



Appearing in the year 2000, capsule endoscopy revolutionized the study of the small bowel. It is the gold standard for the study of small bowel bleeding and is considered a safe procedure.
ObjectiveThe aim of the present study was to identify the indications for, diagnostic yield, and safety of capsule endoscopy in Mexican patients.
Materials and methodsA descriptive study was conducted on the first 500 small bowel capsule endoscopies performed at a tertiary care hospital center in Mexico City. Sex, age, type of video camera employed, bowel transit time, referral diagnosis, and capsule endoscopy findings and complications were registered.
ResultsMean patient age was 55years (±17.63) and 57.9% of the cases were women. Complete visualization of the small bowel was achieved in 420 capsule endoscopies (84%). Mean bowel transit time was 272.25minutes (±114.86). The most common indications for the procedure were small bowel bleeding (65.2%), search for neoplasia (14.4%), and Crohn's disease (10.2%). The presence of ulcers was the most common finding in small bowel bleeding (24.8%), followed by angioectasias (18.9%). Capsule retention was the only complication and it presented in 11 patients (2.2%).
ConclusionsCapsule endoscopy is a safe and efficacious method for studying the small bowel. The results obtained in Mexican patients were similar to those described in the international literature. The present case series is the largest reported in a Mexican population.
La cápsula endoscópica (CE) revolucionó el estudio del intestino delgado desde su aparición en el año 2000. Es el estándar de oro para el estudio de la hemorragia de intestino delgado (HID) y es considerado un estudio seguro.
ObjetivoIdentificar las indicaciones, el rendimiento diagnóstico y la seguridad de la CE en pacientes mexicanos.
MétodosEstudio descriptivo de las primeras 500CE de intestino delgado colocadas en un centro de tercer nivel en México. Se registró el sexo, la edad, el tipo de CE empleada, el tiempo de tránsito intestinal, el diagnóstico de envío, así como los hallazgos y las complicaciones que se presentaron durante la aplicación de las CE.
ResultadosLa media de edad fue de 55años (±17.63) y el 57.9% eran femeninos. Se logró visualización completa del intestino delgado en 420CE (84%). La media del tiempo de tránsito intestinal fue 272.25min (±114.86). Las indicaciones más comunes fueron HID (65.2%), búsqueda de neoplasia (14.4%) y enfermedad de Crohn (10.2%). La presencia de úlceras fue el hallazgo más común en HID (24.8%), seguido de angioectasias (18.9%). La única complicación presentada fue la retención, y se presentó en 11 pacientes (2.2%).
ConclusionesLa CE es un método eficaz y seguro para el estudio del intestino delgado. Los resultados obtenidos en pacientes mexicanos fueron similares a los reportados en la literatura internacional. Esta es la mayor experiencia reportada en población mexicana.
Capsule endoscopy (CE) revolutionized the endoscopic study of the small bowel, an area that was inaccessible by other endoscopic methods. The first publication related to that new technology appeared in the year 2000.1 Since then, the usefulness of CE for the study of the small bowel has been on the rise. The most common indications for said procedure are small bowel bleeding (SBB) and Crohn's disease (CD).2 Other indications are anemia, the search for tumors, intestinal polyposis, celiac disease, and abdominal pain.3 The usefulness of CE is currently being studied in pathologies such as acromegalia4 and graft-versus-host disease (GVHD).5,6
CE is considered the gold standard for the diagnosis of certain pathologies of the small bowel. Such is the case with SBB, in which it has a diagnostic capacity of 61.7% (95% CI: 47.3-76.1) when the pathology is overt.7 In the case of occult SBB, its diagnostic capacity decreases to 53% (95% CI: 41-65).8 The success of CE lies primarily in its safety. The main complication related to the procedure is the retention of the capsule in the bowel, varying from 1.4% in patients with SBB to 13% in those diagnosed with CD.9
The aim of the present study was to describe the experience with CE at a tertiary care hospital in Mexico.
Materials and methodsA retrospective, observational, descriptive, cross-sectional study was conducted that included the first 500 CEs performed at the Endoscopy Service of the Specialty Hospital of the Centro Médico Nacional Siglo XXI of the Instituto Mexicano del Seguro Social within the time frame of August 2008 to September 2018. The variables of sex, age, type of video capsule, bowel transit time, indication, findings, and complications that presented during the CE were registered. The Pillcam (Given Imaging, Yokneam, Israel) small bowel capsule, generations SB, SB2, and SB3, were utilized, as well as the OMOM Smart Capsule 2 (Jinshan Science and Technology Company, Chongqing, China). All the patients underwent bowel preparation with 4 liters of polyethylene glycol the day before the study and fasted for 8hours before the procedure. The content of the video cameras was reviewed by two endoscopists at a velocity of 10 to 12 images per second. Capsule retention was defined as the capsule remaining in the small bowel for more than 15 days. The SPSS version 22 program was employed to obtain the mean as the measure of central tendency when the quantitative variables had a normal distribution and the median as a measure of central tendency when the variables had a central distribution. The program was also used to determine the frequencies and percentages of the qualitative variables.
