






One of the most important characteristics of malnutrition is the loss of muscle mass and the severe depletion of the protein reserve, secondarily affecting energy metabolism. That impacts nutritional status and the progression of disease-related complications.
Nutritional treatment is one of the main factors in the comprehensive management of those patients. Achieving adequate energy intake that provides the macronutrients and micronutrients necessary to prevent or correct malnutrition is attempted through dietary measures. ESPEN, the European Society for Clinical Nutrition and Metabolism, recommends a caloric intake of 30-40kcal/kg/day, in which carbohydrates provide 45-60% of the daily energy intake and proteins supply 1.0-1.5g/kg/day. The remaining portion of the total energy expenditure should be covered by lipids.
The administration of branched-chain amino acids has been shown to be beneficial not only in counteracting malnutrition, but also as a coadjuvant treatment in specific complications, thus playing a favorable role in outcome and quality of life.
Therefore, branched-chain amino acids should be considered part of nutritional treatment in patients with advanced stages of cirrhosis of the liver, particularly in the presence of complications.
Una de las características más importantes de la desnutrición en la cirrosis hepática es la pérdida de masa muscular y agotamiento grave de la reserva de proteínas, afectando de manera secundaria al metabolismo energético; esto influye en el estado nutricional y en la evolución de algunas complicaciones de la enfermedad.
El tratamiento nutricional es uno de los principales factores en el tratamiento integral en estos pacientes, ya que a través de la alimentación se busca lograr un adecuado consumo de energía que provea los macro- y micronutrientes necesarios a fin de evitar o corregir la desnutrición. La ESPEN recomienda un aporte calórico de 30-40kcal/kg/día, en el cual los hidratos de carbono provean del 45-60% del aporte energético diario, y las proteínas aporten de 1.0-1.5g/kg/día, el resto del gasto energético total debe ser cubierto por lípidos.
Se ha demostrado que la administración de aminoácidos de cadena ramificada no solo resulta benéfico para contrarrestar la desnutrición, sino también como tratamiento coadyuvante en complicaciones específicas como encefalopatía hepática, ascitis e incluso en carcinoma hepatocelular, por lo que tienen un papel favorable en el pronóstico y la calidad de vida.
Debido a esto, el uso de aminoácidos de cadena ramificada en pacientes con cirrosis hepática en estadios avanzados, y particularmente cuando aparecen las complicaciones, debería considerarse como parte del tratamiento nutricional.
Cirrhosis of the liver is a diffuse disease of the liver that alters its structure and function and is the final stage of all chronic liver diseases.1 There are two phases in the natural history of the disease: compensated and decompensated. Compensated cirrhosis is characterized by being asymptomatic and presenting with nonspecific symptoms, whereas decompensated cirrhosis is characterized by the appearance of complications derived from portal hypertension, such as variceal bleeding, hepatic encephalopathy, and ascites, among others.2
One of the most frequent complications in both compensated and decompensated cirrhosis is malnutrition.3 Its presence is associated with greater mortality, adverse surgical outcomes, and increased risk for the development of complications inherent in cirrhosis.4
Included in the spectrum of malnutrition are progressive muscle mass loss, known as sarcopenia, as well as a syndrome that involves the loss of muscle mass, fat mass, and weight, associated with the proinflammatory state of the disease, known as cachexia.3 The etiology of malnutrition in cirrhosis is multifactorial and chiefly related to reduced food intake that can be caused by the increase in different proinflammatory cytokines with an anorexigenic effect, increased catabolism, and/or the presence of complications of cirrhosis, such as ascites and hepatic encephalopathy.5 Malnutrition in those patients is also related to a marked decrease in glucose oxidation, with greater fat and protein catabolism, similar to that observed in healthy subjects after 2 to 3 days of inanition. There is marked muscle mass loss and severe protein depletion, with the consequent alteration of tissue function, placing those patients at a high risk for morbidity and mortality.6,7
Nutritional treatment in cirrhosis of the liverDietary treatmentDietary treatment has shown benefits in both early and advanced disease stages. Initially, protein restriction was considered part of the standard treatment for cirrhosis, but that practice was based on observations and uncontrolled studies and on the idea that dietary proteins could induce hepatic encephalopathy (HE).8 It was previously suggested that high doses of protein in the diet could trigger or precipitate HE.9 That idea arose in 1893, when dogs with portal-caval diversion were fed an animal-based diet and developed neurologic symptoms. Those symptoms then improved when the dogs were fed a diet with different protein quality.10 In 1954, Sherlock et al. first demonstrated HE symptom control in cirrhotic patients through the introduction of a low-protein diet (20g/day).11 Based on those observations, dietary prescriptions acquired a special relevance and the restriction of protein ingestion in cirrhotic patients with HE became common practice.
