


Upper gastrointestinal bleeding is a common problem that presents in the outpatient setting, as well as in the emergency service. The most common causes of this clinical entity are peptic ulcer disease, Mallory-Weiss tear, gastrointestinal neoplasias,1 and variceal bleeding in the case of patients with portal hypertension. Aneurysms of the lingual artery are infrequent. Aneurysms of the external carotid artery are estimated to account for 2.2% of all cervical carotid aneurysms. Among those, superficial temporal artery and facial artery aneurysms are the most common, whereas lingual artery aneurysms are rare. They only appear in the literature in case reports and their incidence cannot be determined.2 The majority of cases are pseudoaneurysms, associated with trauma, neoplasias, surgical procedures,3 or radiofrequency ablation.4 There are few cases of true idiopathic congenital aneurysms.
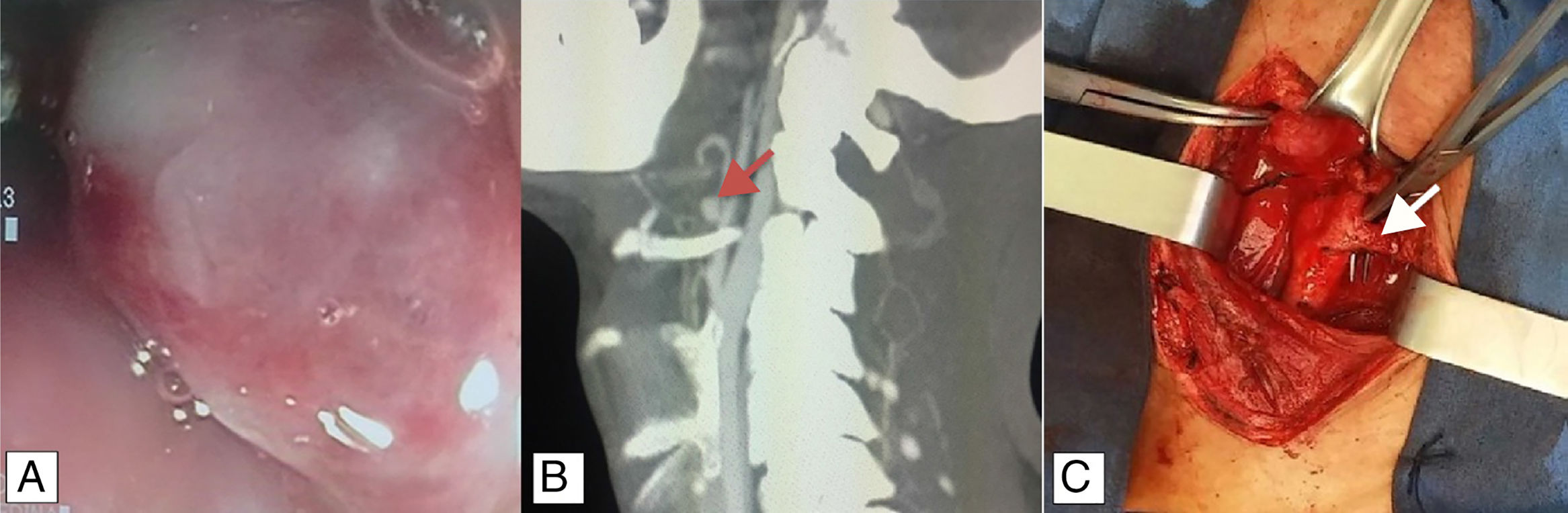
A 39-year-old man had a past medical history of appendectomy due to complicated appendicitis, as well as numerous symptoms of lower gastrointestinal bleeding from probable hemorrhoidal disease that were untreated. He was admitted to the hospital for 2-day progression of symptoms characterized by melena and hematemesis. Endoscopy was performed that identified: pulsatile, erythematous, and congestive polypoid tumoral lesion, 3 x 4cm in diameter, in the right posterolateral wall of the hypopharynx. There were no signs of active bleeding (fig. 1A), but fibrin-covered ulcers extended from the soft palate and proximal portion of the right piriform sinus. Twenty-four hours later, the patient presented with a new episode of bleeding. Angiotomography revealed a thickened hypopharynx and an irregular, right hypodense image, 21 x 17 x 17mm in diameter, at the level of the inferior constrictor muscle that protruded toward the lumen, obstructing 50% of it, with contrast medium leakage. A saccular image dependent on the aberrant artery was also observed that emerged from the trunk of the superior thyroid artery as a probable variant of the lingual artery (fig. 1B). After angiotomography, the patient presented with sudden onset of massive bleeding through the oral cavity. He became hemodynamically unstable, with AP of 48/30mmHg and MAP of 33mmHg. Carotid arteriography was performed (fig. 2A) that identified a 1.5-mm vessel at the level of the bifurcation that drains into the trachea above and to the right of the vallecula. Two sacs measuring approximately 5 and 8mm were observed along its tract. Failed embolization resulted in carrying out vascular examination of the neck with selective ligation of the first branch of the right external carotid artery (thyrolingual trunk) (fig. 1C). Bleeding control was adequate, and the patient was sent to the intensive care unit, where he underwent blood transfusion. His postoperative period was uneventful.