The present study was exempt from examination by the review committee of the Specialty Hospital of the Centro Médico Nacional Siglo XXI due to its retrospective design, only including the analysis of the results of the CEs. The study was conducted in compliance with the Declaration of Helsinki.
ResultsIn the present study, 500 video capsules were placed in 469 patients. Two capsules were placed in 31 patients. Repeat procedures were indicated in 24 cases of SBB and 7 cases of CD. Median patient age was 55 years (± 17.63), with a range of 9 to 93 years. A total of 57.9% of the patients were female. Complete visualization of the small bowel was achieved in 420 CEs (84%). Mean bowel transit time for the video capsule was 272.25min (± 114.86). In 15 cases (3%), the video cameras had to be pushed by means of endoscopy, when gastric transit time was greater than 60min or the capsule could not be swallowed. There was at least one finding in 378 CEs (75.6%). The most widely used video capsule was the SB3 (50.4%), followed by the SB2 (23.6%), SB (22%), and OMOM (4%).
The most common indication for CE was SBB (65.2%), followed by the search for neoplasia (14.4%), and CD (10.2%). Other referral diagnoses were chronic diarrhea (5.6%), GVHD (2.8%), intestinal polyposis (1.4%), and abdominal pain (0.4%). In the patients with SBB, a finding was made in 79.8% of the CEs. There were findings in 80.1% of the cases with overt SBB and in 77.1% of the occult cases, with no statistically significant difference between the two (p=0.684) (Table 1). The most common lesions in the cases of SBB were ulcers in 24.8%, followed by angioectasias in 18.4% (Table 2).
Indications for, positive findings, bowel transit time, and complications of the capsule endoscopies.
| Indication | n (%) | Positive finding (%) | BTT (min) | Complications (%) |
|---|---|---|---|---|
| Overt SBB | 291 (58.2%) | 233 (80.1%) | 277.46 (± 122.84) | 8 (2.7%) |
| Search for neoplasia | 72 (14.4%) | 41 (56.9%) | 281.33 (± 114.86) | 1 (1.4%) |
| CD | 51 (10.2%) | 38 (74.5%) | 230 (± 96.90) | 1 (2.0%) |
| Occult SBB | 35 (7%) | 27 (77.1%) | 255.34 (± 109.35) | 1 (2.9%) |
| Chronic diarrhea | 28 (5.6%) | 22 (78.6%) | 287.04 (± 113.17) | 0 |
| GVHD | 14 (2.8%) | 10 (71.4%) | 288.50 (± 86.48) | 0 |
| Polyposis | 7 (1.4%) | 6 (85.7%) | 263.14 (± 58.36) | 0 |
| Abdominal pain | 2 (0.4%) | 1 (50%) | 280 (± 49.49) | 0 |
| Total | 500 (100%) | 378 (75.6%) | 272.25 (± 114.86) | 11 (2.2%) |
BTT: bowel transit time; CD: Crohn's disease; GVHD: graft-versus-host disease; SBB: small bowel bleeding.
Capsule endoscopy video camera findings in the cases of small bowel bleeding.
| Findings | Small bowel bleeding | ||
|---|---|---|---|
| Overt | Occult | Total | |
| Ulcers | 70 (24.1%) | 11 (31.4%) | 81 (24.8%) |
| Angioectasias | 55 (18.9%) | 5 (14.3%) | 60 (18.4%) |
| Tumors | 32 (11%) | 2 (5.7%) | 34 (10.5%) |
| Erosions | 52 1(7.8%) | 9 (25.7%) | 61 (18.7%) |
| Parasites | 3 (1%) | 0 | 3 (0.9%) |
| Extraintestinal | 21 (7.2%) | 0 | 21 (6.5%) |
| Normal | 58 (19.9%) | 8 (22.9%) | 66 (20.2%) |
Fifty-one video capsules were placed in patients suspected of having CD or as follow-up in those with known disease. Ulcers were observed in 26 (50.9%) of those CEs, whereas the study was normal in the remaining patients. Fourteen video cameras were placed in patients with a history of bone marrow transplantation and suspected gastrointestinal GVHD. Capsule data were consistent with GVHD in 10 of those patients.
Complications presented in 11 patients (2.2%) and capsule retention was the only complication registered. Retention was secondary to tumors in 2 cases (25%) and to stricture in 9 cases (75%). The indication for CE in those patients was SBB in 9 patients (2.7%), known CD in one patient (2.9%), and the search for neoplasia in one patient (1.4%) (fig. 1). The first two cases of retention (tumor and stricture) were resolved through surgery. Of the 9 remaining cases, 7 capsules were retrieved by enteroscopy performed for biopsy sampling and 2 patients had radiologic follow-up until the capsules were expelled through a bowel movement at 3 and 24 months.