Later studies with larger numbers of patients and greater methodological rigor showed that, contrary to what was previously thought, there was no important benefit in HE progression from restricting the quantity of protein in the diet and that said restriction could even cause greater protein degradation and favor the appearance of that complication.12 As a result, protein restriction is no longer recommended and should generally be avoided, given that it can worsen the nutritional status, without improving HE.
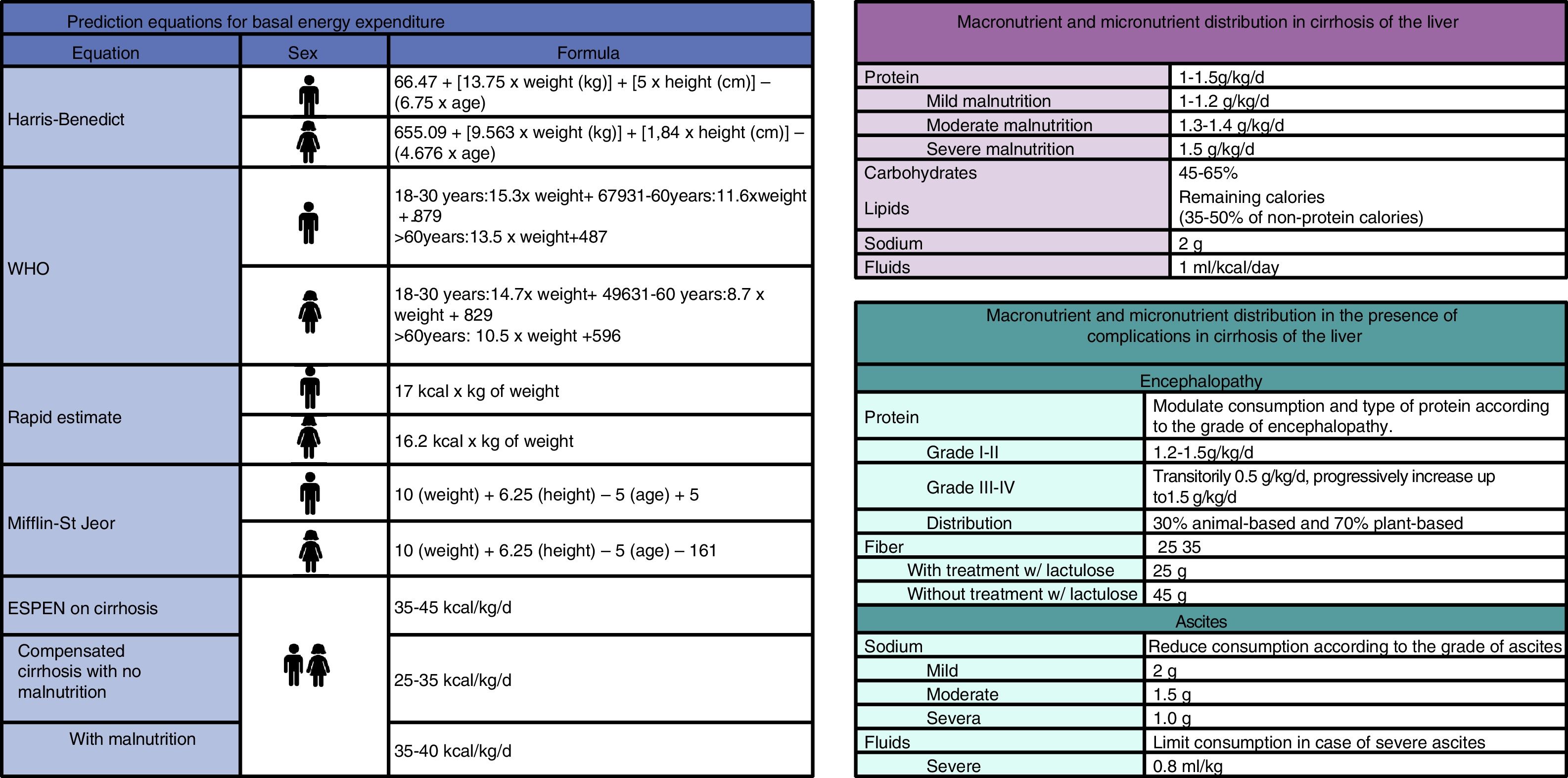
Nutritional recommendationsRecommendations of the European Society for Clinical Nutrition and Metabolism (ESPEN)Regarding macronutrients, the ESPEN suggests that carbohydrates (CHs) supply 45 to 65% of the dietary total energy and the protein recommendation is 1.0-1.5g/kg/day. The exact quantity should be determined in accordance with the nutritional status of the patient. The recommendation is 60-70% plant-based protein and the remaining percentage, animal-based. Once the carbohydrate and protein supply is established, the rest of the calories should be provided by lipids. In the patients that present with ascites and/or edema, the quantity of sodium should be restricted (<2g/day). Consumption of 30g/day of dietary fiber has been recommended, increasing the requirement in patients with hepatic encephalopathy6 (fig. 1). In addition, the ESPEN supports enteral supplementation with branched-chain amino acid (BCAA) formulas in patients with hepatic encephalopathy, as well as oral supplementation in patients with advanced cirrhosis. Supplementation with BCAAs can also be considered in children on the waiting list for liver transplantation.6
The recommendation for fluid intake according to the American Society for Parenteral and Enteral Nutrition stipulates that ideal consumption for any adult should be 1ml/kcal/day.13 Body water loss can be due to various factors (diarrhea, wounds, surgical drains, nasogastric drains, pancreatic secretions, urinary secretions, and the use of diuretics). Fluid restriction should be carried out when there is hyponatremia (sodium levels < 120 mmol/l).5
