



Malignant tumors of the digestive system are a public health problem with epidemiologic variations attributed to factors resulting from the aging of the population and lifestyle changes. Therefore, estimating the future magnitude of the problem is prudent.
AimTo determine the epidemiologic projection up to 2025 of malignant tumors of the digestive system in Veracruz.
Materials and methodsA predictive, analytic, observational study was conducted on patients belonging to the Public health sector of Veracruz that presented with digestive system cancer, within the time frame of 2000-2016, carrying out a disease projection up to 2025. The IBM SPSS 22.0 program was utilized for the statistical analysis, employing simple linear regression. A comparative analysis of the data was carried out and results are shown in scatter graphs.
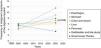
ResultsA total of 2,540 cases were included in the study. Mean patient age was 63.25±13.43, with a predominance of men at 56.65%. The most frequent tumor locations were in the colon and rectum (25.04%), liver (23.66%), and stomach (21.93%). Less frequent sites were the esophagus (4.88%) and small bowel (5.08%). A general 7.63% increase in the disease was predicted for 2025, with increases to 11.51% for esophageal cancer, 7.22% for gastric cancer, 9.09% for colorectal cancer, 5.98% for liver cancer, 7.88% for pancreatic cancer, and 6.46% for cancer of the gallbladder and bile ducts. Only cancer of the small bowel showed a predicted decrease to 3.33%.
Discussion and conclusionsThe results of the present study predict that digestive system cancers in Veracruz will increase importantly by 2025, with colorectal cancer, hepatocellular carcinoma, and gastric cancer as the most frequent tumors, in descending order. The other cancers are estimated to maintain a discrete line of growth. In addition to predicting the behavior of those cancers, the results of the present study are useful for estimating the resources that will be needed for their care by 2025.
Las neoplasias malignas del aparato digestivo representan un problema de salud pública con variaciones epidemiológicas atribuidas a factores resultantes del envejecimiento poblacional y cambios del estilo de vida por lo que es conveniente estimar la magnitud del problema a futuro. Objetivo: Determinar la proyección epidemiológica a 2025 de las neoplasias malignas de aparato digestivo en Veracruz.
Material y métodosEstudio predictivo, analítico, observacional de pacientes con cáncer de aparato digestivo del Sector Salud de Veracruz durante 2000-2016 y su proyección al 2025. Análisis estadístico: Se utilizó el programa IBM SPSS 22.0, regresión lineal simple. Los datos se analizaron de forma comparativa y representados mediante gráficos de dispersión.
ResultadosSe incluyeron 2,540 casos, con promedio de edad 66.93±14.94, predominando el género masculino 56.65%, la localización más frecuente fue colorrectal 25.04%, hígado 23.66% y gástrico 21.93%; siendo los de menor frecuencia esofágico (4.88%) y de intestino delgado 85.07%. Para 2025 se aprecia un incremento de 7.63% en general, el cáncer de esófago de 11.51%, estómago 7.22%, colorrectal 9.09%, hígado 5.98%, páncreas 7.88% y vesícula y vías biliares 6.46%, solamente el cáncer de intestino delgado mostró decremento de 3.32%.
Discusión y conclusionesLas neoplasias del aparato digestivo en Veracruz sufrirán un incremento importante para el 2025 siendo los más frecuentes el colorrectal y el carcinoma hepatocelular con descenso a tercer lugar del gástrico, el resto mantendrá una línea de crecimiento discreta. Los resultados además de predecir su comportamiento son de utilidad para estimar los recursos necesarios para su atención en el 2025.
