
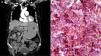
A 68-year-old woman with a stage III IgGκ multiple myeloma, according to the Revised International Staging System, was undergoing treatment with bortezomib, thalidomide, and dexamethasone, with partial response after 6 months of treatment. She arrived at the emergency service due to intense epigastric pain and tarry stools. An abdominal tomography scan with contrast revealed an irregular exophytic lesion at the level of the gastric body, with gastric overdistension (Fig. 1A). Endoscopic evaluation confirmed the presence of an ulcerated tumor with a diameter of 3 cm in the gastric body toward the greater curvature. Histopathologic and immunochemical analyses of the biopsies identified clonal plasma cell infiltration (Fig. 1B). The patient underwent distal gastrectomy and received two cycles of lenalidomide and dexamethasone as second-line regimen but presented with disease progression and died 6 months later.

A) Abdominal computed axial tomography image showing a vascularized solid vegetative tumor dependent on the internal edge of the greater curvature at the level of the gastric body, measuring 3.7 x 1.5 x 2.7 cm (black arrows). Enhancement of the gastric wall is observed after endovenous contrast administration. B) Photomicrograph of the gastric biopsy (magnification x100) with infiltration into the muscle layers and serosa by plasma cells with aberrant morphology. In the immunohistochemical study, the neoplastic cells showed diffuse positivity for cytoplasmic kappa light chains.
Gastrointestinal involvement in multiple myeloma occurs in less than 5% of cases and is associated with poor prognosis.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.

