

















Mantle cell lymphoma is an aggressive subtype of B-cell non-Hodgkin lymphoma and its incidence is 0.5/100,000 inhabitants. Gastrointestinal involvement at diagnosis is 15-30%. The aim of our study was to analyze the clinical and endoscopic characteristics of mantle cell lymphoma affecting the digestive tract.
Material and methodsA retrospective study was conducted, based on a case series of patients with mantle cell lymphoma affecting the gastrointestinal tract that were diagnosed over a 10-year period.
ResultsTen patients (11.7%) had gastrointestinal tract involvement. The upper endoscopic findings were polypoid lesions (66%), thickened folds (44%), and nonspecific changes in the mucosa (33%). At colonoscopy, polypoid lesions were viewed in 100% of the patients and ulcerated lesions in 40%.
ConclusionPolypoid lesions are the most common endoscopic characteristics in patients with mantle cell lymphoma of the gastrointestinal tract. Upper endoscopy and colonoscopy should be carried out on patients with mantle cell lymphoma, even those with nonspecific symptoms, to check their gastrointestinal status. Gastrointestinal involvement has an impact on disease staging.
El linfoma de células del manto es un subtipo agresivo de linfoma no Hodgkin de fenotipo B, con una incidencia de 0.5/100,000 habitantes. La afectación gastrointestinal al momento del diagnóstico es del 15-30%. El objetivo del estudio fue analizar las características clínicas y endoscópicas del linfoma del manto que afecta al tubo digestivo.
Material y métodosSe realizó un estudio retrospectivo, con base en una serie de casos de pacientes con diagnóstico de linfoma del manto con afección del tracto gastrointestinal en un período de 10 años.
ResultadosDiez pacientes (11.7%) tuvieron afección del tracto gastrointestinal. Los hallazgos endoscópicos en la endoscopia alta fueron: lesiones polipoides (66%), pliegues engrosados (44%) y cambios inespecíficos de la mucosa (33%). En la colonoscopia se observaron lesiones polipoides en el 100% de los pacientes y lesiones ulceradas en el 40% de estos.
ConclusiónLas lesiones polipoides son las características endoscópicas más comunes en pacientes con linfoma de células del manto del tracto gastrointestinal. El estado gastrointestinal de los pacientes con linfoma de células del manto debe investigarse incluso con síntomas inespecíficos, incluyendo endoscopia superior y colonoscopia. La afectación gastrointestinal tiene un impacto en la estadificación de la enfermedad.
Mantle cell lymphoma is an aggressive subtype of B-cell non-Hodgkin lymphoma and accounts for 3 to 6% of non-Hodgkin lymphoma, with an annual incidence of 0.5 per 100,000 inhabitants.
Four histologic variants are described: small-cell, mantle zone, diffuse, and blastoid. The pathology predominates in men and the mean presentation age is 60 years. It is more frequently diagnosed at advanced disease stages, with bone marrow and peripheral blood involvement, as well as generalized lymphadenopathy in 75% of the cases. Some patients also present with splenomegaly, hepatomegaly, and extranodal disease, such as lymphomatous polyposis of the colon. Mantle cell lymphoma is very aggressive and has a poor treatment response. The frequency of gastrointestinal involvement at diagnosis is 15 to 30% and many patients are asymptomatic.1,2
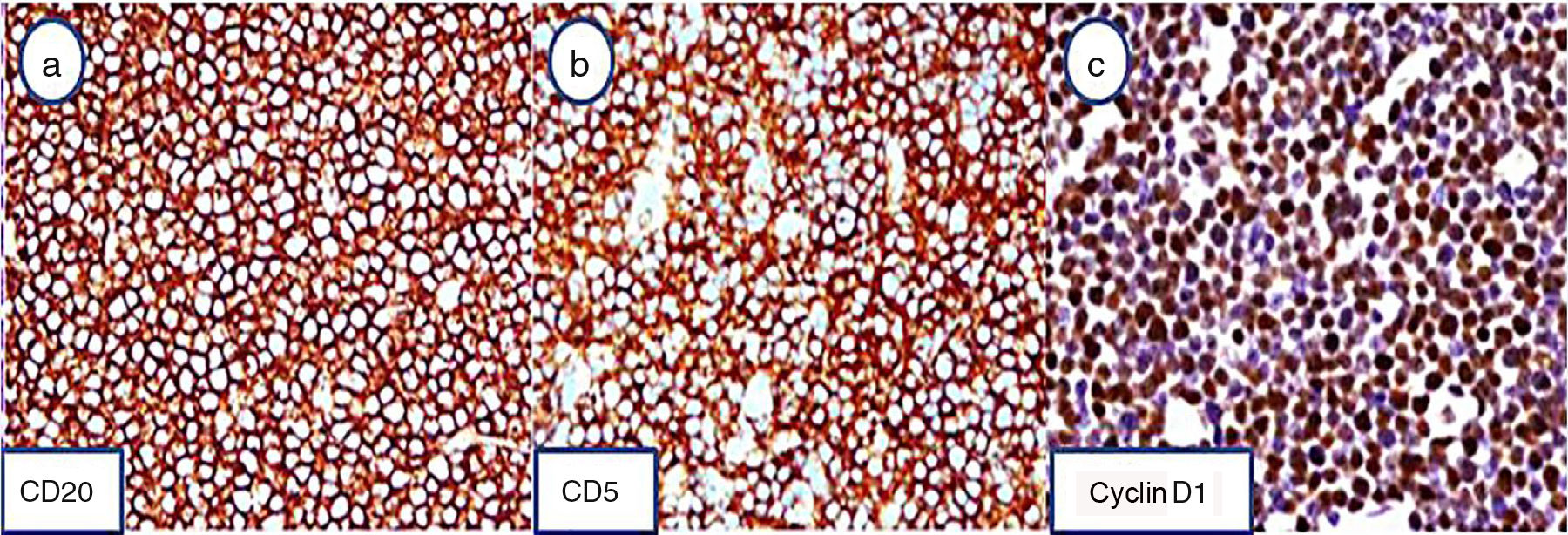
The disease is characterized by the presence of a monoclonal B-cell line population that expresses CD19, CD20, and CD5 markers on the surface of immunoglobulin M and FMC7. Cyclin D1 overexpression is associated with the presence of translocation t (11;14) and CD3, CD10, and CD23 are negative.3
Endoscopy is among the different tests available for mantle cell lymphoma diagnosis and it is very useful for characterizing lesions and taking biopsies for their histologic study. Up to 50% of patients can have normal mucosa.4,5