Discussion and conclusions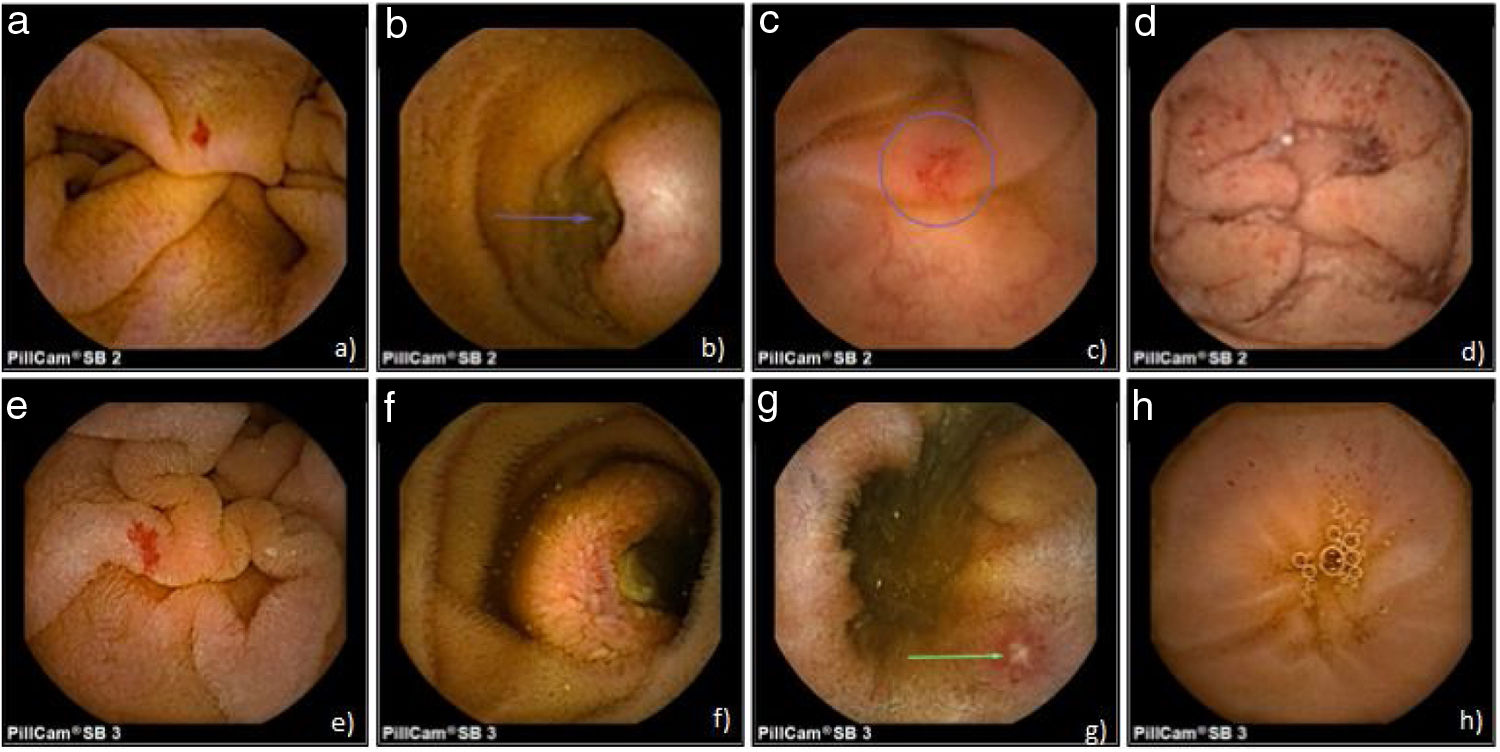
The indications for CE in our study were similar to those reported worldwide. In 2010, Liao et al.9 conducted a meta-analysis that included 22,172 CEs and found that the main indication for the procedure was SBB in 66% of the cases, followed by clinical symptoms in 10.6%, and CD in 10.4%. The most common indication in our study was SBB (65.2%), followed by the search for neoplasia (14.4%), and CD (10.2%). Unlike the study by Liao et al., our second indication was the search for neoplasia, which could be due to the fact that our hospital center has a large population of acromegalic patients that undergo CE to search for neoplasia and small bowel polyps.