Malignant neoplasias of the digestive tract are an important health problem worldwide. According to the GLOBOCAN 2012 database, there were 14.1 million new cases of cancer, 8.2 million cancer deaths, and 32.6 million persons living with a malignant neoplasia. Common cancers in more developed regions are breast cancer, prostate cancer, lung cancer, and hepatocellular cancer, followed by gastric cancer, with 462,000 cases and 441,000 deaths reported for hepatocellular cancer and 456,000 cases and 362,000 deaths for gastric cancer. In the less developed regions, they represent 40% of the new cancer cases.1
In Mexico, digestive tract neoplasias have been reported as the first cause of cancer death in persons above 20 years of age and the most affected organs are the colon and rectum, stomach, and liver.2 Villalobos et al. studied 14,325 cases of digestive tract cancer over a 35-year period at 4 healthcare institutions in Mexico City and found a significant decrease in the incidence of gastric cancer at the Hospital General (p<0.013), the Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán” (p<0.012), and the Centro Médico Nacional “20 de Noviembre” of the ISSSTE (p<0.010). They also found a significant increase in colorectal carcinoma, similar to that in the United States and more developed countries.3
The increase in the incidence of digestive tract cancers is attributed to the aging of the population and “modernization” factors, increasingly less healthy lifestyle changes, poor eating habits, a sedentary lifestyle, and obesity, among others, as well as to predisposing disease and genetic factors. The elevated mortality rate in Mexico, compared with others in cancers of greater prevalence, is associated with late diagnoses and poor outcomes, which reflects a deficiency in screening methods.4–7
According to registers of the INEGI in the State of Veracruz, from 2004 to 2015, there were 3,579 cases of digestive tract cancers. In first place was colorectal cancer 1,378 cases, 38.5% of the total), followed by hepatocellular carcinoma (811 cases, 22.66%), gastric cancer (549 cases, 15.33%), pancreatic cancer (429 cases, 11.99%), and others (267 cases, 7.46%).8
In 2012, in the city of Veracruz, a study was conducted on the epidemiologic behavior of digestive tract neoplasias over a 5-year period. There was an increase in the total number of cases per year, and the main sites were the colon (16.86%), stomach (16.76%), and rectum (14.75%), with a predominance in males (52%) over females (48%).9
Knowledge of the current epidemiologic behavior and its projection for the coming years, makes it possible to estimate the magnitude of the problem in the medium term, which is extremely useful for planning disease management and identifying and prioritizing risk factors. The data enable the justification of better prevention measures, focused on creating changes in habits and lifestyles of the population at risk, as well as on screening, so there can be opportune diagnoses and treatments, and consequently, better disease outcome.
AimTo determine the epidemiologic projection for 2025 in malignant digestive tract neoplasias in Veracruz.
Materials and methodsA predictive, analytic, observational study was conducted. A total of 2,540 medical records registered at the Instituto de Investigaciones Médico-Biológicas of the Universidad Veracruzana of patients with a histopathologic diagnosis of a malignant gastrointestinal cancer were reviewed. The patients were seen at the hospitals of the suburban area of Veracruz-Boca del Río that included the Unidad Médica de Alta Especialidad of the Secretaría de Salud, the Hospital de Especialidades del ISSSTE, the Unidad Médica de Alta Especialidad, Centro Médico Nacional “Adolfo Ruiz Cortines” of the IMSS, and the Hospital Naval de Veracruz of the Armada de México. All patients of any age or sex that had a corroborated histologic diagnosis of primary cancer of the digestive tract, within the time frame of 2000-2016, were included in the study.
The statistical analysis was performed using measures of central tendency and dispersion. Absolute and relative frequencies were determined, utilizing the SPSS version 24.0 program. Generalized linear models were used for the bivariate and multivariate analyses, obtaining crude and adjusted prevalence ratios and 95% confidence intervals.
Ethical disclosuresThe present analysis is an observational study and therefore does not require informed consent from the patients, nor does it contain any data identifying them. The study was conducted in accordance with the principles of the Declaration of Helsinki and the protocol was approved by the Bioethics and Research Committee of the Universidad Veracruzana, Región Veracruz-Boca de Río.
ResultsOf the 2,540 cases analyzed, colorectal cancer held first place, with 636 cases 25.04%), followed by hepatocellular carcinoma, with 601 cases (23.66%), and gastric cancer, with 557 cases (21.93%). The less frequent cancers were esophageal cancer, with 124 cases (4.88%), and small bowel cancer, with 129 cases (5.08%). The mean of new cases per year was 149, of which 37 were cases of colorectal cancer, 35 were liver cancer, 33 were gastric cancer, and 20 were cases of pancreatic cancer. The less frequent cancers were those of the bile ducts, esophagus, and small bowel, varying from 7 to 8 cases (Table 1).