Endoscopic findings vary from the most common manifestation, the so-called “lymphomatoid polyposis”, characterized by the identification of multiple lymphoid polyps principally in the small and large bowel, to superficial ulcers and tumors, generally observed at the ileocecal level, or normal-appearing mucosa. The ileocecal region of the bowel tends to be the most frequently affected, but the area from the stomach to the rectum can also be compromised.6
In different prospective studies, microscopic infiltration of the gastrointestinal mucosa by mantle cell lymphoma, with no apparent macroscopic lesions, has been demonstrated.7
Approximately 90% of the patients that present with multiple lymphomatous polyps in the gastrointestinal tract have clinical manifestations such as weight loss, asthenia, fatigue, anemia, palpable abdominal or rectal tumor, and superficial adenopathies. The biologic behavior of mantle cell lymphoma is very aggressive, with mean patient survival of 3-5 years. Systemic chemotherapy is the treatment that offers the best results.8,9
The aim of the present study was to analyze the clinical and endoscopic characteristics of mantle cell lymphoma affecting the upper and lower gastrointestinal tract.10
Materials and methodsA retrospective and descriptive case series was conducted on patients diagnosed with mantle cell lymphoma that affected the gastrointestinal tract. The patients were retrieved from a review of the archives of the Instituto Nacional de Cancerología (INCAN) in Mexico City covering a 10-year period, utilizing the Keywords: mantle cell lymphoma. The following variables were selected from the case records that were identified: age; sex; initial symptoms; digestive symptoms; affected site; and endoscopic lesion characteristics. Demographic; clinical; and endoscopic variables were reviewed.
Measures of central tendency, percentages, and ranges of the demographic and endoscopic findings were calculated.
Because the study was retrospective, it was exempt from review by the institutional ethics committee.
ResultsThe demographic and endoscopic findings in 10 patients diagnosed with mantle cell lymphoma are described. All patients underwent endoscopic examination ordered by the treating physician. Biopsies were taken only from the patients with macroscopically visible lesions, all of which resulted in the diagnosis of mantle cell lymphoma. Seven of the patients were men and 3 were women, and the mean patient age at diagnosis was 65 years. The symptoms present at the time of diagnosis were: weight loss in 6 patients, asthenia and adynamia in 4 patients, and digestive symptoms in 3 patients. The 10 patients studied presented with clinical stage IVB (Table 1).
Demographic characteristics.
| Patient | Sex | Age Dx | Initial symptom | Primary lesion | Digestive symptoms |
|---|---|---|---|---|---|
| 1 | M | 86 | Asthenia, adynamia,digestive symptoms,weight loss | None | Anorexia, upper gastrointestinal bleeding, abdominal pain |
| 2 | M | 86 | Digestive symptoms,weight loss | None | Anorexia, upper gastrointestinal bleeding, abdominal pain |
| 3 | M | 63 | Anorexia,weight loss | Cervical adenomegalyEpigastric tumor | Anorexia |
| 4 | F | 63 | Asthenia, adynamia,syncope | Inguinal adenomegalyJaundice | None |
| 5 | M | 56 | Anorexia,asthenia, adynamia,digestive symptoms,rash, papules | HepatomegalySplenomegalyCervical adenopathyInguinal adenopathyEpigastric tumor | AnorexiaPostprandial fullnessBloating |
| 6 | M | 64 | Digestive symptoms | None | None |
| 7 | F | 65 | Odynophagia | Cervical adenomegalyNeck tumor | None |
| 8 | F | 65 | Anorexia, odynophagia | Cervical adenomegaly | None |
| 9 | M | 62 | Digestive symptoms,Nocturnal diaphoresis | Cervical adenomegaly | None |
| 10 | M | 40 | Digestive symptoms | Cecal tumor | BloatingAbdominal painChanges in bowel habit |
Six patients had lymphadenopathy that was diagnostic for lymphoma: 4 in the cervical region and 2 in the inguinal region. They also presented with epigastric tumor and tumor of the amygdala.