Late evening snackOne of the most widely used strategies supported by the literature is the addition of a late evening snack that contains CHs. Previous studies have shown that muscle mass and energy metabolism improve by meeting energy necessities required at night, which also increase due to hypercatabolism observed in cirrhosis.14 The calories derived from those snacks can vary between 200 and 400kcal and should contain complex CHs to prolong absorption during the night and provide dietary fiber. Patient preferences should also be considered for their prescription to ensure good adherence.15,16
In a clinical trial published in 2006, the efffect of the consumption of a 200-kcal portion of rice as a late evening snack in patients with cirrhosis of the liver with Child class A disease was evaluated and showed a clear improvement in the patients that had the late evening snack, improving metabolism measured through indirect calorimetry.17
Another strategy supported by the literature, in addition to the late evening snack with complex CHs, is the prescription of a late evening snack with BCAAs. In fact, a study that compared the late evening snack based on ordinary food with the snack with BCAAs showed that the latter significantly improved the nutritional parameters and the catabolic state. The BCAA mixture also elevated the nitrogen balance and serum albumin level, compared with an isocaloric food.14
Energy calculationThe gold standard for estimating the quantity of energy consumed is indirect calorimetry. When that method is not available, implementation of the ESPEN recommendations is suggested. They propose a caloric intake of 30-40kcal/kg of body weight per day, based on the actual weight of the patient, and in cases of ascites, on the ideal patient weight, or using energy calculation formulas (fig. 1).
