

Small bowel volvulus (SBV) is defined as the torsion of a small bowel loop around its mesentery axis. It may result in partial or complete obstruction. That condition after laparoscopic appendectomy has rarely been described. The diagnosis of SBV may be suggested by an abdominal computed tomography (CT) scan that shows the “whirlpool sign”, which is caused by twisting of the small bowel, mesentery, and mesenteric vessels1.
A 19-year-old man with no past medical history was admitted to the emergency department on postoperative day 6, after an uneventful laparoscopic appendectomy for a suppurative appendix. The appendectomy was performed with a 3-trocar technique and the appendiceal stump and mesoappendix were secured with an EndoGIA™ stapler (Ethicon Endosurgery, Cincinnati, OH, USA), with no complications. The patient presented with severe diffuse abdominal pain, accompanied by nausea, with no vomiting. Physical examination revealed normal vital signs, mild diffuse abdominal tenderness, and reduced bowel sounds.
The laboratory work-up showed normal hemoglobin of 13.7 g/dl and elevated white blood count of 14.5 × 1010. There were no other abnormal lab results. An abdominal X-ray showed no abnormalities, but an abdominal CT scan identified free fluid in the perihepatic and perisplenic regions, as well as a whirlpool sign on the mesentery of the terminal ileum, in the sagittal view, suggesting SBV (Fig. 1A). Diagnostic laparoscopy was performed, visualizing free hematic fluid and necrosis of the terminal ileum, secondary to a volvulus at that site. The procedure was converted to open surgery and the terminal ileum volvulus was then devolvulated. Necrosis was found 10 cm from the ileocecal valve, compromising 40 cm of the terminal ileum (Fig. 1B). A loose staple was observed on the peritoneal surface of the small bowel mesentery, 7 cm from the distal region of the necrotic bowel. A 50 cm intestinal resection was completed, followed