Of the patient total (n = 10), 5 presented with digestive symptoms. The main symptoms were anorexia, bloating, and abdominal pain, followed by postprandial fullness, upper gastrointestinal bleeding, nausea, and changes in bowel habit. The other 5 patients had no associated symptoms (Table 2).
Upper gastrointestinal endoscopy.
| Patient | Endoscopic findings | Affected site |
|---|---|---|
| 1 | Thickened folds, polypoid lesions, ulcerated lesion | Esophagus, antrum, corpus, pylorus, and duodenum |
| 2 | Infiltrating lesion, ulcerated lesion, polypoid lesion, excavated lesion | Antrum, duodenum, and pylorus |
| 3 | Thickened folds, polypoid lesion | Antrum, corpus, fundus, pylorus, and duodenum |
| 4 | Polypoid lesion | Antrum |
| 5 | Polypoid lesion, nonspecific changes in the mucosa | Pylorus |
| 6 | Nonspecific changes in the mucosa | Antrum and corpus |
| 7 | Thickened folds, infiltrating lesion, nonspecific changes in the mucosa | Antrum, corpus, fundus, and incisura |
| 8 | Polypoid lesion, nonspecific changes in the mucosa | Corpus and duodenum |
| 9 | Exophytic tumor, thickened folds, infiltrating lesion, polypoid lesion | Antrum, corpus, fundus, and duodenum |
| 10 | Upper gastrointestinal endoscopy was not performed |
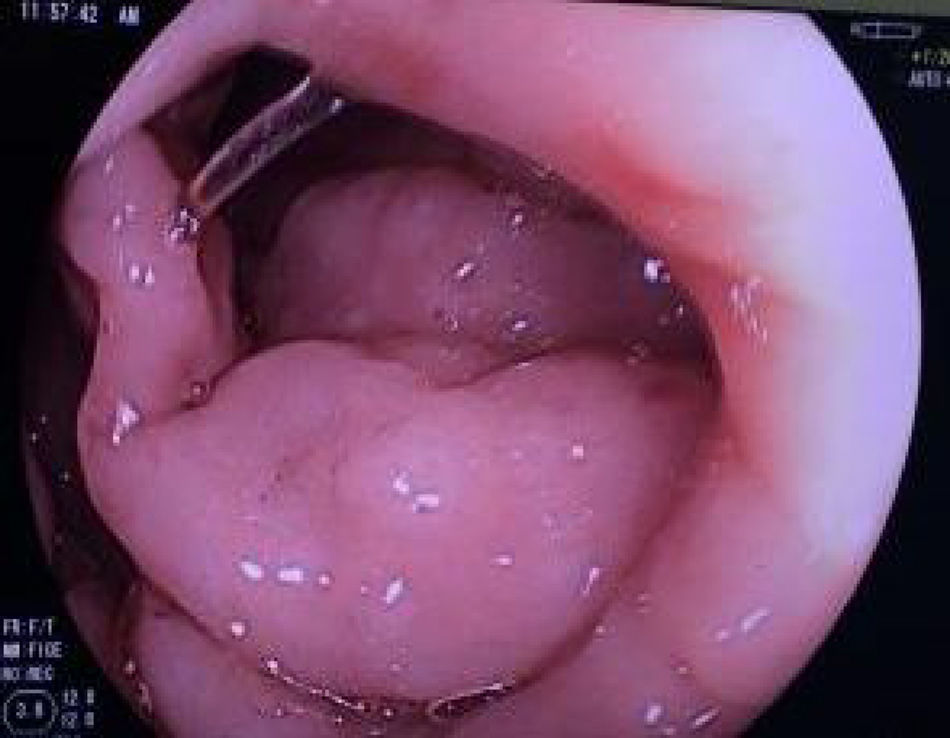
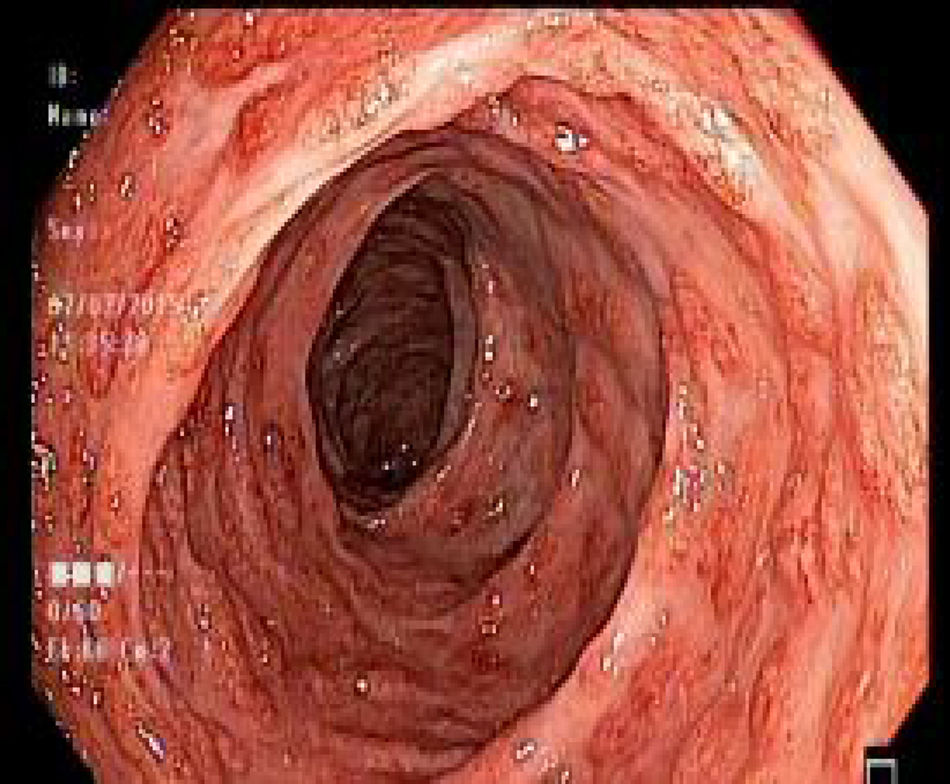
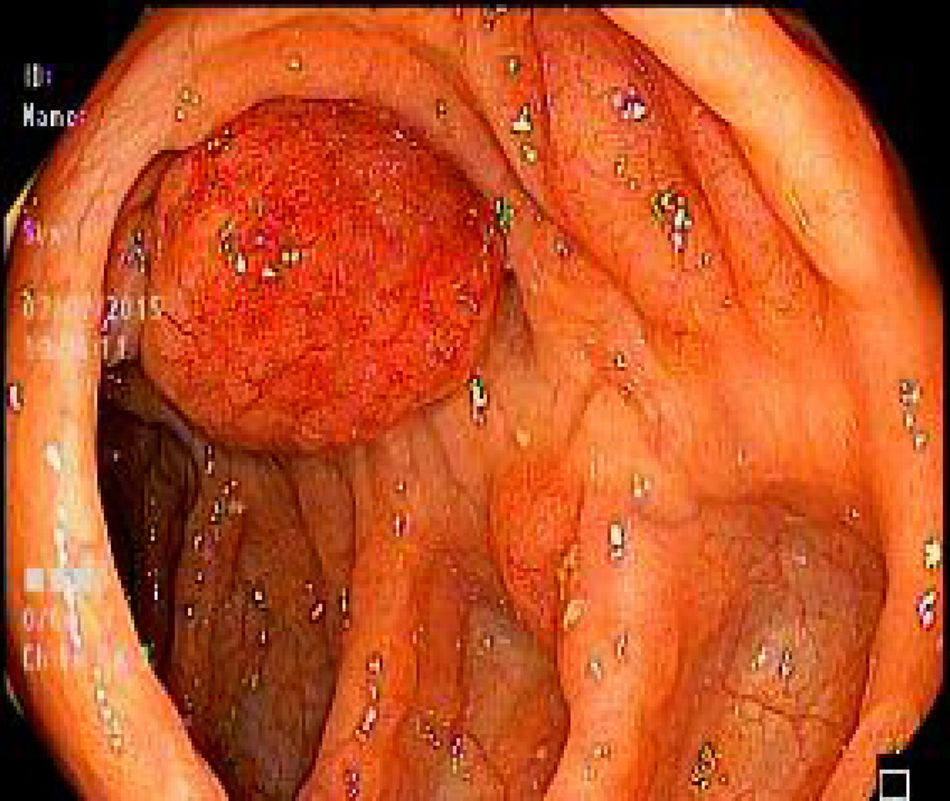
Of the 10 patients studied, 4 underwent both upper endoscopy and colonoscopy, one patient underwent colonoscopy alone, and 5 patients underwent upper endoscopy alone. The findings described at upper endoscopy were: polypoid lesions, thickened folds, nonspecific changes of the mucosa, and infiltrating lesions (figs. 1-3).
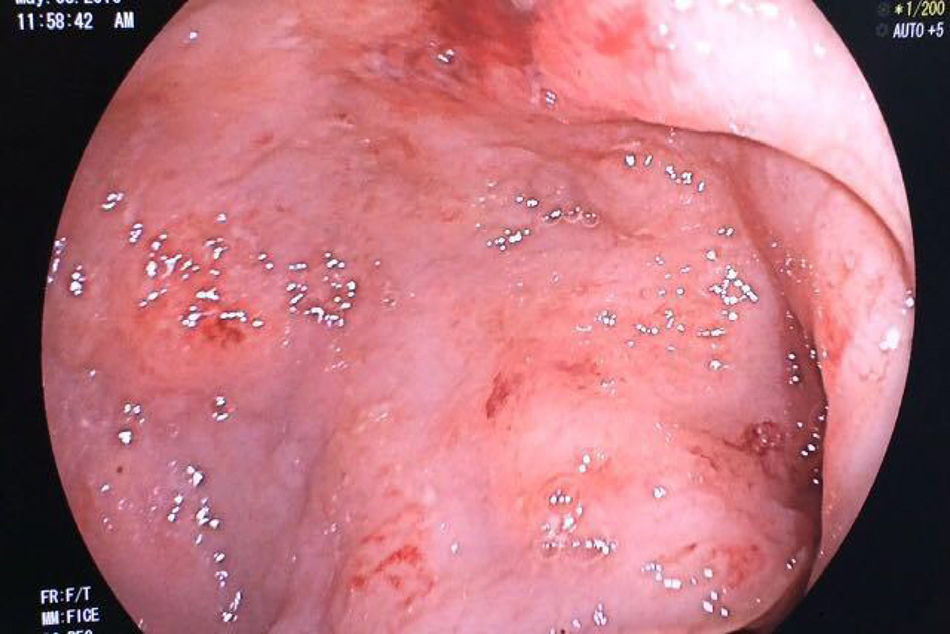

The most affected sites of the upper gastrointestinal tract were the antrum, corpus, and duodenum (Table 3).
