.036 |
| AST (U/l), Me | 47 | 68 | 0.06 |
ALT: alanine aminotransferase; AST: aspartate aminotransferase; INR: international normalized ratio; Me: median; MELD: Model for End-stage Liver Disease; n: number; PT: Prothrombin time; X: mean.
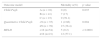
In the logistic regression analysis with mortality as the outcome, hospital mortality was significantly higher in the group of participants that were admitted due to an infectious process, compared with those that were admitted for other causes (47.4 vs 16.1%; OR: 4.68, CI: 1.5-14.4). Mortality was also higher in patients with creatinine levels > 1mg/dl, compared with those with creatinine levels ≤ 1mg/dl (39.2 vs 15.1%; OR: 3.6, CI: 1.25-10.5) and in patients with bilirubin levels > 2mg/dl, compared with those with bilirubin levels ≤ 2mg/dl (33.3 vs 12.8%; OR: 3.4; CI: 1.05-10.9). In regard to outcome models in cirrhosis, mortality increased the higher the Child-Pugh classification (A: 0%, B: 17%, C: 39.1%; OR: 3.54, CI: 1.3-10). In addition, mortality was significantly higher in the group of participants with a MELD score ≥ 18, compared with those with a score < 18 (57.1 vs 9.2%; OR: 13; CI: 3.7-46.1) (Table 3).
Outcome models and hospital mortality.
| Outcome model | Mortality n(%) | p value | |
|---|---|---|---|
| Child-Pugh | A (n = 10) | 0 (0) | 0.035 |
| B (n = 41) | 7 (17) | ||
| C (n = 23) | 9 (39.1) | ||
| Quantitative Child-Pugh | <9 (n = 35) | 1 (2.86) | 0.004 |
| ≥9 (n = 39) | 15 (38.4) | ||
| MELD | <18 (n=54) | 5 (9.2) | < 0.0001 |
| ≥18 (n=21) | 12 (57.1) | ||
MELD: Model for End-stage Liver Disease; n: number
According to the multivariate logistic regression analysis adjusted by age and sex, the variables that were independently related to hospital mortality were a MELD score ≥ 18 (OR: 7.4; CI: 2.1-26.6), albumin value < 2.5g/dl (OR: 6.7; CI: 1.5-32.5), and a leukocyte count > 12,000/ul upon admission (OR: 11.6; CI: 2.6-46.5) (p < 0.05 for those 3 variables) (Table 4).
Multivariate logistic regression analysis of factors related to hospital mortality.
| Variable | Raw OR (95% CI) | p | Adjusted OR (95% CI) | p |
|---|---|---|---|---|
| MELD ≥ 18 | 13 (3.7 - 46.1) | 0.000 | 7.4 (2.1 - 26.6) | 0.013 |
| Albumin < 2.5 g/dl | 13.3 (2.7 - 64) | 0.001 | 6.7 (1.5 - 32.5) | 0.037 |
| Leukocytes > 12,000/ul | 10.3 (3 - 35.6) | 0.000 | 11.6 (2.6 - 46.5) | 0.014 |
CI: confidence interval; MELD: Model for End-stage Liver Disease; OR: odds ratio. The cutoff point values presented are those at which the variables gave the best OR in relation to mortality.
Cirrhosis of the liver is a worldwide public health problem,1,2 with a commonly underestimated social and economic impact. The epidemiologic information in our environment is limited and, in fact, quite scarce, given that there is very little clinical research on this pathology. Greater knowledge as to the clinical progression, hospital attention, and prevention of complications could result in the development of specific measures for its control.11
It has been recognized that in-hospital mortality in cirrhotic patients with acute decompensation is high, and it is higher than that of patients with other diseases.12 Acute-on-chronic liver failure is a recently identified entity characterized by acute decompensation of cirrhosis associated with organ failure and a very high in-hospital mortality rate.3,5 Its identification is crucial for establishing outcome, and in turn, offering patients the appropriate medical management.