by a stapled side-to-side anastomosis, using GIA™ 60 blue (Covidien, Mansfield, Massachusetts, USA). The patient had a satisfactory immediate postoperative outcome, referring only to mild pain during the first postoperative day. Oral diet was reintroduced on postoperative day 3. He was discharged home on the fifth postoperative day, with adequate oral intake and regular bowel movements.
 Sagittal view of the CT scan. The red arrow indicates the whirlpool sign in the mesentery of the terminal ileum. (B) Intraoperative image showing bowel ischemia.")
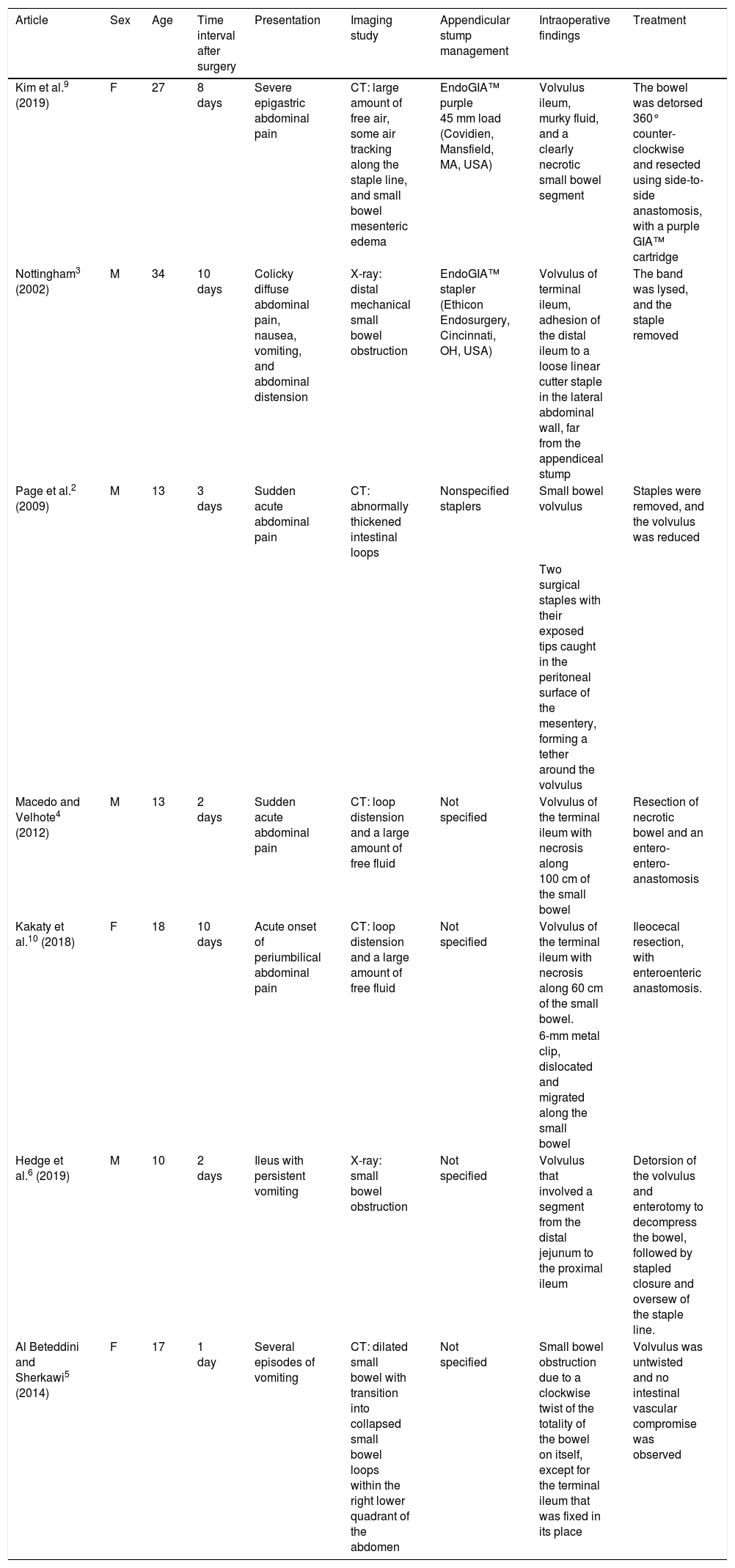
We cannot be sure of the exact mechanism of our patient’s volvulus. However, a few similar cases have been reported in the literature (Table 1). Page et al.2 and Nottingham3 described a 13-year-old patient and a 34-year-old patient, respectively, each of whom underwent laparoscopic appendectomy, employing a linear cutting stapler. They presented with abdominal pain on their third and tenth postoperative days, caused by SBV. In both cases, the volvulus was thought to be the result of a loose linear cutter staple in the abdominal cavity. In each case, the staple was caught in the peritoneal surface of the small bowel mesentery. Other theories of SBV after a laparoscopic appendectomy include patient positioning, inclination, bowel mobilization, and changes in the pneumoperitoneum. Nonetheless, those theories have not been well studied4. Similar to the two cases just described, we found a free staple snagged in the peritoneal surface of the small bowel mesentery, with no adhesion bands nearby. Given the widespread use of stapler/cutter devices, staples are likely becoming one of the most common foreign bodies in the abdominal cavity but only a few reports have described surgical staples causing adhesion-like complications, such as bowel obstruction or volvulus2.
Reported cases of small bowel volvulus, following laparoscopic appendectomy.