The formulation of a nutritional plan in patients with cirrhosis requires knowing the stage of the disease, the complications present, comorbidities, physical activity performed, and nutritional data, as well as the quantity of kilocalories (kcals) needed. Energy requirements can be calculated through calorimetry, but since it is a method that is not very accessible, prediction equations are often used. To make the calculation, it is necessary to know the sex, height, and age of patients in addition to parameters previously described. There are different prediction formulas for obtaining the basal energy expenditure, according to the characteristics of each patient. In healthy persons, the World Health Organization formulas can be used, and the Mifflin-St. Jeor equation is suggested for obese patients. However, the Harris-Benedict formula is the most widely used for the general population, with separate equations for women and men. Once the basal energy expenditure is obtained, the kcals from the thermogenic effect of food and from physical activity are added to obtain the final result of a person's total energy expenditure.18 In patients with cirrhosis of the liver, that formula tends to underestimate energy expenditure, and so the ESPEN recommendations are suggested for those cases (fig. 2).6
Nutritional supplementation in cirrhosis of the liver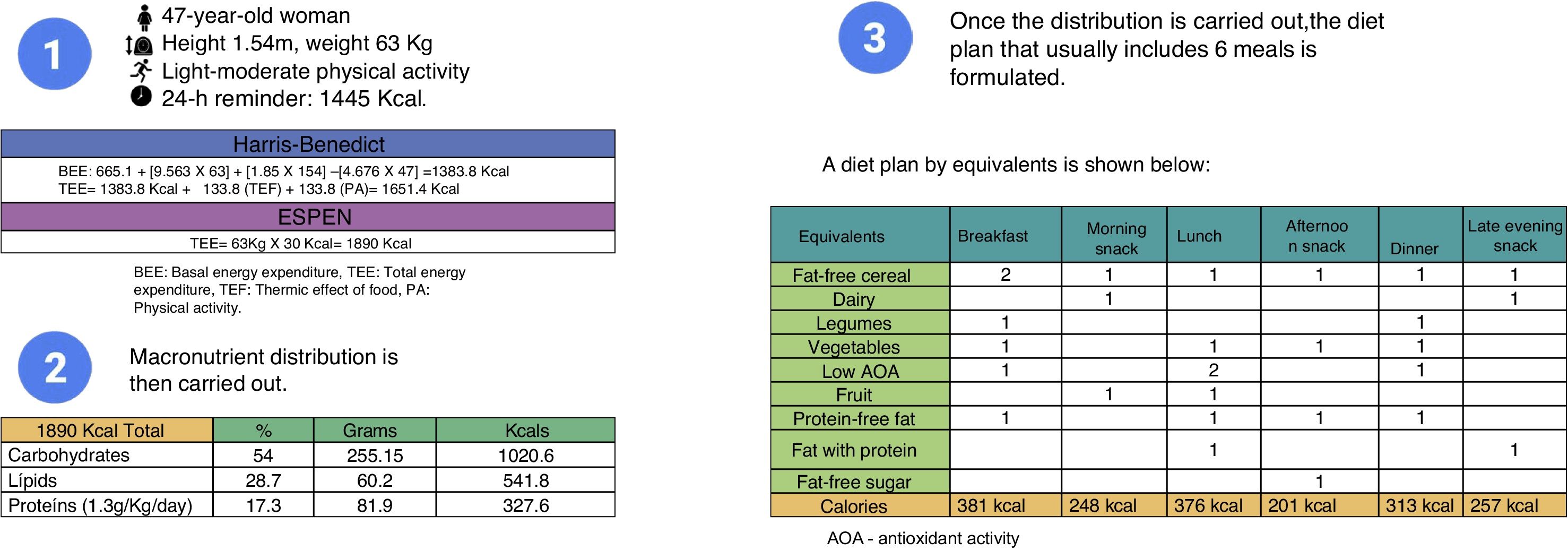
When dietary consumption is not sufficient for maintaining the energy requirements of a patient, oral supplementation with hypercaloric or high-protein formulas have been proposed. Thus, the patient can receive the energy necessary for overcoming the catabolic state characteristic of the disease.19 Supplementation with BCAA formulas are among the approaches that have been described, and are reported to be the most useful in improving the nutritional status and associated complications, such as HE, physical and mental fatigue, and immune system function.20