Annual frequency of malignant digestive tract neoplasias, 2000-2016, Veracruz n=2,540.
| Year | Esophagus | Stomach | Colon and rectum | Liver | Pancreas | Gallbladder and bile ducts | Small bowel |
|---|---|---|---|---|---|---|---|
| 2000 | 6 (4.84) | 23 (4.13) | 27 (4.25) | 32 (5.32) | 20 (5.79) | 9 (6.08) | 7 (5.42) |
| 2001 | 4 (3.23) | 28 (5.03) | 26 (4.08) | 33 (5.49) | 17 (4.93) | 4 (2.70) | 5 (3.88) |
| 2002 | 4 (3.23) | 37 (6.64) | 32 (5.03) | 43 (7.15) | 19 (5.51) | 12 (8.11) | 9 (6.98) |
| 2003 | 9 (7.26) | 34 (6.10) | 40(6.29) | 27 (4.49) | 18 (5.22) | 8 (5.41) | 11 (8.53) |
| 2004 | 4 (3.23 %) | 34 (6.10) | 32 (5.03) | 34 (5.66) | 15 (4.35) | 10 (6.76) | 8 (6.20) |
| 2005 | 6 (4.84) | 30 (5.39) | 29 (4.56) | 41 (6.82) | 20(5.79) | 9 (6.08) | 10 (7.76) |
| 2006 | 4 (3.23) | 42 (7.54) | 34 (5.35) | 37 (6.16) | 17(4.93) | 6 (4.05) | 11 (8.52) |
| 2007 | 6 (4.84) | 30 (5.39) | 40 (6.29) | 44 (7.32) | 21(6.09) | 12 (8.11) | 9 (6.98) |
| 2008 | 6 (4.84) | 32 (5.75) | 32 (5.03) | 31 (5.15) | 23 (6.67) | 9 (6.09) | 8 (6.20) |
| 2009 | 7 (5.65) | 28 (5.03) | 39 (6.13) | 34 (5.66) | 19 (5.51) | 6 (4.06) | 8 (6.20) |
| 2010 | 10 (8.06) | 26 (4.67) | 34 (5.35) | 36 (5.99) | 24 (6.96) | 9 (6.08) | 9 (6.20) |
| 2011 | 5 (4.03) | 27 (4.85) | 47 (7.39) | 32 (5.32) | 20 (5.79) | 7 (4.73) | 7 (5.43) |
| 2012 | 11 (8.87) | 38 (6.82) | 42 (6.60) | 35 (5.82) | 18 (5.22) | 13 (8.78) | 5 (3.88) |
| 2013 | 9 (7.26) | 36 (6.46) | 40 (6.29) | 36 (5.99) | 19 (5.51) | 9 (6.08) | 4 (3.10) |
| 2014 | 11 (8.87) | 35 (6.28) | 44 (6.92) | 33 (5.49) | 26 (7.54) | 7 (4.73) | 5 (3.88) |
| 2015 | 13 (10.48) | 38 (6.82) | 48 (7.55) | 35 (5.82) | 24 (6.96) | 8 (5.40) | 7 (5.43) |
| 2016 | 9 (7.26) | 39 (7.001) | 50 (7.86) | 38 (6.32) | 25 (7.25) | 10 (6.76) | 6 (4.65) |
| 2025 | (11.51) | (7.22) | (9.095) | (5.98) | (7.88) | (6.45) | (4.65) |
| Subtotal | 124 | 557 | 636 | 601 | 345 | 148 | 129 |
| Percentage (%) | 4.88 | 21.93 | 25.04 | 23.66 | 13.58 | 5.83 | 5.08 |
Males predominated over females in the present case series, with 1,439 men 56.65% and 1,101 women 43.35%). In esophageal cancer, the majority of cases were in men (n=103) (83.10%), with 21 cases in women (16.90%). Females predominated in the cases of gallbladder and bile duct cancer (n=123) (83.10%), with 25 cases in males (16.90%) (Table 2).
Distribution by sex of the malignant digestive tract neoplasias, 2000-2016, Veracruz n=2,540.
