





Clinical practice guidelines on the diagnosis and treatment of acute pancreatitis (CPGDTAP) have been designed in an effort to reduce the morbidity and mortality of that severe disease.
AimTo identify the knowledge acquired from CPGDTAP in hospitals in Veracruz.
Materials and methodsA descriptive, observational, multicenter study was conducted at four hospitals in Veracruz, through the application of a survey to evaluate the knowledge of attending physicians and residents that treat patients with acute pancreatitis. Descriptive statistics were employed to analyze the results.
ResultsA total of 74 physicians were surveyed, 55.41% of whom were attending physicians and 44.59% of whom were resident physicians. The majority of physicians (67.57%) were familiar with CPGDTAP from the Asociación Mexicana de Gastroenterología (AMG), followed by those of the General Health Council of the Mexican Department of Health (CENETEC, the Spanish acronym) (54.05%) and the American College of Gastroenterology (ACG) (48.65%). A total of 97.30% of the physicians routinely use a nasogastric tube, 79.73% considered early enteral nutrition to be very important, as did 98.65% regarding generous fluid replacement, 85.14% did not routinely use antimicrobials, 63.51% ordered a CAT scan at 72 h or later, and 87.84% answered that infected necrosis was the indication for surgery, preferably after the third week.
Discussion and conclusionsIn our hospital environment, the CPGDTAP issued by the AMG and CENETEC were the most well-known, but their recommended measures were given importance by under 85% of the physicians surveyed. Therefore, the diffusion of the knowledge they contain is advisable to guarantee optimal results in acute pancreatitis management.
Las Guías de Práctica Clínica para el Diagnóstico y Tratamiento de la Pancreatitis Aguda (GPCDMPA) han sido diseñadas con la finalidad de disminuir la morbimortalidad de ésta grave enfermedad.
ObjetivoIdentificar el conocimiento de las GPCDMPA en hospitales de Veracruz.
Material y métodosEstudio observacional, descriptivo, multicéntrico realizado en 4 hospitales de Veracruz, aplicando encuesta para evaluar su conocimiento en médicos y residentes que atienden pacientes con pancreatitis aguda. El análisis de los resultados se realizó por estadística descriptiva.
ResultadosSe aplicaron 74 encuestas: 55.4% a médicos adscritos y 44.59% a residentes. La GPCDTPA más conocida fue la de la Asociación Mexicana de Gastroenterología (AMG) (67.57%), seguida por la del Consejo de Salubridad General de la Secretaría de Salud (CENETEC) (54.05%) y la del Colegio Americano de Gastroenterología (ACG) (48.65%). El 97.30% de los médicos utilizaron rutinariamente una sonda nasogástrica, el 79.73% consideran muy importante el inicio temprano de la nutrición enteral, el 98.65% la reposición hídrica generosa, el 85.14% no emplearon antimicrobianos de rutina, el 63.51% realizan la TAC a partir de las 72 h y el 87.84% consideran que la indicación quirúrgica es la necrosis infectada, preferentemente después de la tercera semana.
Discusión y conclusionesEn nuestro medio las (GPCDMPA) más conocidas fueron las de la AMG y CENETEC y su conocimiento es inferior al 85.00%, por lo que es recomendable su difusión para garantizar resultados óptimos en el manejo de la pancreatitis aguda.