Hypercaloric formulasWith respect to the hypercaloric formulas, one study showed significant nitrogen balance improvement in patients that received enteral nutrition with a hypercaloric formula immediately after liver transplantation. Another study utilized an oral hypercaloric supplement in patients diagnosed with sarcopenia that were on the liver transplantation list. The supplementation was maintained until the day of the transplant, and significant improvement was observed in muscle mass and muscle strength, as well as a trend towards better pre-transplantation survival.21
Enteral administration of those formulas is limited to the patients that do not tolerate oral diet due to a comorbidity. Some authors have suggested that enteral nutrition is more efficient than oral diet in cirrhotic patients, even when the patient tolerates oral diet. Nevertheless, a recent study that included hospitalized patients with alcoholic hepatitis could not demonstrate survival improvement in patients that received intensive enteral nutrition, compared with those that received conventional oral diet. Moreover, enteral nutrition is not recommended outside of its conventional indications due to reported risks, such as aspiration pneumonia.22
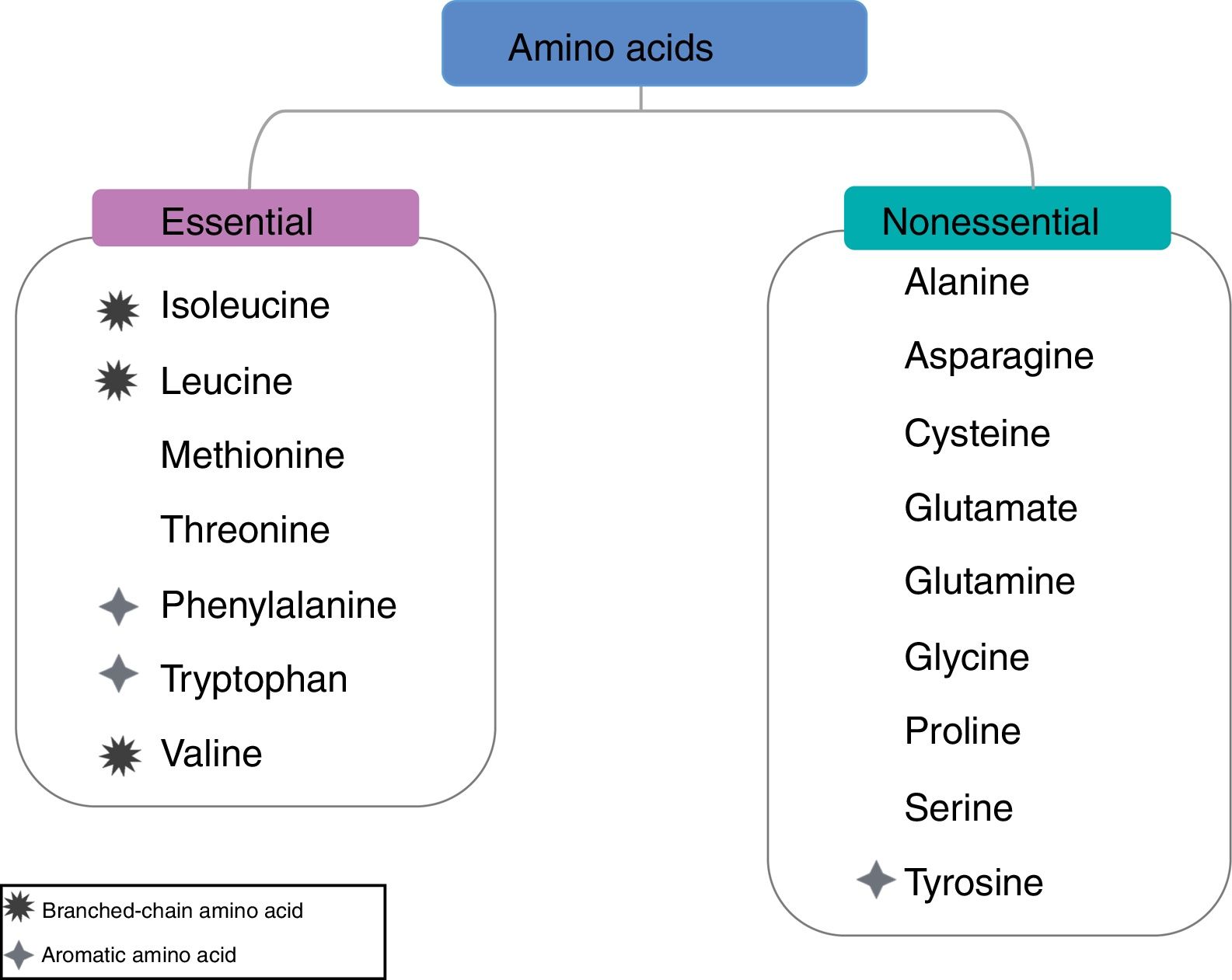
Branched-chain amino acidsA low ratio of plasma BCAAs to aromatic amino acids is a characteristic process of cirrhosis caused by several factors, including reduced dietary ingestion, hypercatabolism, and ammonia detoxification in skeletal muscle. In addition, it reduces albumin biosynthesis and secretion in the hepatocytes and is also associated with poor prognosis in patients with chronic liver disease. BCAAs have aliphatic lateral chains with a branching point and include valine, leucine, and isoleucine. They are not only protein components, but also a source of glutamate, which facilitates ammonia detoxification through glutamine synthesis. That reaction is catabolized by glutamine synthetase, present in skeletal muscle (fig. 3).23
Different studies have shown that BCAA administration stimulates liver protein synthesis, contributing to improving the nutritional status and quality of life of patients with cirrhosis of the liver 24 (Table 1).