In the CEs performed due to overt SBB, there was a finding in 80.1% of the procedures. In 52 patients (17.8%), the findings were lesions identified as P1 erosions, or those with uncertain bleeding potential, according to the Saurin classification.10 P2 lesions, or those with a high potential for bleeding (ulcers, angioectasias, tumors), were found in 62.3% of the CEs, similar to the 61.7% observed by Teshima et al.7 The main finding in SBB was the presence of ulcers, followed by angioectasias. There is controversy in Asia as to whether ulcers,11 tumors,12 or angiodysplasias13 are the most common cause of bleeding, but in the Western world it is agreed that angioectasias are the main cause.14,15 In our case series, the presence of ulcers was superior to that of angioectasias, which could be due to the fact that our study was conducted at a tertiary care hospital center with a large population of patients with nephropathies and rheumatologic diseases that take nonsteroidal anti-inflammatory drugs on a daily basis. CE performed in patients with occult SBB produced findings in 77.1% of the cases. Of those findings, 25.7% were erosions that were P1 lesions. If we take P2 lesions into account, they were present in 51.4% of the cases, which is close to the 53% presented by Pennazio et al.8 in the European gastrointestinal endoscopy guidelines.
In our case series, in the patients with diagnosis or suspicion of CD, no lesions compatible with the disease were observed in 49.1% of the CEs. Nevertheless, the video capsules were useful in helping rule out the disease in the suspected cases and confirming effective treatment in the cases of known CD. The diagnosis of gastrointestinal GVHD is a recent application of CE. Pérez-Cuadrado-Robles et al.6 showed that CE had a diagnostic yield of 54.39%, which was greater than that of conventional endoscopy. In our case series we placed video capsules in 14 patients with GVHD, confirming the diagnosis in 10 of the patients and ruling it out in 4. Comparing those results with the gold standard of histopathologic study, we failed to diagnosis the disease in only one case, in which no data consistent with GVHD were shown by the video camera. Disease diagnosis was made through histopathologic study in that patient. Our diagnostic yield was 92% and diagnosis took less time through CE than through histopathologic study.
CE was performed in 28 patients with chronic diarrhea and positive findings were shown in 22 cases (78.6%). However, the findings were nonspecific due to erosions, angioectasias, or polyps in 10 of the cases. In 12 cases (42.8%), significant lesions were observed: ulcers in 5 cases, data consistent with celiac disease in 5 cases, parasites in one case, and neoplasia in one case. In the patients with ulcers, CD was diagnosed in 3 of them, and no cause of the ulcers was identified in the rest. Diagnosis was confirmed in all the patients with signs of celiac disease. The tumor identified was a lymphoma. Our data were similar to those reported by Song et al.16 in a multicenter study conducted on 91 Korean patients with chronic diarrhea. They identified significant lesions in 42.9% of the patients, nonspecific lesions in 15.4%, and the studies were normal in 41.8%. When compared with our study, the percentage of significant lesions was similar, whereas our percentage of nonspecific lesions was higher.
CE is a safe study. In a meta-analysis that included 25 studies and 5,876 patients, capsule retention was observed in 2.1% (95% CI: 1.5-2.8) of the patients with SBB, 3.6% (95% CI: 1.7-8.6) of the patients with suspected CD, and 8.2% (95% CI: 6.0-11.0) of the patients with an established diagnosis of CD.17 In our study, there were 11 (2.2%) cases of capsule retention, in whom CE was indicated for SBB in 9 of the patients, confirmed CD in one patient, and the search for neoplasia in one patient. Retention was due to stricture in 9 patients and to tumor in 2 patients. The current trend is to keep those patients under surveillance or remove the capsule by enteroscopy, leaving surgery as a last resort if signs of bowel obstruction appear.18 Of the patients in the present study, the first two cases of capsule retention were resolved through surgery, given that one of the patients presented with bowel obstruction and the other underwent surgical resection of the intestinal tumor. In the remaining patients, 7 video capsules were retrieved through enteroscopy, during biopsy sampling. The other 2 patients were followed up until they expelled the video capsules, with no signs of bowel obstruction.
The main limitations of our study were its retrospective design and its performance at a single hospital center.
In conclusion, CE is an efficacious method for the study of small bowel diseases and has a diagnostic yield above 70% in the majority of its indications. In addition, it is a safe procedure, given that it is associated with a low complication rate. Our case series is the largest reported in Mexico, and the use of video capsules was shown to have an efficacy and safety similar to that reported internationally. CE should continue to be performed to increase the knowledge of small bowel pathologies, not only in Mexico, but also worldwide. A multicenter study in Mexico is needed to confirm the data obtained at our hospital center.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Blanco-Velasco G, Mendoza-Segura C, Solórzano-Pineda OM, Hernández-Mondragón OV, Paz-Flores V, Blancas-Valencia JM. Indicaciones, rendimiento diagnóstico y seguridad de la cápsula endoscópica de intestino delgado en pacientes mexicanos. Experiencia de un centro de tercer nivel. Revista de Gastroenterología de México. 2019. https://doi.org/10.1016/j.rgmx.2019.02.008