| Article | Sex | Age | Time interval after surgery | Presentation | Imaging study | Appendicular stump management | Intraoperative findings | Treatment |
|---|---|---|---|---|---|---|---|---|
| Kim et al.9 (2019) | F | 27 | 8 days | Severe epigastric abdominal pain | CT: large amount of free air, some air tracking along the staple line, and small bowel mesenteric edema | EndoGIA™ purple 45 mm load (Covidien, Mansfield, MA, USA) | Volvulus ileum, murky fluid, and a clearly necrotic small bowel segment | The bowel was detorsed 360° counter-clockwise and resected using side-to-side anastomosis, with a purple GIA™ cartridge |
| Nottingham3 (2002) | M | 34 | 10 days | Colicky diffuse abdominal pain, nausea, vomiting, and abdominal distension | X-ray: distal mechanical small bowel obstruction | EndoGIA™ stapler (Ethicon Endosurgery, Cincinnati, OH, USA) | Volvulus of terminal ileum, adhesion of the distal ileum to a loose linear cutter staple in the lateral abdominal wall, far from the appendiceal stump | The band was lysed, and the staple removed |
| Page et al.2 (2009) | M | 13 | 3 days | Sudden acute abdominal pain | CT: abnormally thickened intestinal loops | Nonspecified staplers | Small bowel volvulus | Staples were removed, and the volvulus was reduced |
| Two surgical staples with their exposed tips caught in the peritoneal surface of the mesentery, forming a tether around the volvulus | ||||||||
| Macedo and Velhote4 (2012) | M | 13 | 2 days | Sudden acute abdominal pain | CT: loop distension and a large amount of free fluid | Not specified | Volvulus of the terminal ileum with necrosis along 100 cm of the small bowel | Resection of necrotic bowel and an entero-entero-anastomosis |
| Kakaty et al.10 (2018) | F | 18 | 10 days | Acute onset of periumbilical abdominal pain | CT: loop distension and a large amount of free fluid | Not specified | Volvulus of the terminal ileum with necrosis along 60 cm of the small bowel. | Ileocecal resection, with enteroenteric anastomosis. |
| 6-mm metal clip, dislocated and migrated along the small bowel | ||||||||
| Hedge et al.6 (2019) | M | 10 | 2 days | Ileus with persistent vomiting | X-ray: small bowel obstruction | Not specified | Volvulus that involved a segment from the distal jejunum to the proximal ileum | Detorsion of the volvulus and enterotomy to decompress the bowel, followed by stapled closure and oversew of the staple line. |
| Al Beteddini and Sherkawi5 (2014) | F | 17 | 1 day | Several episodes of vomiting | CT: dilated small bowel with transition into collapsed small bowel loops within the right lower quadrant of the abdomen | Not specified | Small bowel obstruction due to a clockwise twist of the totality of the bowel on itself, except for the terminal ileum that was fixed in its place | Volvulus was untwisted and no intestinal vascular compromise was observed |
CT: computed tomography; F: female; M: male.
Diagnosis can be made through several modalities. For instance, a plain abdominal X-ray can appear normal, or reveal some bowel distension. Our patient’s initial x-ray revealed no abnormalities. Ultrasound has been previously used in the pediatric population to identify duodenal obstruction with SBV5. However, that imaging study is somewhat vulnerable due to the dependence on operator experience. A CT scan can detect the whirlpool sign, which is highly suggestive of intestinal volvulus, showing the twisting of the mesenteric vessels. However, the study’s sensitivity and specificity have not been evaluated6. In our case, the whirlpool sign was only seen in the sagittal view of the CT scan, and with the aid of a radiologist, we made the final diagnosis. The fact that the sign was not visible in the axial view made the diagnosis a challenge. Furthermore, a CT scan can be used to detect bowel infarction or ischemia (bowel-wall thickening or pneumatosis), so the study is more sensitive in the advanced stage of the disease. It can also be used to rule out other severe intra-abdominal diseases7.
In conclusion, we presented the case of a young adult patient that underwent laparoscopic appendectomy and presented with SBV, six days after his procedure. Even though we cannot be absolutely certain, we hypothesized that the volvulus resulted from a loose staple in the abdominal cavity that acted as a “hook” in the mesentery, causing rotation around its axis. As laparoscopic bowel stapling becomes more customary, there may be more reports of problematic staples that have been left in situ. We suggest removing all staples left in situ at the end of a laparoscopic procedure, to prevent any complication a loose staple could cause8.
Ethical considerationsProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Financial disclosureNo specific grants were received from public sector agencies, the business sector, or non-profit organizations in relation to this article.
Conflicts of interestThe authors declare that they have no conflict of interest.
Please cite this article as: González-Urquijo M, Quevedo-Fernández E, Morales-Morales CA, Alejandro-Rodríguez H, Leyva-Alvizo A. Vólvulo de intestino delgado tras apendicectomía laparoscópica. Revista de Gastroenterología de México. 2021;86:445–448.