Acute pancreatitis is the most urgent of pancreatic diseases and it preferentially affects reproductive-age subjects. Its etiology is multifactorial, and the most frequent cause is gallstones (45%), followed by chronic alcohol consumption (32-35%). Trauma, hypercalcemia, hypertriglyceridemia, and anatomic alterations (2-8%) are less common causes and around 10% of cases are idiopathic. The majority of cases are mild or moderate, with a general mortality rate of 2 to 9%. Nevertheless, 15 to 20% of cases can be severe, in which the mortality rate increases to 39 to 42%. Incidence worldwide is from 4.8 to 24.0 per 100,000 inhabitants and accounts for more than 220,000 annual hospital admissions in the United States.1–5 The estimated prevalence in Mexico of 2 to 3% places it as the seventeenth cause of death, with a mortality rate of 0.5 × 100,000 inhabitants.6
The Institute of Medicine (IOM) first published the clinical practice guidelines for management and treatment,7–8 and over time, they were modified to include scientific and technologic advances to optimize the care of different severe diseases and reduce morbidity and mortality.9
Over the past two decades, different national10–12 and international13–19 Clinical Practice Guidelines for the Diagnosis and Treatment of Acute Pancreatitis (CPGDTAP) have been published, and even though there are reports from different countries on the degree of knowledge acquired from them and their application,20–28 such studies are scarce in Mexico.29,30 Therefore, we decided to conduct the present study in our hospital environment to find out the importance the clinical practice guidelines have in the main hospitals of the public health sector in Veracruz.
AimTo identify the degree of knowledge of the CPGDTAP held by attending physicians and residents at hospitals in Veracruz.
Materials and methodsA descriptive, observational, and multicenter study was conducted.
Study universeThe study was conducted on attending physicians and residents from the services of the emergency department, hospitalization, and intensive care units of four hospitals belonging to the Public Health Sector of the Port of Veracruz: the Hospital Regional de Especialidades (HRV) of the Health Department, the Hospital General de Zona No. 71 (IMSS), the Hospital de Especialidades del Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE), and the Hospital Naval de Especialidades de Veracruz (HNAVER) of the Department of the Navy.
Inclusion criteriaPhysicians with a specialty in internal medicine, general surgery, gastroenterology, and emergency medicine and residents specializing in internal medicine and general surgery. There were no distinctions in relation to age or sex.
Exclusion criteriaPhysicians and residents that answered the questionnaires incompletely.
ProcedureA direct response questionnaire was applied to evaluate the following variables: age, sex, specialty, years of professional medical practice, national and international guidelines known and utilized (from the Asociación Mexicana de Gastroenterología [AMG], the Centro Nacional de Excelencia Tecnológica [CENETEC] of the General Health Council of the Mexican Department of Health, the Asociación Mexicana de Cirugía General [AMCG], the American College of Gastroenterology [ACG], the American Gastroenterological Association [AGA], from Japan [Japanese guidelines], the United Kingdom [British], and the Sociedad Española de Patología Digestiva [Spanish]). The questionnaire also determined the importance of employing the following management conducts: fasting, early feeding, nasogastric tube use, routine antimicrobial use, generous fluid replacement, when to carry out a computed axial tomography (CAT) scan, and when to perform surgery. The answers were classified in three grades: a) very important, b) important, and c) not very important.
The questionnaire was formulated at the Gastroenterology Department of the Instituto de Investigaciones Médico-Biológicas of the Universidad Veracruzana, taking into account the main concepts issued by the consensus on the CPGDTAP conducted by the AMG, and applied by medical students, in their final year of study, doing their social service at each participating hospital center, after undergoing training in questionnaire application to prevent answer bias.
Sample sizeFifty percent of the 148 staff physicians and residents that treated patients with acute pancreatitis at the four participating hospitals (74 questionnaires) were surveyed.
Statistical analysisDescriptive statistics were performed through measures of central tendency and dispersion and standard deviation, utilizing the IBM SPSS version 22 program.
Ethical considerationsThe present article follows the current regulations in bioethical research and the protocol was approved by the Bioethics and Research Committee of the School of Medicine of the Universidad Veracruzana, Región Veracruz-Boca del Rio. The authors declare there was no need for statements of informed consent because the questionnaires were anonymous.
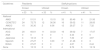
ResultsAmong the four hospital centers, a total of 74 questionnaires were applied: 24 at the HRV (32.43%), 30 at the IMSS (40.54%), 13 at the ISSSTE (17.57%) and 7 at the HNAVER (9.46%). Forty-one (55.41%) of the questionnaires corresponded to staff physicians and 33 (44.59%) to residents. Regarding specialties, 28 corresponded to the service of internal medicine (37.84%), 26 to general surgery (35.14%), 13 to emergency medicine (17.57%), and 7 to gastroenterology (9.46%). The mean age of the residents was 28.61 + 7.18, with a range of 25 to 36 years, and of the staff physicians was 51.12 + 11.27, with a range of 34 to 77 years. The predominant sex was male, with 51 physicians (70.27%), and 23 of the physicians were female (29.73%) (Table 1).