| Location | Total | Male | Female | Male (%) | Female (%) |
|---|---|---|---|---|---|
| Pancreas | 345 | 213 | 132 | 61.8 | 38.2 |
| Stomach | 557 | 324 | 233 | 58.2 | 41.8 |
| Esophagus | 124 | 103 | 21 | 83.1 | 16.9 |
| Liver | 601 | 341 | 260 | 56.8 | 43.2 |
| Colon and rectum | 636 | 347 | 289 | 54.6 | 45.4 |
| Small bowel | 129 | 86 | 43 | 66.7 | 33.3 |
| Gallbladder and bile ducts | 148 | 25 | 123 | 16.9 | 83.1 |
| Total | 2,540 | 1,439 | 1,101 | 56.65 | 43.35 |
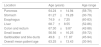
The overall mean patient age was 63.25±13.43 years (range 30-94). The oldest group corresponded to the patients with esophageal cancer, with a mean age of 74.9±7.25 years (range 60-83), followed by patients with hepatocellular carcinoma, with a mean age of 68.7±8.55 years (range 52-86), and patients with colorectal cancer, with a mean age of 67.30±9.87 years (range 42-88). The mean age of patients with pancreatic cancer was 64.24±14.94 years (range 58-79) and for patients with gastric cancer it was 61.27±19.28 years (range 30-79). They were under the overall mean patient age and in fourth place, followed by patients with small bowel cancer, with a mean age of 56.56±16.25 years (range 59-72), and patients with bile duct cancer, with a mean age of 49.8±17. 87 years (range 45-94) (Table 3).
Distribution by age of the malignant digestive tract neoplasias, 2000-20016, Veracruz n=2,540.
| Location | Age (years) | Age range |
|---|---|---|
| Pancreas | 64.24±14.94 | (58-79) |
| Stomach | 61.27±19.28 | (30-79) |
| Esophagus | 74.9±7.25 | (60-83) |
| Liver | 68.7±8.55 | (52-86) |
| Colon and rectum | 67.30±9.87 | (42-88) |
| Small bowel | 56.56±16.25 | (59-72) |
| Gallbladder and bile ducts | 49.8±17. 87 | (45-94) |
| Overall mean patient age | 63.25±13.43 | (30-94) |
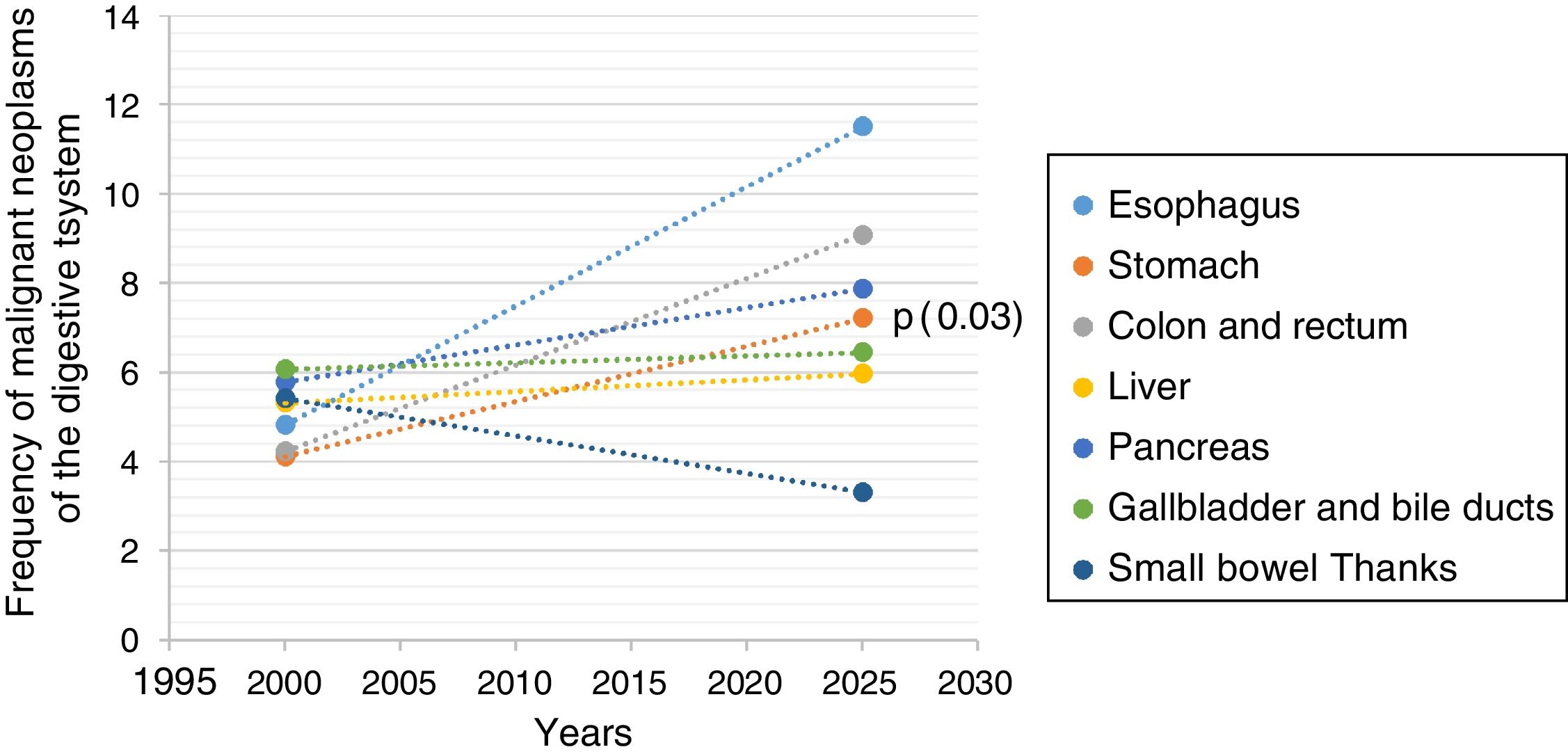
Utilizing the information from the database, the prediction for the year 2025 was calculated. A general increase in the majority of the neoplasias was shown. Esophageal cancer was in first place, with a statistically significant increase from 4.84 to 11.51% (6.67%) (p=0.001), followed by colorectal cancer from 4.24 to 9.09% (4.85%) (p=0.001). The calculation showed an increase in gastric cancer from 4.13 to 7.22% (3.09%) (p=0.036) and in pancreatic cancer from 5.8 to 7.88% (2.08%) (p=0.006). Hepatocellular carcinoma showed an increase from 4.01 to 5.98% (1.98%) (p=0.854) and bile duct cancer from 6.0 to 6.46% (1.98%), with no statistically significant difference. There was a decrease in small bowel cancer from 5.43 to 3.33% (2.11%) (p=0.016) (Table 4, Figure 1).
Predictions of malignant digestive tract neoplasias for the year 2025, Veracruz n=2,540.
| Location | r | R² | % | p | Prediction (%) |
|---|---|---|---|---|---|