Colonoscopy.
| Patient | Endoscopic findings | Site affected |
|---|---|---|
| 1 | Polypoid lesion, ulcerated lesion, tumor lesion | Ascending colon, transverse colon, descending colon, sigmoid colon, and rectum |
| 2 | Colonoscopy was not performed | |
| 3 | Polypoid lesion, edematous mucosa | Cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum |
| 4 | Colonoscopy was not performed | |
| 5 | Polypoid lesion | Cecum, transverse colon |
| 6 | Colonoscopy was not performed | |
| 7 | Colonoscopy was not performed | |
| 8 | Polypoid lesion | Cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum |
| 9 | Colonoscopy was not performed | |
| 10 | Ulcerated lesion, polypoid lesion | Sigmoid colon and rectum |
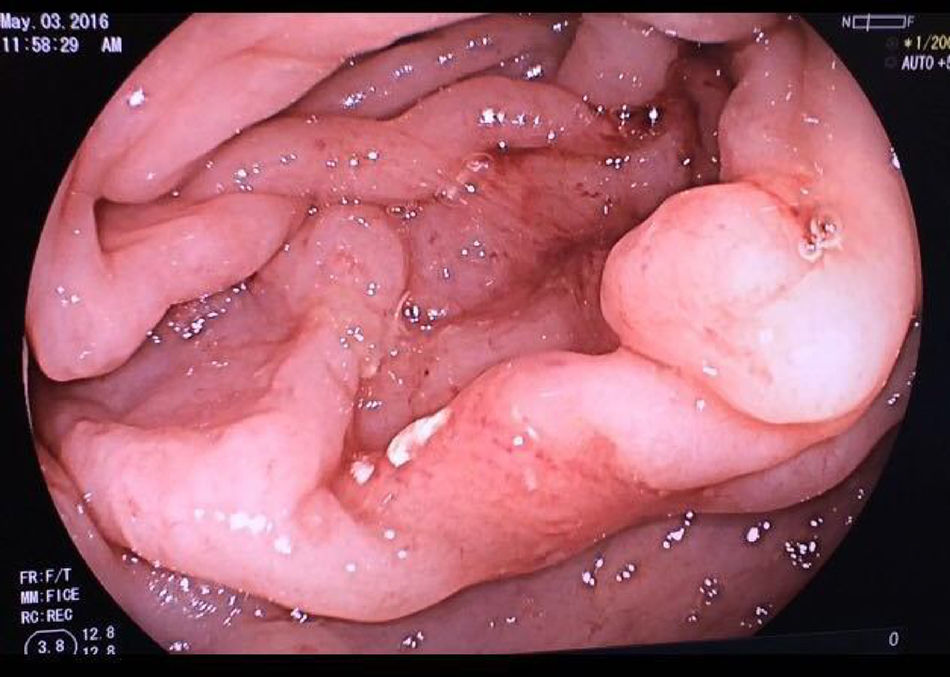
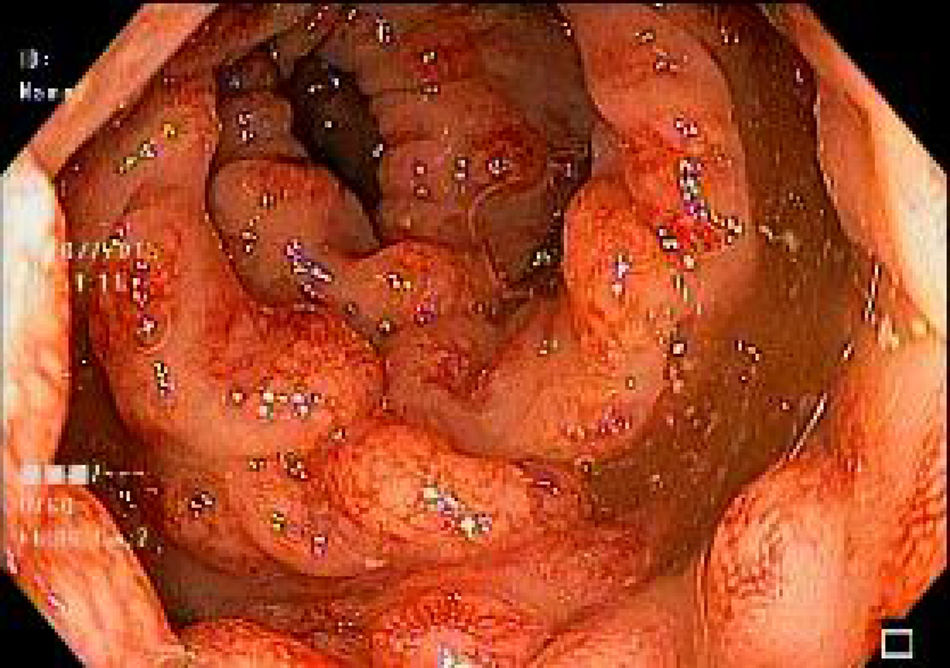
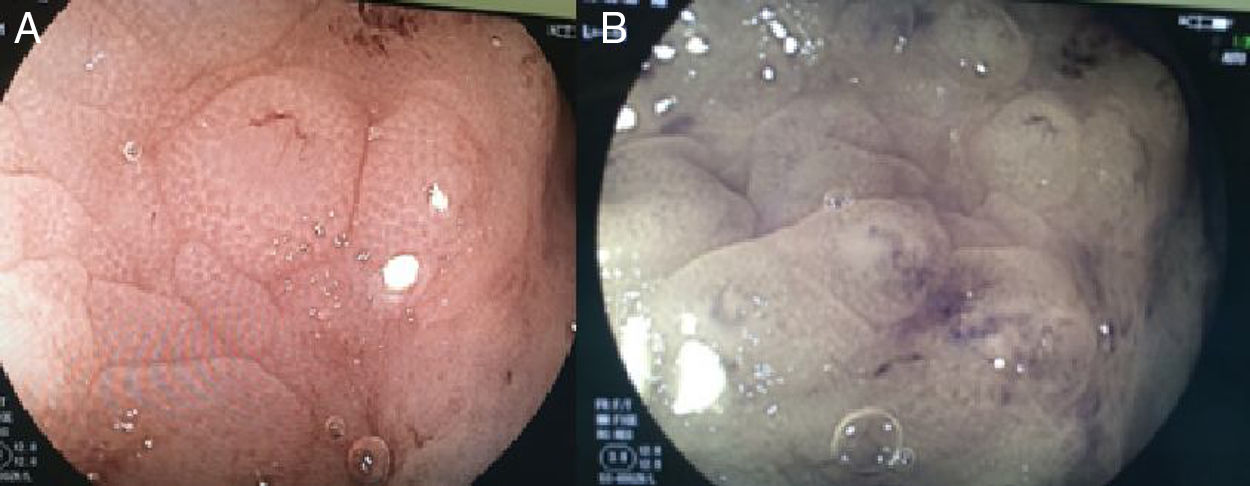
The findings described at colonoscopy were: polypoid lesions, ulcerated lesions, and tumor lesion (figs. 4 and 5 a,b).
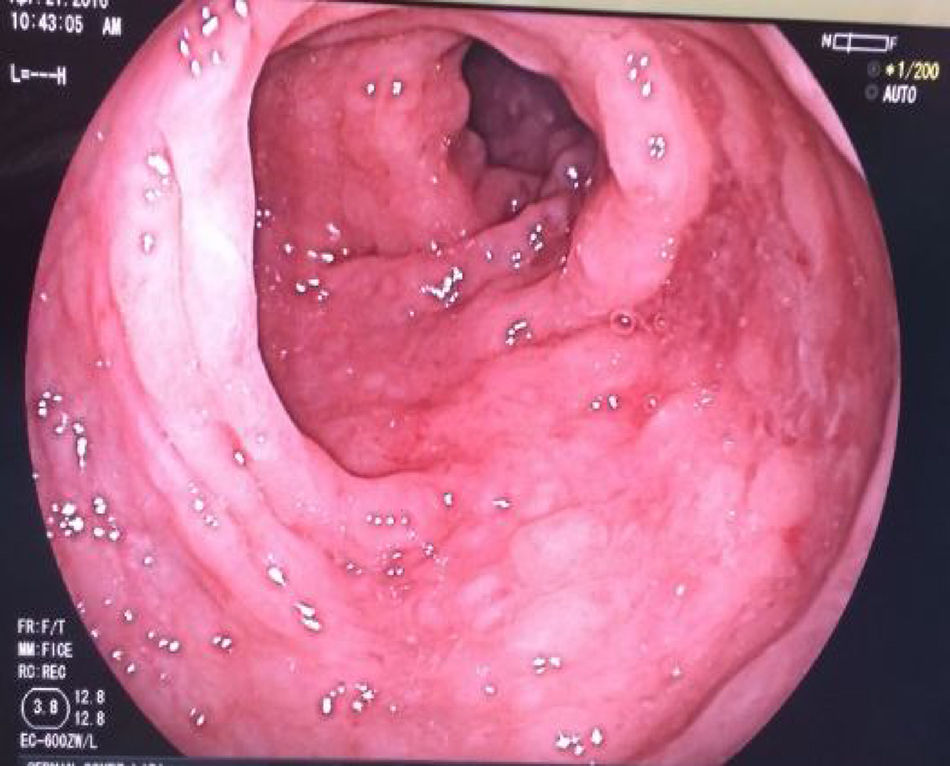
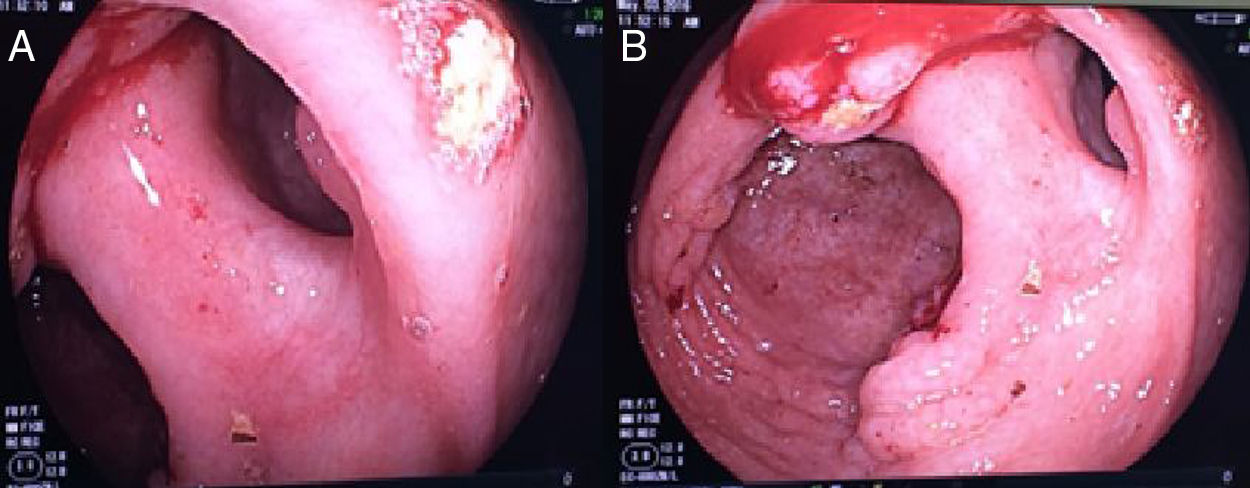
The most affected sites were the transverse colon, sigmoid colon, and rectum (Table 3) (figs. 6-10 a,b).