The number of questionnaires answered by the residents and staff physicians, according to specialty, hospital, sex, and age.
| Residents | Staff physicians | |||
|---|---|---|---|---|
| n | % | n | % | |
| Specialty | ||||
| Internal medicine | 16 | 48.48 | 12 | 29.27 |
| Surgery | 10 | 30.30 | 16 | 39.02 |
| Emergency medicine | 7 | 21.22 | 3 | 7.32 |
| Gastroenterology | - | - | 10 | 24.39 |
| Total | 33 | 41 | ||
| Specialty grade | ||||
| R1 | 12 | 36.3 | ||
| R2 | 12 | 36.3 | ||
| R3 | 5 | 15.1 | ||
| R4 | 4 | 12.1 | ||
| Hospital | ||||
| HRV | 11 | 33.34 | 13 | 31.71 |
| ISSSTE | 7 | 21.21 | 6 | 14.63 |
| IMSS | 10 | 30.30 | 20 | 48.78 |
| HNAVER | 5 | 15.15 | 2 | 4.88 |
| Total | 33 | 41 | ||
| Sex | ||||
| Male | 20 | 60.61 | 31 | 75.61 |
| Female | 13 | 39.39 | 10 | 24.39 |
| Mean age, range (years) | 28.61 + 7.18 (25-36) | 51.12 + 11.27 (34-77) | ||
The most well-known national CPGDTAP, for the two groups, were the guidelines of the AMG (50; 67.57%), the CENETEC (40; 54.05%), and the AMCG (22; 29.73%). Nine (12.16%) of the physicians were not familiar with any of them. The most well-known guidelines in the staff physician group were those of the AMG (33; 80.49%), in second place those of the CENETEC (16; 39.02%), and in third place those of the AMCG (12; 29.27%), whereas in the resident group the most well-known were the guidelines of the CENETEC (24; 72.71%), followed by the AMG (17; 51.50%), and the AMCG (10; 30.3%).
The most well-known international guidelines were those of the ACG (36; 48.65%), followed by the Spanish guidelines (26; 35.13%), the British guidelines (11; 14.86%), the Japanese guidelines (7; 9.46%), and those of the AGA (1; 1.35%). Nine (12.16%) of the physicians were not familiar with any of the guidelines and 15 (20.27%) were familiar with more than one.
The national CPGDTAP most utilized by the two groups were those of the AMG (14; 18.92%), CENETEC (23; 31.08%), and AMCG (5; 6.76%). Eleven staff physicians utilized the guidelines of the CENETEC (26.83%), 9 utilized those of the AMG (21.95%), and 3 those of the AMCG (7.32%). Twelve residents utilized the guidelines of the CENETEC (36.36%), 5 those of the AMG (15.15%), and 2 those of the AMCG (6.06%). The international guidelines used by the staff physicians were those of the ACG (7; 17.07%), followed by the Japanese guidelines (2; 4.87%), and the British guidelines (1; 2.44%), whereas 11 residents utilized the guidelines of the ACG (33.33%) and one resident used the Spanish guidelines (3.03%) (Table 2).