| Esophagus | 0.721 | 0.519841 | 51.9841 | 0.001 | 11.5125 |
| Stomach | 0.394 | 0.155236 | 15.5236 | 0.038 | 7.22 |
| Colon and rectum | 0.844 | 0.712336 | 71.2336 | 0. 001 | 9.095 |
| Liver | 0.034 | 0.001156 | 0.1156 | 0.854 | 5.9781 |
| Pancreas | 0.635 | 0.403225 | 40.3225 | 0.006 | 7.8825 |
| Gallbladder and bile ducts | 0.09 | 0.0081 | 15.21 | 0.621 | 6.456 |
| Small bowel | −0.461 | 0.2121 | 21.21 | 0.016 | - 3.3275 |
Different factors have influenced the epidemiologic behavior of malignant neoplasias in different regions across the globe, such as ethnic characteristics, economic, technologic, and cultural development, healthcare infrastructure, and the aging of the population. In the coming years, the numbers of cases of cancer in general are estimated to increase, whereas some are expected to decrease,1,4,5 making it of interest to evaluate the panorama of the digestive tract neoplasias in a projection for the year 2025 in the population of the city of Veracruz.
According to reports from the GLOBOCAN database and the WHO, colorectal cancer holds third place in men (746,000 cases, 10% of the total) and second place in women (614,000 cases, 9.2% of the total). Frequency is higher in more developed regions, but the mortality rate is greater in developing countries. The related risk factors are hereditary polyposis disease, inflammatory bowel disease, obesity, processed food consumption, and smoking.1 According to statistical data published by the American Cancer Society, colorectal cancer was in first place, but risk was lower in the Hispanic or Latin population than in non-Hispanic whites.4,10 The same behavior has been observed in Mexico.11,12 In the present study, colorectal cancer has been in first place since 2003, with a projection for 2025 of an increase to 9.09%, a mean patient age at disease presentation of 67.30±9.87 years, and greater frequency in males (54.8/45.4%).
Gastric cancer is in fifth place worldwide in malignant neoplasias and second place in digestive tract neoplasias, with nearly one million new cases, a predominance in males, and a tendency to decrease in developed countries.1 In 2017 in the United States, 27,510 new cases were diagnosed (62.67% in men and 37.33% in women). There was a tendency to present with greater frequency and at earlier stages in life in the Hispanic population.4 In Mexico, Sánchez-Barriga et al., as well as other authors, have corroborated a significant decrease in gastric cancer at the metropolitan area hospitals.13–15 However, in our study, we observed an increase to 7.22% for the year 2025, with a mean patient age of 61.27±19.28 years, and predominance in males (58.2/41.8%), most likely associated with a high incidence of Helicobacter pylori, the type of eating habits, and the low cultural level of the population.