Effect of BCAAs on the different outcomes of cirrhosis of the liver.
| Author and year | Intervention population vs. control | Aim | Intervention | Result | Limitations |
|---|---|---|---|---|---|
| Nakaya Y et al., 2007. 14 | 48 patients with CL (24 vs. 23) | To compare the effect of BCAAs and LES on the nutritional status and quality of life in patients with CL | Equicaloric supplementation of BCAAs vs. consumption of a carbohydrate-rich LES | Serum albumin level, nitrogen balance, and respiratory quotient significantly improved in the BCAA group | -Study was not blinded -Sex distribution between groups was not comparable |
Takeshita S et al., 2009. 35 | 56 patients with CL and HCC (28 vs. 28) | To evaluate whether a BCAA-rich LES improved liver function and nutritional status in patients that underwent TACE in the perioperative period | Consumption of an LES rich in BCAAs (50 g) 1 day before and 2 weeks after TACE | Albumin level, BTR, ChE, TC, and blood cell count were lower in the BCAA group | -Baseline clinical characteristics were worse in the BCAA group |
Kawamura E et al., 2009. 42 | 56 patients with CL (28 vs. 28) | To examine BCAA effectiveness using markers that indicate pre-transplantation liver reserve | Oral supplementation of 12.5 g/day of BCAA for one year | In the BCAA group, the MELD and CPT scores decreased, changes in TB and albumin were better conserved, and complication incidence was lower | -Lack of placebo -No protein synthesis or catabolism evaluation was carried out |
Lee IJ et al., 2011.33 | 37 patients with CL and HCC (20 vs. 17) | To evaluate oral BCAA supplementation in the biochemical and amino acid profiles of patients with liver tumors that underwent radiotherapy | Supplementation of 4.74g of BCAA 3 times/day after meals during radiotherapy treatment (5-6 weeks) | The percentage of patients that returned to normal serum albumin levels between 3-10 weeks after BCAA administration was significantly higher (41.18%) than in the placebo group (p=0.043). | -Supplementation was administered only during radiotherapy -Small sample |
Ichikawa K et al., 2013. 29 | 56 patients with CL and HCC (26 vs. 30) | To evaluate the effect of BCAA on the development of liver tumorigenesis after liver resection in patients with HCC | Oral supplementation of 4g/day of BCAA for 2 weeks before and 6 months after liver resection vs. conventional diet | The patients in the BCAA group showed a 28.5% accumulative recurrence rate of HCC vs. 55.7% in controls at 30 months after liver surgery | -Small number of patients |
Morihara D et al., 2012. 43 | 30 patients with CL and HCC (10 vs. 10 vs. 10) | To examine whether BCAA consumption as LES helped improve liver function in patients with HCC that underwent RFA | 1st group (control), 2nd group (6.5g of BCAA in the morning), 3rd group (LES 6.5g BCAA), 1 time/day for 12 weeks | The LES-BCAA group experienced rapid and significant improvement in albumin and TB levels and in CPT that began during the initial period after RFA | -Short follow-up period -Small sample |
Nishikawa H et al., 2012.32 | 99 patients with CL and HCC (40 vs. 59) | To examine the importance of treatment with BCAA before TACE in patients with HCC | Supplementation of 1.7g of BCAA, 3 times a day for 1 month before TACE | The patients with BCAA showed a significant difference in serum albumin level 1, 3, and 6 months after TACE and in the CPT score 3 and 6 months after TACE | -Retrospective study -Demographic characteristic bias between groups |
Marchesini G et al., 2003.25 | 174 patients 59 (BCAA) vs. 56 (L-ALB) vs. 59 (M-DXT) | To evaluate the effect of BCAA supplementation on liver failure, nutritional parameters, and quality of life | Group 1 (14.4 g/day BCAA=37.5 kcal), group 2 (2.1g of L-ALB with 4.0g of sucrose and 3.0g of mannitol=33.6 kcal), group 3 (2.4g of M-DXT plus 6.7g of sucrose=34.9 kcal), for one year | Treatment with BCAA reduced the combined rates of events, compared with L-ALB. The mean hospital admission rate and CPT score were lower in the BCAA group, compared with the L-ALB and M-DXT groups, and anorexia and health-related quality of life (SF-36 questionnaire) improved | Long-term compliance with BCAAs was poor |
Yoshiji H et al., 2013.44 | 93 patients with CL and HCC (51 vs. 42) | To examine the effect of BCAA on the accumulated recurrence of HCC under conditions of IR in clinical practice | Consumption of 12 g/day of BCAA for 60 months plus local curative therapy under the condition of IR | The patients with BCAA had reduced accumulated recurrence of HCC. In patients with a high IR index ([HOMA]-IR > 2.5), HOMA-IR improved and VEGFR2 was inhibited, together with those clinical effects | Adherence to treatment with BCAA (60 months) was not measured |