Knowledge and use of the national and international CPGDTAP by the residents and staff physicians surveyed.
| Guidelines | Residents | Staff physicians | ||||||
|---|---|---|---|---|---|---|---|---|
| Known | Utilized | Known | Utilized | |||||
| n 33 | % | n 33 | % | n 41 | % | n 41 | % | |
| National | ||||||||
| AMG | 17 | 51.51 | 5 | 15.15 | 33 | 80.49 | 9 | 21.95 |
| CENETEC | 24 | 72.73 | 12 | 36.36 | 16 | 39.02 | 11 | 26.83 |
| AMCG | 10 | 30.30 | 2 | 6.06 | 12 | 29.27 | 3 | 7.32 |
| International | ||||||||
| ACG | 20 | 60.61 | 11 | 33.33 | 16 | 39.02 | 7 | 17.07 |
| AGA | 0 | 0 | 0 | 0 | 1 | 2.44 | 0 | 0 |
| Japanese | 4 | 12.12 | 0 | 0 | 3 | 7.32 | 2 | 4.87 |
| Spanish | 9 | 27.27 | 1 | 3.03 | 17 | 41.46 | 0 | 0 |
| British | 9 | 27.27 | 0 | 0 | 2 | 4.87 | 1 | 2.44 |
| None | 5 | 15.15 | 0 | 0 | 4 | 9.76 | 5 | 12.19 |
The analysis of the answers to the items about the diagnosis and treatment of acute pancreatitis produced the following results:
- •
Routine use of the nasogastric tube. Twelve (16.22%) physicians considered it very important, 60 (81.08%) important, and 2 (2.70%) not very important. The answers were proportionally similar between the staff physicians and residents.
- •
Early enteral nutrition use. Fifty-nine (79.73%) physicians considered it very important, 13 (17.57%) important, and 2 (2.70%) not very important. The staff physicians gave that measure more importance than the residents did (82.93% versus 75.76%).
- •
Generous fluid replacement. Seventy-three (98.65%) of the physicians considered vigorous hydration at the beginning of management very important and none of the physicians (0%) considered it not very important. The answers were similar between the two groups (Table 3).
Table 3.The importance of using a nasogastric tube, early enteral nutrition, and generous fluid resuscitation, according to the physicians surveyed.
Parameter Residents Staff physicians Total n 33 % n 41 % n 74 % Routine nasogastric tube use Very important 7 21.21 5 12.20 12 16.22 Important 25 75.76 35 85.37 60 81.08 Not very important 1 3.03 1 2.43 2 2.70 Early enteral nutrition Very important 25 75.76 34 82.93 59 79.73 Important 7 21.21 6 14.64 13 17.57 Not very important 1 3.03 1 2.43 2 2.70 Generous fluid replacement Very important 32 96.97 41 100.00 73 98.65 Important 1 3.03 0 0 1 1.35 Not very important 0 0 0 0 0 0 - •
Routine antimicrobial use. Sixty-three (85.14%) physicians answered that antimicrobials should not be routinely used and 11 (14.86%) answered that they used them routinely, with similar percentages between the two groups (84.85/85.37%).
- •
When to perform surgery. Sixty-five (87.84%) of the physicians answered that surgery should be performed after the third week, 6 (8.11%) between the second and third week, and 3 (4.05%) in the first week. A total of 95.12% of the staff physicians recommended the later performance of surgery, compared with 78.79% of the residents, which we consider was due to the experience of the attending physicians.
- •
When to carry out a CAT scan: Forty-seven (63.51%) physicians responded that a CAT scan should be carried out from the third day and 27 (36.49%) upon hospital admission of the patient. There was a big difference between the two groups, given that 57.58% of the residents and 68.29% of the staff physicians considered it should be performed from the third day and 42.43% of the residents and 31.71% of the staff physicians recommended its early performance. Table 4 describes the results in more detail.
Table 4.The routine use of antimicrobials, when to perform surgery, and when to carry out a CAT scan, according to the physicians surveyed.
Parameter Residents Staff physicians Total n 33 % n 41 % n 74 % Antimicrobial use Routinely used 5 15.15 6 14.63 11 14.86 Not used 28 84.85 35 85.37 63 85.14 When to perform surgery 1st week 3 9.09 0 0 3 4.05 2nd – 3rd week 4 12.12 2 4.88 6 8.11 After the 3rd week 26 78.79 39 95.12 65 87.84 When to opportunely carry out a CAT scan Upon hospital admission 14 42.43 13 31.71 27 36.49 On the 3rd day 14 42.43 17 41.47 31 41.89 After the 4th day 5 15.14 11 26.83 16 21.62 CAT: computed axial tomography with endovenous contrast medium.