One of the neoplasias whose frequency has increased in recent decades is hepatocellular carcinoma, now in fifth place in men and the second cause of cancer death worldwide. In national reports, it is in third place, and in our study, it is in second place, with a mean patient age of 68.7±8.55 years, predominance in males (56.8/43.2%), and a projected increase to 5.98% for 2025. We believe its elevated frequency is the result of a greater number of cases with chronic liver diseases due to viral infections and the rising number of cases of fatty liver disease.1,16–18
Pancreatic cancer is estimated to be responsible for 331,000 deaths annually, with a 4% mortality rate. It holds sixth place, with greater frequency in developed countries, and is the seventh cause of cancer death in both sexes, worldwide. It has been on the rise in recent decades,19 with variations in different regions across the globe. Pancreatic cancer is related to alcohol consumption, smoking, obesity, chronic pancreatitis, and diabetes mellitus in genetically predisposed subjects. It is considered one of the most lethal neoplasias, given that its incidence is similar to its mortality rate and there is only a 5% 5-year survival rate.20,21 In Mexico, the disease holds fifth place in men and seventh place in women. In our study, it held fourth place, with a mean patient age of 64.24±14.94, a predominance in males over females (61.8/38.2%), and a tendency to increase to 7.88% for 2025.
Esophageal cancer is in eighth place worldwide, with 456,000 cases reported annually and a frequency of 7.5%. Close to 80% of the cases present in less developed regions, such as Africa and Asia, with a 3:1 predominance in males and a very low survival rate.1 Factors identified for squamous cell disease are the consumption of carcinogens, smoking, alcohol consumption, lesions produced by the ingestion of caustic substances, and achalasia. The main factor in adenocarcinoma of the distal third of the esophagus is Barrett’s esophagus.22 In Mexico, esophageal cancer holds one of the last places of digestive tract neoplasias. In our study, it was in seventh place, with a mean patient age of 74.9±7.25 years, the oldest age in the entire case series, a predominance in males (83.1/16.9%), and a projected increase to 11.51% for 2025, with the majority of cases located in the cardioesophageal junction.
In national and international publications, as well as in the present study, gallbladder and bile duct cancer holds sixth place, with greater frequency in females (83.1/16.9%), a mean patient age of 49.8±17.87 years, and a slight but not significant increase for 2025 to 6.46%. That type of neoplasia is related to gallstone disease, alcohol consumption, smoking, and cholestasis, and its low frequency is related to early cholecystectomy and the current resources for managing bile duct obstruction.23,24
In our study, small bowel cancer was the only cancer with a negative prediction and the lowest frequency. That concurs with reports from the GLOBOCAN database, in which it accounts for only 5% of cancers and has a higher rate in patients over 60 years of age. The mean age in our patients was lower, at 56.56±16.25 years, with a predominance in males (66.7/33.3%), and a decrease to 3.33% for the year 2025.25
In conclusion, digestive tract neoplasias in Veracruz, as well as in the rest of the world, will have increased by the year 2025. In our study, the types that presented with greater frequency were colorectal cancer, followed by hepatocellular carcinoma and gastric cancer, all with a projected increase for 2025. Pancreatic cancer and gallbladder and bile duct cancer had a lower incidence, in fourth and fifth place, with a slight increase that was not statistically significant. Small bowel cancer was the least frequent, with a tendency to decrease in the coming years, similar to that reported in studies worldwide.
We believe that knowledge of the modifications in the epidemiologic panorama of digestive tract neoplasias is of great use for planning the medium-term and long-term use of health sector resources, which should essentially be directed toward the opportune detection of those cancers in at-risk populations.
Financial disclosureNo financial support was received in relation to the present study.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Roesch-Dietlen F, Ortuño-García KJ, González-Santés M, Grube-Pagola P, Remes-Troche JM, Díaz-Roesch F, et al. Cáncer del aparato digestivo en Veracruz. La magnitud del problema al año 2025. Revista de Gastroenterología de México. 2020;85:145–150.