Tomoaki Ishihara et al., 2014.34 | 270 patients with CL and HCC -TACE (76 vs. 86) -RFA (40 vs. 68) | To study BCAA usefulness before TACE or RFA | Oral supplementation of 12.5g of BCAA for two weeks prior to the intervention with TACE or RFA vs. those that did not receive the supplementation beforehand | Pre-intervention BCAA suppressed the development of post-intervention hypoalbuminemia and reduced the inflammatory reactions during the later clinical course. The Δ CRP and albumin level were lower in patients treated with BCAA 2, 5, and 10 days after TACE | -The time of supplementation before the intervention was very short (2 weeks) |
Park JG et al., 2017.45 | 82 patients with CL (41 vs. 41) | To study the effect of BCAA supplementation on the MELD score and the complications of cirrhosis of the liver | The BCAA group was divided into 3 different dose groups (4.15?g, 8.3?g, and 12.45 g/day), supplemented for 6 months | The MELD score improved in the group of 12.45g BCAA, compared with the controls. The changes in the serum bilirubin level and CPT score also differed significantly between the 2 groups over time | -The guidelines for BCAA use varied between centers -Eating habits were not evaluated |
| Ruiz-Margáin et al., 2017.19 | 72 patients with CL (37 vs. 35) | To evaluate the effect on nutritional status of the combination of a high-protein and high-fiber diet with BCAA supplementation for a period of 6 months | Intervention group: diet of BCAA (110 g) + HPHF (1.2 g/kg of protein and 30g of fiber) Control group: diet HPHF (1.2 g/kg of protein and 30g of fiber) | No significant increase in ammonia or glucose levels was shown in either group, reflecting the safety of supplementation with BCAA. There was an increase in muscle mass and a decrease in fat mass in the BCAA group | -Sample size was calculated only for the primary aim, which was nutritional status |
BCAA: branched-chain amino acids; BTR:BCAA-to-tyrosine ratio; ChE: cholinesterase; CL: cirrhosis of the liver; CPT: Child-Pugh-Turcotte; CRP: C-reactive protein; HCC: hepatocellular carcinoma; HOMA-IR: Homeostatic Model Assessment of Insulin Resistance; HPHF: high-protein high-fiber; IR: insulin resistance; L-ALB:L-albumin; LES: late evening snack; MELD: Model For End-Stage Liver Disease; M-DXT: maltodextrin; RFA: radiofrequency ablation; TACE: transarterial chemoembolization; TB: total bilirubin; TC: total cholesterol; VEGFR2: vascular endothelial growth factor receptor 2; Δ: basal.
A pilot study evaluated the efficacy of oral supplementation with BCAAs and the effect on the liver reserve for the purpose of prolonging the time on the liver transplantation waiting list. The patients of both groups had a diet based on the ESPEN guidelines for liver disease and only the experimental group received the BCAA supplement (952mg of L-isoleucine, 1904mg of L-leucine, 1144mg of L-valine) 3 times a day. At the end of treatment, the Child-Pugh severity scales and MELD score decreased in the group that received the BCAAs.26 In another randomized, multicenter study, oral BCAA supplementation was compared with a group that received a similar quantity of nitrogen with lactalbumin (L-ALB) and another group that received a similar quantity of calories based on maltodextrins (M-DXT) for 12 months in 174 patients with decompensated cirrhosis. Long-term BCAA supplementation showed greater benefit, compared with the L-ALB and M-DXT groups, given that there was a decrease in progressive liver disease, reduced hospital admission rates, lower Child-Pugh scores, and a decline in bilirubin levels, as well as improved quality of life.25
Effect of branched-chain amino acid supplementation in complications of cirrhosisMalnutritionThe dual effect of a high-protein and high-fiber diet plus BCAA supplementation was previously evaluated, comparing it with only a high-protein and high-fiber diet. The high-protein and high-fiber diet consisted of 1.2g/kg/day of protein and 30g/day of fiber. The intervention group received 110g/day of the BCAA supplementation for a period of 6 months. At the end of the study, the patients in the intervention group receiving the diet plus the BCAAs had an increase in muscle mass and a decrease in fat mass.19
Hepatic encephalopathyIn 2009, a randomized, double-blind, multicenter study was published in which cirrhotic patients with at least one HE episode prior to their inclusion in the analysis were compared. They received identical caloric intake (35kcal/kg/day), but a varying quantity of protein (1 to 1.2g/kg/day, rich in BCAAs vs. 0.7g/kg/day) and were followed for one year. The group that received the normal protein diet enriched with BCAAs showed improvement in neuropsychometric tests and nutritional parameters, as well as a trend toward shorter HE duration. No differences were found in relation to HE recurrence (47 vs. 34%; p=0.27) or in liver function.26,27