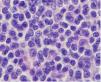
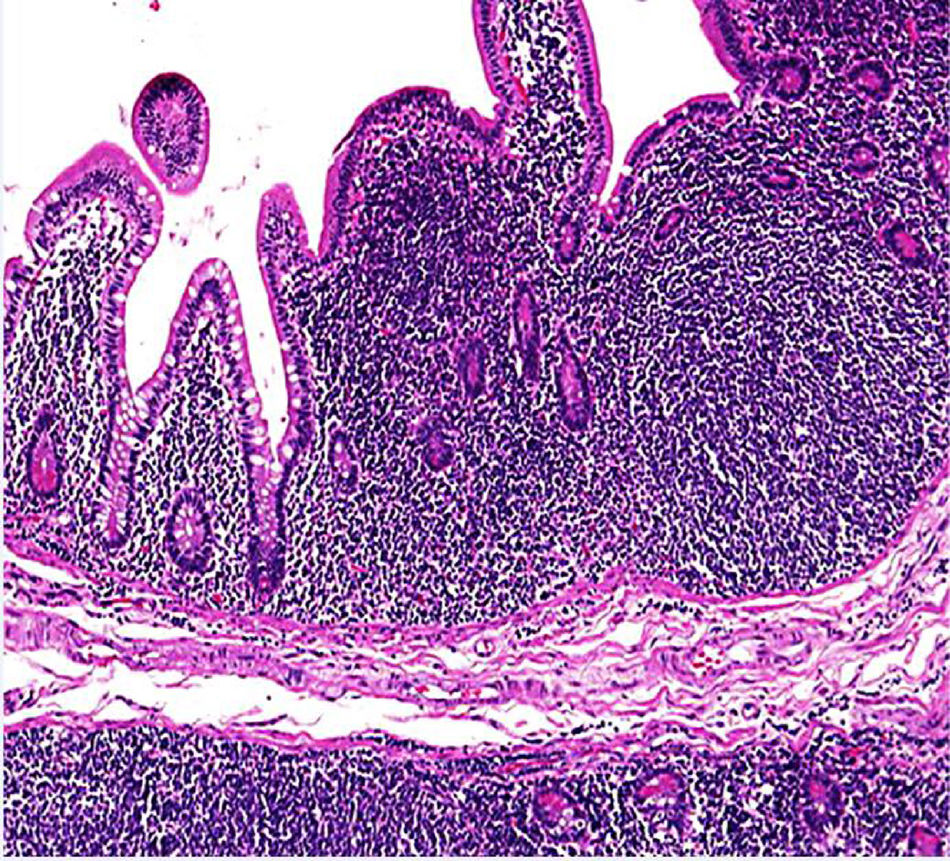
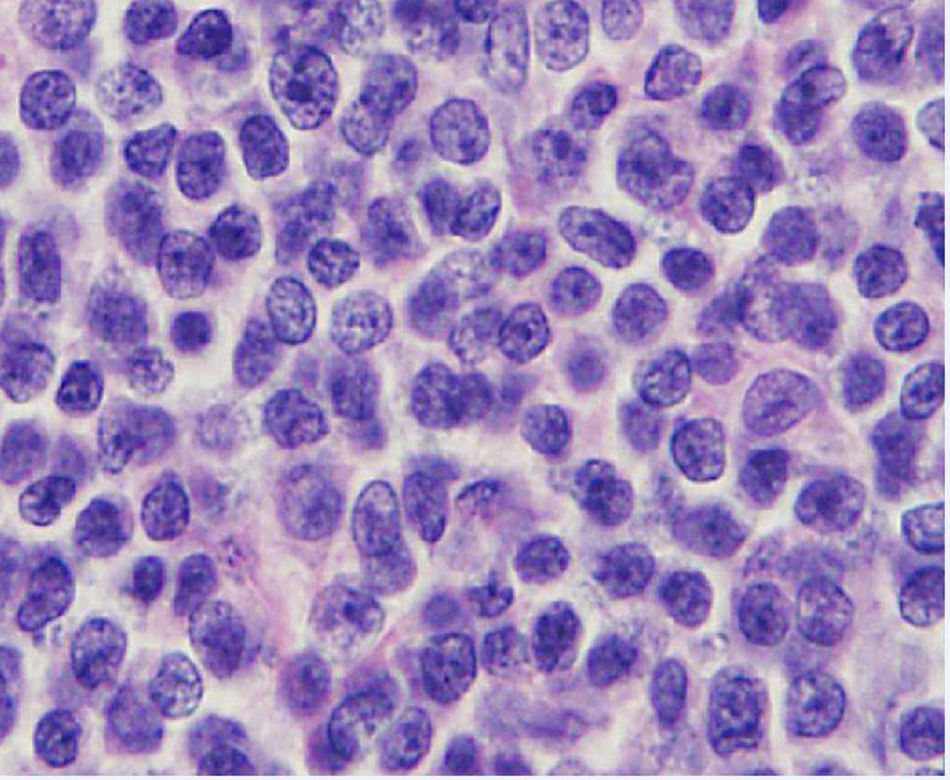
Among the histopathologic tumor features, the lymphomas identified in our case series were characterized by a proliferation of small, cleaved lymphocytes in a nodular arrangement in the submucosa or the mucosa of the affected segments (fig. 11). Cytologic evaluation revealed a hyperchromatic, small (7μm in diameter), cleaved nucleus with scant cytoplasm (fig. 12). Immunohistochemical tests were carried out in all the cases to corroborate the diagnosis, and they showed positivity in the cytoplasmic membrane for CD20 and CD5 in the neoplastic B-lymphocytes (fig. 13 a,b) and positivity for cyclin D1 in the nuclei of the neoplastic lymphocytes (fig. 13c), thus confirming the diagnosis. Only atrophy of the epithelium and edema were identified in the mucosa adjacent to the tumors. No intraepithelial lymphocytosis or pathogenic microorganisms were observed, and the presence of H. pylori was not identified in the gastric biopsies.