The CPGDTAP first introduced two decades ago have become a valuable resource for the medical personnel and hospital centers that treat acute pancreatitis because they provide a methodological management option based on the best evidence, whose main goal is to reduce the morbidity and mortality of the disease.4,5,9 Different medical associations worldwide have formulated their own guidelines and recommendations.13–18 In Mexico, the guidelines from the AMG, the AMCG and the Mexican Norm issued by the General Health Council of the Department of Health10–12 have been published, and they should be widely distributed for the knowledge they contain and the application of said knowledge.
The best manner to evaluate the use of that knowledge is by determining modifications in the morbidity and mortality rates, but there is considerable interhospital variability, along with factors, such as the level of knowledge of the personnel and physical, technologic, and economic resources, making such an evaluation difficult to carry out. The other procedure for evaluating guideline knowledge is through surveys that explore the clinical experience of the personnel directly involved in patient management, through the statements and recommendations of experts. The main disadvantage of that type of intervention is the lack of objectivity, but in general, it allows a situational diagnosis to be made.
Our study showed that the mean age was 28.61 years + 7.18 for the residents and 51.12 years + 11.27 for the attending physicians, which was logical, given the generational difference between the two groups. Males (68.92%) predominated over females (31.08%) (Table 1).
The results of our survey showed that 87.84% of the attending physicians and residents were familiar with at least one of the CPGDTAP, whereas 12.16% were not. The Mexican guidelines were the most well-known, with those of the AMG (67.57%) in first place, followed by those of the CENETEC (54.05%), with almost equal frequency for the ACG (48.65%). The attending physicians were more familiar with the AMG guidelines, whereas the residents were more familiar with those of the CENETEC and the AMCG. The two groups were not very familiar with the international guidelines.
Regarding the use of the guidelines, there was no clear inclination by either the attending physicians or the residents towards any of them, and the preference for the national and international guidelines was similar: the CENETEC (31.08%), the AMG (18.92%) and the ACG (24.32%). The residents preferred the guidelines of the CENETEC and the ACG, whereas the attending physicians preferred those of the CENETEC and the AMG (Table 2).
Upon evaluating the importance of certain specific treatment measures, the answers were satisfactory overall, in 82.43% of the physicians. They were higher in the attending physicians (90.94%) than in the residents (76.19%). Importance was given to the routine use of a nasogastric tube (97.30%), generous fluid resuscitation (98.65%), the non-routine use of antimicrobials (85.14%), the performance of surgery after 3 weeks of symptom onset (87.84%), early enteral nutrition (79.73%), and the indication for when to carry out a CAT scan (Tables 3 and 4).
We only evaluated the aspect of knowledge in our study, which was a disadvantage and a methodological limitation.
ConclusionsOur study results showed that 87.84% of the physicians and residents that work in hospital centers are familiar with at least one of the CPGDTAP. The most well-known among the staff physicians were the AMG guidelines, whereas the residents were more familiar with those of the CENETEC.
Only 82.43% of the physicians surveyed gave importance to the measures recommended in the guidelines, thus we consider their distribution and promotion in the institutions of the public health sector to be of great importance, for ensuring the best healthcare to patients with acute pancreatitis.
Conflict of interestJosé María Remes Troche is an advisor and speaker for the Takeda and Azofarma laboratories. The rest of the authors declare they have no conflict of interest.
Financial disclosureThe present study was carried out utilizing funds from the Instituto de Investigaciones Médico-Biológicas of the Universidad Veracruzana.
Please cite this article as: Roesch-Dietlen FB, Salgado-Vergara L, Sánchez-Maza YJ, Durán-Álvarez DI, Díaz-Roesch F, Remes-Troche JM, et al. Conocimiento de las Guías Clínicas de Diagnóstico y Tratamiento de la Pancreatitis Aguda en médicos adscritos y residentes de los hospitales de Veracruz. Revista de Gastroenterología de México. 2021;86:133–139.