The International Society for Hepatic Encephalopathy and Nitrogen Metabolism recently carried out a consensus on the nutritional management of patients with cirrhosis and encephalopathy, in which a special recommendation of BCAA supplementation was made.28,29
And finally, an up-to-date meta-analysis that included eight randomized controlled trials indicated that BCAA-enriched oral formulas improved episodic HE manifestations.30,31
Hepatocellular carcinomaBCAAs are beneficial in patients with hepatocellular carcinoma. A lower risk for developing hepatocellular carcinoma has been observed in patients that received BCAA supplementation.32 Furthermore, different studies published in recent years have shown the importance of nutritional supplementation with BCAAs in patients with hepatocellular carcinoma, prior to locoregional treatment with radiofrequency ablation (RFA), hepatic artery infusion chemotherapy, or transarterial chemoembolization (TACE), given that improvement in the nutritional status and liver function was observed, as well as better treatment response.33–36
AscitesHypoalbuminemia is directly associated with the development and persistence of ascites in patients with CL. Ascites induces abdominal distension and anorexia, which perpetuates hypoalbuminemia. Diuretic agents and albumin infusion are currently the only palliative treatment for ascites.36 BCAA supplementation complements albumin synthesis through an increase in the ratio of BCAAs to aromatic amino acids.19
In addition, BCAAs activate the mammalian target of rapamycin (mTOR) pathway with a later increase in protein synthesis.36 Some of the previously described studies support the improvement of hypoalbuminemia through BCAA supplementation.23,37
Interestingly, due to the fact that some patients show no increase in serum albumin after supplementation with BCAAs, one study evaluated the possible factors involved, such as dietary ingestion and baseline characteristics of the patients. The authors reported that the continuous use of BCAAs significantly reduced the incidence of ascites and edema, even in patients whose serum albumin did not respond to treatment with BCAAs.38
Quality of lifeQuality of life is defined by the World Health Organization as “individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”.
Different studies have demonstrated that patients with CL have a lower quality of life, compared with the healthy population, due to the complications of the disease and the limitations that it creates in activities of daily living, as well as the psychologic factors and treatment side effects.39–41
Supplementation with BCAAs has been shown in different randomized controlled trials to improve the general perception of health as measured utilizing the SF-36 questionnaire, compared with control groups.25,38 The possible mechanism through which BCAA supplementation could improve quality of life is that improved cerebral blood flow helps counterbalance fatigue and sleep disorders.23
ConclusionsMalnutrition in patients with cirrhosis of the liver is one of the most frequent complications and is also related to disease outcome. Therefore, nutritional treatment in those patients is essential to prolong survival, improve quality of life, and prepare patients for successful liver transplantation, helping to reduce the days of hospital stay and susceptibility to postoperative infections.
Ensuring adequate daily energy intake is one of the main goals of nutritional treatment, and there are different prediction equations that help calculate the total energy expenditure of a patient. However, they tend to underestimate energy intake in cirrhotic patients, thus the ESPEN recommendations appear to be the better option. According to the ESPEN, a caloric intake of 30-40kcal/kg of body weight per day of the patient's actual weight provides enough energy, whereas in the patient with fluid overload, ideal patient weight is recommended for making calculations with that formula. Carbohydrates should supply 45-60% of the daily energy expenditure. Protein intake should be 1.0-1.5g/kg/day, of which 70% should be plant-based and 30% animal-based, and the remaining energy expenditure should come from lipids.
The use of BCAAs as a nutritional supplement is the best option available in patients that do not reach the caloric requirement through diet, or as a coadjuvant in the treatment of complications characteristic of the disease.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Astrid Ruiz Margáin wishes to thank the Consejo Nacional de Ciencia y Tecnología (CONACYT) and Ricardo Macías Rodríguez wishes to thank the CONACYT-UNAM and the INCMNSZ Sponsorship.
Please cite this article as: Ruiz-Margáin A, Méndez-Guerrero O, Román-Calleja BM, González-Rodríguez S, Fernández-del-Rivero G, Rodríguez-Córdova PA, et al. Manejo dietético y suplementación con aminoácidos de cadena ramificada en cirrosis hepática. Revista de Gastroenterología de México. 2018;83:424–433.