A mean patient age at the time of mantle cell lymphoma diagnosis of 60 years and a greater frequency in the male sex are described in the medical literature. Gastrointestinal involvement of 15 to 30% is also reported.1,2
The findings of the present review concur with those data. Our patients had a mean age of 65 years at diagnosis and 70% of them were men.
“Lymphomatoid polyposis” in the small and large bowel, superficial ulcers, tumors generally at the ileocecal level, and at a lower percentage, normal-appearing mucosa are among the mucosal lesions described in the literature.6 The endoscopic findings at upper endoscopy reported in our study were polypoid lesions (66%), thickened folds (44%), and nonspecific changes in the mucosa (33%). Only 3 patients had infiltrating lesions. The most affected site in the stomach was the antrum in 77% of the patients, followed by the corpus in 66%, and the duodenum in 55%.
Of the patients that underwent colonoscopy, 100% had polypoid lesions, ulcerated lesions were reported in 40%, and edematous mucosa and tumor lesion in 20%. The transverse colon, sigmoid colon, and rectum were affected in 60% of the patients.
Because the study was retrospective, upper endoscopy and colonoscopy were not performed in all the patients, which was a limitation of our review.
With the data obtained, we conclude that endoscopic studies are a tool with a low complication rate that can be very useful in the diagnosis, management, and follow-up of patients with mantle cell lymphoma. It is of great value to know the gastrointestinal involvement of those patients to treat the lesions that are present and offer the patients a better quality of life and specific treatment at the affected sites.
It is important to study the gastrointestinal involvement in patients with mantle cell lymphoma, even in those patients that have nonspecific symptoms, given that digestive tract compromise impacts disease stage. Examination should include upper endoscopy and colonoscopy, whenever possible.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Oña-Ortiz FM, Sánchez-del Monte J, Ramírez-Solís ME, de la Mora-Levy JG, Alonso-Larraga JO, Lino-Silva LS, et al. Linfoma del manto con afección del tubo digestivo. Revista de Gastroenterología de México. 2019;84:434–441.