The characteristics of the patients with cirrhosis seen at our hospital center embodied the group of patients with acute-on-chronic liver failure, given that the main etiology of cirrhosis was alcoholic, with infectious processes as the triggering factor of decompensation and high in-hospital mortality.3–5
There is limited regional data on hospital mortality in cirrhotic patients. Two studies in Peru, one in Ecuador, and one in Brazil described in-hospital mortality rates similar to the results of our study (23.8, 19.8, 23.7, and 24.2%, respectively),6,13–15 whereas another Peruvian study reported a much lower mortality rate (5.1%).11 The fact that there are numerous factors that determine hospital mortality must be taken into account, and they include disease stage, complications, associated comorbidities, infections, organ dysfunction, acute-on-chronic liver failure, and clinical status upon admission.4,16,17 The mortality rate in cirrhotic patients whose condition requires management in the intensive care unit can reach 86%.7,18
In our patient cohort, hospital mortality was 23.5%, and infectious processes were the most frequent cause of death (68.4%). This finding is related to the cirrhosis-associated state of immunosuppression, which is secondary to a reduced capacity of the cirrhotic liver to remove endotoxins and bacteria, a decrease in the activity of the endothelial reticulum system, immunoglobulin and complement alterations, and a lower opsonic capacity of plasma and fluid ascites.12,19–21 This results in a high rate of infections, increased hospital stay, and greater mortality in infected cirrhotic patients.20,22 Different studies have identified infections as the main cause of death in patients with cirrhosis, with variable percentages, depending on the group studied: Valenzuela et al.14 (70%), Levesque et al.7 (81.6%), Malpica-Castillo et al.13 (31.5%), Houissa et al.23 (56.7%), and Oliveira et al.6 (63.9%). Cirrhosis has also been identified as a risk factor for the development of sepsis and hospital mortality.24 All of the above demonstrates the importance of the identification and early treatment of the infectious processes in this type of patient, justifying the use of prophylactic measures when indicated, given that they have been shown to reduce the risk for infection and associated mortality.25,26 In our hospital center, the patients with cirrhosis received routine prophylactic antibiotics upon admission, except in cases of upper gastrointestinal bleeding.
In our study, the group of patients that died had the highest values of creatinine, bilirubin, INR, and leukocytes and the lowest values of albumin, compared with the group of survivors. This was related to greater liver dysfunction, greater multiorgan involvement, or greater infectious process severity in the patients that died, conditioning a worse outcome.17 Different studies have established certain laboratory variables as independent risk factors for mortality in cirrhosis that include creatinine, albumin, bilirubin, prolonged INR, and infections.6,7,23,27,28 In our cohort, the results of a multivariate logistic regression analysis described a MELD ≥ 18, a leukocyte count greater than 12,000/ul, and an albumin level under 2.5g/dl as independent factors related to hospital mortality. The odds ratios were greater than 5 for the 3 variables, but the confidence intervals were wide, which could be explained by the small sample size.
There are various outcome models in cirrhosis that combine clinical or laboratory variables for the purpose of predicting mortality. The MELD and Child-Pugh scores are the most widely used classic models that can predict mortality at 3 months and at one year, respectively.9,10,29,30 Even though they have been used to predict hospital mortality,13,31,32 the models that are generally used in intensive care, the Sequential Organ Failure (SOFA), Acute Physiology and Chronic Health Evaluation (APACHE) II and III, and the Simplified Acute Physiologic Score (SAPS) II have been shown to have better mortality predictive capacity in critical stage cirrhotic patients.7,16,32,33 The aim of the present study was not to evaluate or compare the capacity of the outcome models to predict hospital mortality in cirrhosis, and thus we cannot provide a concept of performance in the prediction of mortality with the models we used. We suggest that studies in our population be conducted that aim to evaluate and compare the performance of these models.
Finally, we consider that the morbidity and mortality data presented herein demonstrate the importance of cirrhosis of the liver in our environment, given its great social and economic burden. These data suggest the need for new public health measures for the prevention and early and opportune diagnosis of this disease, so that the development of complications that darken the outcome in patients with cirrhosis can be prevented and delayed.
One of the limitations of the present work was the fact that the study population was patients hospitalized in a single hospital center and therefore the reported data cannot be generalized for the entire population or for cirrhotic patients in the outpatient realm. It should be mentioned that the health regimens of the majority of the patients seen at our institution are subsidized, and their socioeconomic characteristics are different from patients under other health regimens. Because of the study's observational design, the information collected from the medical records and the paraclinical tests carried out during hospitalization were limited to those ordered and recorded by the attending physicians. Lastly, an important limitation was the size of our sample, which could have restricted the level of confidence in the estimations made.
ConclusionsIn-hospital mortality in patients with cirrhosis of the liver is high, and sepsis and bleeding are the 2 precipitating events of acute-on-chronic liver failure and death. A high MELD score, an augmented leukocyte count, and a low level of albumin are related to poor outcome during hospitalization. The adaptation of public health measures directed towards prevention and early and opportune diagnosis of this disease is necessary to prevent the development of complications and improve outcome in cirrhotic patients.
Ethical disclosureProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Zubieta-Rodríguez R, Gómez-Correa J, Rodríguez-Amaya R, Ariza-Mejia KA, Toloza-Cuta NA. Mortalidad hospitalaria en pacientes cirróticos en un hospital de tercer nivel. Revista de Gastroenterología de México. 2017;82:203–209.
See related content at DOI: http://dx.doi.org/10.1016/j.rgmxen.2017.04.006, Buganza-Torio E, Montano-Loza AJ. Hospital mortality in cirrhotic patients at a tertiary care center in Latin America. Rev Gastroenterol Méx. 2017;82:201–2.


www.publicationethics.org.