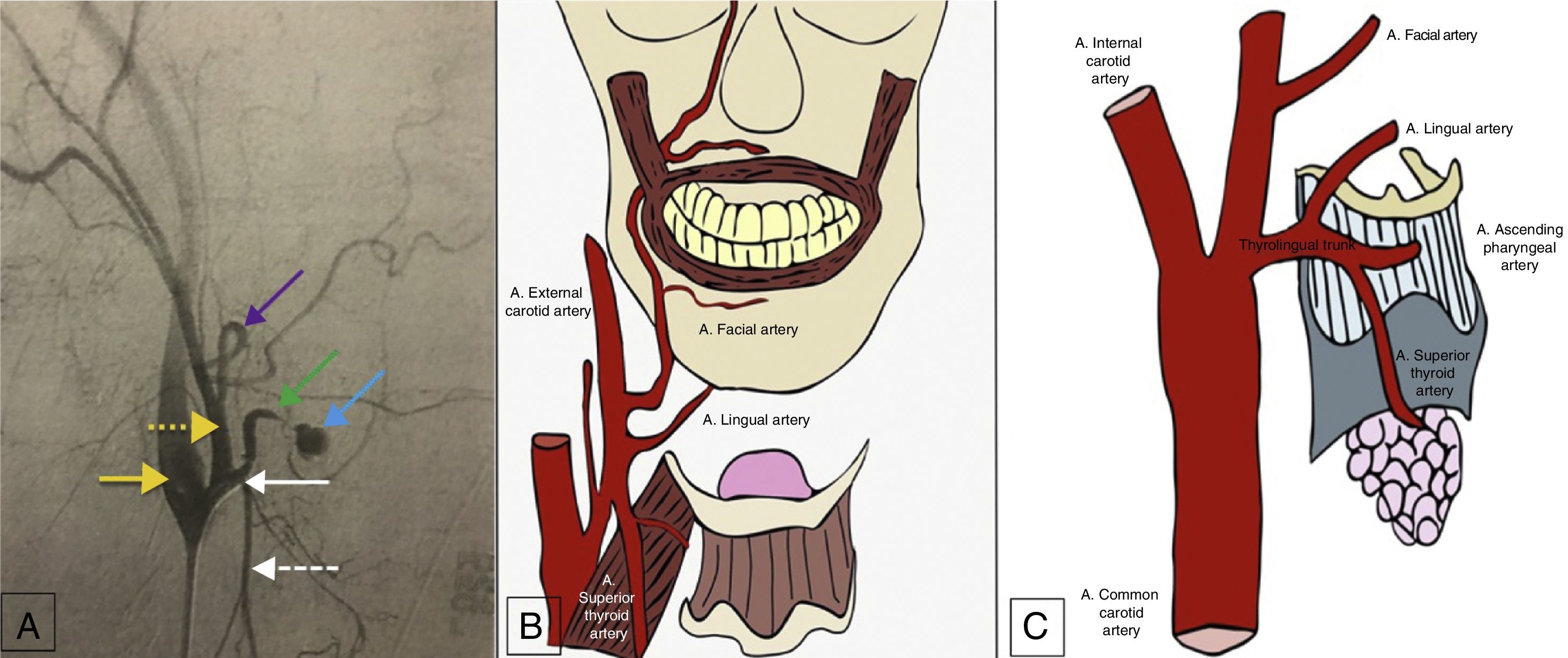
A) Arteriography. Yellow arrow: internal carotid artery; dotted yellow arrow: external carotid artery; purple arrow: facial artery; green arrow: lingual artery; blue arrow: aneurysm of the lingual artery; white arrow: thyrolingual trunk; dotted white arrow: superior thyroid artery. B) Most frequent anatomy of the branches of the external carotid artery. C) Thyrolingual trunk, seen in 0.99% of cases.
The clinical presentation of pseudoaneurysms generally involves upper gastrointestinal bleeding, whereas congenital aneurysms are asymptomatic, and so their diagnosis is usually made as an incidental radiologic finding from contrast-enhanced tomography of the cervical region.2 Upper gastrointestinal bleeding secondary to a pseudoaneurysm of the lingual artery is a potentially fatal event. The customary treatment reported in the literature is embolization through interventional radiology. The case presented herein was unusual in that it was a congenital aneurysm with a history of intermittent gastrointestinal bleeding. Finally, the patient presented with hemorrhagic shock, embolization was unsuccessful, and he then underwent surgical treatment with thyrolingual trunk ligation.
The right common carotid artery arises from the brachiocephalic trunk and the left common carotid artery from the aortic arch. After the posterolateral ascent within the carotid sheath, it divides at the level of the superior edge of the thyroid cartilage into the internal carotid artery and external carotid artery, which have a posterolateral and an anteromedial tract, respectively. They usually do not give off any branches in the neck. The eight habitual branches of the external carotid artery are: the superior thyroid artery, lingual artery, occipital artery, posterior auricular artery, maxillary artery, and superficial temporal artery.5 The lingual branch originates in the external carotid artery in 84.16% of cases. The majority (24.75%) arise between the superior thyroid artery and facial artery (fig. 2B) at the level of the hyoid bone and 14.85% form a common trunk with the facial artery. The lingual artery originates together with the superior thyroid artery in only 0.99% of cases (fig. 2C).6
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Ramírez-Ramírez MM, Clemente-Gutiérrez UE, Silva-González M, Zúñiga-Zamora HM, Sánchez-Conejo AR. Aneurisma congénito de la arteria lingual como causa inusual de sangrado de tubo digestivo alto. Revista de Gastroenterología de México. 2019;84:248–250.

